
Abstract
This study evaluated the step length–frequency relationship in physically active community-dwelling older women in order to investigate whether the relationship between these two spatio-temporal gait parameters changes with increasing age. Forty older women in four age groups, i.e. 64–69, 70–74, 75–79 and 80–85 year olds, participated in the study. Subjects walked at five different self-selected speeds and while simultaneously performing an additional cognitive and/or upper-extremity motor task. Gait parameters were determined from forward accelerations measured by a tri-axial accelerometer on the lower back. All subjects demonstrated a strong linear relationship between step length and step frequency for walking at different speeds. No evidence for a change in the step length–frequency relationship with age was found, suggesting that there are no differences between physically active older women of different age groups regarding the adoption of a “cautious gait”, i.e. a gait pattern characterized by a reduced step length.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Older people seem to walk with smaller step lengths compared to young adults (Kavanagh et al. 2004; Menz et al. 2003; Oberg et al. 1993). A gait pattern with reduced step length has specifically been observed in older people with Parkinson’s disease (Morris et al. 1994; Zijlstra et al. 1998), older patients with osteo-arthritis (van den Akker-Scheek et al. 2007; Hulet et al. 2000; McGibbon and Krebs 2002) and in older people with fall incidents (Richardson et al. 2005), or fear of falling (Aizen 2001; Nutt 2001).
A reduced step length, for a given gait speed, is often mentioned as a characteristic of “cautious gait” (Elble et al. 1992; Giladi et al. 2005; Nutt et al. 1993; Nutt 2001; Sudarsky 2006; Wall et al. 1991). A “cautious gait”, also termed “senile gait” (Bloem et al. 2000; Elble et al. 1992; Nutt et al. 1993), can be observed in real (e.g. slippery ice) or perceived conditions of balance-control difficulty and is often interpreted as an attempt to reduce the balance-control challenge during walking. “Cautious gait” has been observed in healthy older men (Murray et al. 1969), older people with fear of falling (Aizen 2001) and older people with neurological disorders, including vascular dementia, normal-pressure hydrocephalus, Alzheimer’s dementia and peripheral neuropathy (Elble et al. 1991). According to Elble et al. (1992) most of the kinematic changes that are associated with “senile gait” (e.g. increased double-limb stance, decreased maximum heel and toe displacement, reduced hip and knee rotations) are attributable to the reduced step length. Gait with reduced step length results in spending a proportionally longer time in the relatively stable periods of double-support and less in the more unstable single-support phase of the gait cycle (e.g. see Zijlstra et al. 1995, 1998).
At present, it is still unclear whether aging per se may lead to a “cautious gait” type or whether other factors are the primary causes. Other factors may be the effects of neuromusculoskeletal conditions, i.e. neurological diseases such as Parkinson’s disease, impairments of the joints or injuries to the muscles, or the effects of deconditioning. Impairments of the neuromusculoskeletal system, as well as psychological factors, may lead to a reduced level of physical activity which, by itself, may result in deconditioning and hence in altered movement patterns (Timiras 1994; Vorhies and Riley 1993). In dissociating possible age-effects from the effects of impairments of the neuromusculoskeletal system or deconditioning, it is important to know whether or not aging per se affects gait. Gait was therefore investigated in a sample of physically active community-dwelling older women. A population of women was chosen since women make up the larger part of the older population, and since women are nearly three times more likely than men to be hospitalized for a fall-related injury (Alexander et al. 1992).
In order to investigate whether aging has an effect on step length, the present study specifically focused on the relationship between step length and step frequency during walking at different speeds. As well as under undisturbed walking conditions, an alteration in the step length–frequency relationship may occur under conditions in which an additional task has to be simultaneously performed during walking. Some older people show optimal performance under undisturbed walking conditions, yet demonstrate abnormal gait under multiple-task conditions (Woollacott and Shumway-Cook 2002). An explanation may be that walking is attention demanding and that the attention demands increase with age (Woollacott and Shumway-Cook 2002). Walking under optimal conditions requires minimal attention. The attention requirements increase when additional tasks have to be performed simultaneously during walking. When walking is performed non-automatically, limited attention resources have to be divided between tasks. Gait changes under multiple-task conditions may therefore be the result of allocating insufficient attention resources to the walking task while prioritising performance on the additional task.
The relationship between step length and step frequency was investigated during undisturbed walking at different walking speeds as well as during walking while performing a simultaneous cognitive or upper-extremity motor task. It was expected that older women of different ages differ in the step length–frequency relationship.
Methods
Subjects
Subjects were recruited from recreative sports groups that aim to stimulate physical activities in older community-dwelling people. Subjects, who were not able to walk without a walking aid, e.g. cane or rolling walker, were excluded from participation, as well as subjects who had neuromusculoskeletal conditions that severely affect mobility.
After inclusion, each subject filled in a questionnaire in which details were obtained on health status, performance of functional tasks, experience of pain during mobility-related tasks, participation in recreational physical activities, history of falls during the last year, and the use of orthopedic footwear and walking aids during every day walking. In addition, subjects were asked whether they could hear properly without a hearing aid and in case of a negative answer they were asked whether they could hear properly with their hearing aid. The same was asked regarding vision and the use of glasses. Measurements of body mass, body height and leg length were made with subjects wearing their shoes. Leg length was measured as the distance between the anterior superior iliac spine (ASIS) and the floor. The local Ethics Committee approved of the study and subjects gave their written informed consent prior to participation.
Forty physically active community-dwelling older women in four age groups, i.e. 64–69, 70–74, 75–79 and 80–85 year olds, were included in the study. In each age group, ten subjects participated. Descriptive characteristics of the subjects are presented in Table 1. All subjects indicated that they could carry out different functional tasks, such as shopping, walking the stairs and domestic work. Thirty-one subjects indicated they could easily walk more than one kilometer and the other nine subjects mentioned they could walk more than 500 m. None of the subjects reported experiencing significant pain during performance of mobility-related tasks. Most subjects participated in more than one recreational physical activity, e.g. walking, cycling, swimming, gymnastics. Four subjects reported two or more falls and six subjects reported one fall in the previous year. One subject used a cane and another subject used a rolling walker during every day walking. All subjects had adequate vision and sense of hearing, with or without glasses and/or hearing aid.
Protocol
Subjects walked back and forth along a corridor in a public building. During a single walk, they walked 30 m, encircled a pylon and walked back to the starting point. Subjects walked wearing their regular shoes and wearing their usual clothing. Measurements were made without the use of a walking aid. Prior to the measurements, subjects were instructed not to make remarks or start a conversation during walking. Gait was measured at five different walking speeds. Speed instructions included walking on a “preferred”, “slow” or “even slower”, “fast” or “even faster” speed. The subjects performed two walks at the preferred speed and one walk for all remaining speeds. After walking at different speeds, subjects walked successively at a “preferred” and “fast” speed while simultaneously performing an additional cognitive task. Finally, subjects walked at a “preferred” speed while carrying, with both hands, a tray with a glass of water. The tray task was performed once without presenting the cognitive task and once while subjects simultaneously performed the cognitive task. Subjects were instructed not to spill any water. An auditive version of the Stroop task was used as cognitive task. The task consisted of presenting the words “high” and “low” randomly at a high or low tonal frequency with intervals of 2-s. Subjects had to respond verbally whether the words were pronounced at a high or low tone. To be able to compare multiple task performance with baseline performance, the cognitive task was first performed while sitting.
Data acquisition
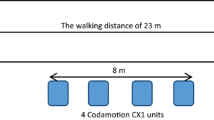
A tri-axial accelerometer (DynaPort MiniMod, McRoberts BV, The Hague, The Netherlands) was used to measure pelvic accelerations. The accelerometer was placed at the lower back of the subject with the center approximately at the level of the second sacral vertebrae. Size and mass of the sensor were 6.4 cm × 6.2 cm × 1.4 cm, and 75 g. The sensor was operated with a remote control, and data were stored locally on a secure digital (SD) memory card. Measurements were made with a sample rate of 100 Hz. During performance of the cognitive task, an additional observer recorded the given answers.
Data analyses
The middle 25 m of straight line walking during back and forth trajectories was used for an analysis of steady state walking (Lindemann et al. 2008). Mean walking speed was calculated for each of the 12 trajectories and was based on the distance and duration of a trajectory. Stride cycles were selected based on instants of foot contacts as determined from forward pelvic accelerations (Zijlstra 2004). Mean step length, mean step frequency and mean length/frequency-ratio (step length/step frequency-ratio) were calculated for each trajectory. Group means of walking speed, step length and frequency and length/frequency-ratio were determined using all available data. An individual linear regression equation between step length and step frequency was determined for each included subject. The individual regression equations were calculated using data of both forth and back trajectories of the 6 walks at the different walking speeds. Performance on the auditive Stroop task was indicated as a percentage of wrong answers. For each of the four gait parameters, the value determined for the multiple walking task (i.e. walking at preferred or fast speed with Stroop task, or walking with tray and Stroop task) was calculated as a percentage of the value determined for undisturbed walking. Also, the difference in percentage wrong answers on the Stroop task between when sitting and when performing the multiple walking task was calculated. To assess the multiple task interference effect on both walking performance and Stroop task performance, total scores of multiple task performance were determined by adding the percentage calculated for one of the gait parameters to the percentage calculated for the Stroop task.
Statistical analyses
Paired t-tests were performed to determine whether significant differences existed between back and forth trajectories in walking speed, step frequency, step length and linear regression equation variables. In addition, Pearson’s correlation coefficients between back and forth trajectories were calculated. One-way analyses of variance (One-Way ANOVA’s) and Kruskal–Wallis tests were used to investigate whether main effects of age group existed. Subsequently, Bonferonni multiple comparisons tests were used to identify which pairs of age groups differed. Correlations with age were investigated by calculating Pearson’s correlation coefficients. Paired t-tests were performed to determine whether significant differences existed between undisturbed walking and walking while simultaneously performing additional tasks. Subjects who reported one or more falls during the last year were age-matched to subjects who did not report falls, and differences between the two groups were investigated using Mann–Whitney tests. Mann–Whitney tests were performed for body weight and height, leg length, walking speed, step frequency and length, length–frequency ratio, linear regression equation variables and for all parameters that were determined during walking while performing additional tasks. All analyses were performed at a significance level of 0.050.
Results
No significant differences between back and forth trajectories were found in walking speed, step frequency and step length. In addition, Pearson’s correlation coefficients between back and forth trajectories were high (i.e. >0.80). Therefore, data of both back and forth trajectories were used in the analyses.
Walking at different speeds
For all five walking speed conditions, main effects of age group were observed for walking speed, step length and frequency (Kruskal Wallis tests, P < 0.009, Table 2). The post-hoc revealed that the 80–85 year olds walked with lower walking speeds compared to the other three age groups (Bonferonni, P < 0.026). In addition, the 80–85 year olds had lower step lengths compared to the other three age groups for walking at a slow, preferred, fast and even faster speed (Bonferonni, P < 0.005). For walking at the slowest speed condition, the 80–85 year olds had lower step lengths compared to only the 70–74 and 75–79 year olds (Bonferonni, P < 0.003). Step frequencies were lower for the 80–85 year olds compared to the other three age groups for walking at a preferred, fast and even faster speed (Bonferonni, P < 0.049). For walking at a slow and even slower speed, the 80–85 year olds had lower step frequencies compared to only the 64–69 and 70–74 year olds (Bonferonni, P < 0.007). Maximum and minimum values of walking speed, step frequency and step length decreased with age (see Fig. 1). Pearson’s correlations with age were significant for maximum and minimum values of walking speed and step frequency (P < 0.018), and for maximum values of step length (P = 0.003).

Minimum (white dots) and maximum (black dots) values of walking speed (a), step frequency (b) and step length (c) for the different ages of the 40 physically active community-dwelling older women. The Pearson’s correlation coefficient (R) between the maximum values and age is indicated at the top of the figure and the Pearson’s correlation coefficient (R) between the minimum values and age is indicated at the bottom of the figure
For the length/frequency-ratio, main effects of age group were demonstrated for walking at a slow, even slower and preferred speed (Kruskal Wallis tests, P < 0.002, Table 2). The post-hoc revealed that the 75–79 year olds had larger length/frequency-ratios compared to the other three age groups (Bonferonni, P < 0.010). Pearson’s correlations between length/frequency-ratio and age were not significant.
Results for the regression equation variables, classified into four age groups, are presented in Table 3. Within age groups, a large variation existed in the intercept of the regression equation. Some variation also existed in regression coefficient. Mean correlation coefficients and coefficients of determination were high (i.e. >0.80). Main effects of age group were observed for both the intercept and regression coefficient (Kruskal Wallis tests, P < 0.039, Table 3). The post-hoc revealed that the 75–79 year olds had a larger intercept (Bonferonni, P = 0.005) and a smaller regression coefficient (Bonferonni, P = 0.027) than the 64–69 year olds. Pearson’s correlations between regression equation variables and age were not significant.
Walking with additional tasks
A significant difference between subjects with reported falls and age-matched subjects without reported falls existed in the difference of scores on the auditive Stroop task when sitting compared to when walking while carrying a tray with a glass of water (Mann–Whitney test, P < 0.028). In addition, a significant difference existed in the total score of multiple task performance, with walking speed as gait parameter, during walking at a fast speed (Mann–Whitney test, P < 0.036).
Table 4 shows the results for the total group of older women. The sample of older women demonstrated a significantly decreased walking speed, step length and step frequency when walking at a preferred speed while simultaneously performing the Stroop task compared to undisturbed walking. In addition, the percentage of wrong answers on the Stroop task was significantly higher when walking at a preferred or fast speed compared to when sitting.
Walking while carrying a tray with a glass of water resulted in a decreased step length, an increased step frequency and a decreased length/frequency-ratio compared to undisturbed walking. Walking with tray task while also performing the Stroop task resulted in a decreased walking speed, step length and length/frequency-ratio compared to undisturbed walking. In addition, subjects made significantly more mistakes on the Stroop task when walking with tray task compared to when sitting.
No main effects of age group were demonstrated for multiple task interference effects on walking performance, Stroop task performance and on total scores of multiple task performance. A significant correlation with age (P = 0.024) was found only for the interference effect on step length when walking while performing additional tray and Stroop tasks (Pearson’s correlation coefficient = −0.36).
Discussion
This study aimed to analyze whether or not older women develop a “cautious gait” type with increasing age. To separate the effects of age per se from the effects of severe age-related neuromusculoskeletal conditions and/or deconditioning due to a sedentary life style, only physically active community-dwelling older women were included. Since a reduced step length is mentioned as a main characteristic of “cautious gait” (Elble et al. 1992; Giladi et al. 2005; Nutt et al. 1993; Nutt 2001; Sudarsky 2006; Wall et al. 1991), the present study focused on age-related changes of the step length–frequency relationship during undisturbed walking at different walking speeds as well as during walking while performing a simultaneous cognitive or upper-extremity motor task.
Although the results of the present study show that the observed minimum and maximum values (i.e. ranges) of walking speed, step length and step frequency decrease with increasing age, no age-effects on the step length–frequency relationship were demonstrated. The findings indicate that the step length–frequency relationship was independent of age within the studied sample of physically active, community-dwelling older women, even when the older women performed additional tasks during walking. Thus, it seems that the physiological and psychological changes that are associated with aging do induce an older person to walk slower, however, they do not induce a change in the step length–frequency relationship. This implies that “cautious gait” is caused by an underlying pathology and/or by decreased physical activity. This notion is supported by Giladi et al. (2005) and Bloem et al. (2000) who identified possible disease-related causes for the adoption of a “cautious gait” pattern in groups of older patients with “senile gait” disorder. Based on their results, Giladi et al. and Bloem et al. claim that it is likely that the gait changes in older adults who walk with a “cautious gait” pattern, are a marker of underlying pathology and not a consequence of age-related processes.
An unexpected result of the present study is that the group of 75–79 year olds, in comparison to the other age groups, showed larger step lengths during walking at the slowest speeds. An evaluation of anthropometric characteristics and other descriptors such as activity level and number of reported falls revealed no clear differences between the 75–79 year olds and the other age groups. It is therefore unclear why the 75–79 year olds showed deviating results for step length.
Contrary to the findings in the present study, a large scale study by Nagasaki et al. (1996) did demonstrate a relationship with age of the step length/step frequency-ratio in community-dwelling older people. During walking at a preferred and at a maximum speed, the older people in the study by Nagasaki et al. walked with steps that tended to shorten with age. The difference in findings can be explained by the difference in sample characteristics. Contrary to the present study, Nagasaki et al. included a random sample of people over 65 years old, not specifying whether or not subjects with neuromusculoskeletal conditions that affect mobility were excluded. The decrease in ratio with age in the study by Nagasaki et al. may therefore have been caused by a larger proportion of subjects with pathology and/or a sedentary life style in the oldest age groups.
The inclusion criterium of participation in recreative sports groups for community-dwelling older women resulted in a group of older women who were predominantly non-frail and physically active. However, besides excluding older women who were not able to walk without walking aid and women who had neuromusculoskeletal conditions that severely affected mobility, no further exclusion criteria were applied. Conditions that can mildly affect mobility were not excluded since exclusion of these conditions would have resulted in a very selective group of older women, not representative of the target population of physically active community-dwelling older women. Due to the broad inclusion criteria, the studied sample included subjects with cardio-vascular and respiratory conditions, diabetes, incidental dizziness, Meniére’s disease, osteoporosis and diseases of the joint(s). The effect of these conditions on gait, however, was assumed to be minimal since all subjects indicated that they were able to carry out functional tasks in and around their homes, participated in recreational physical activity and did not experience pain during performance of mobility-related tasks. In addition, most subjects indicated that they were able to walk more than 1 km and the other subjects reported that they were able to walk more than 500 m.
Sekiya et al. (1997) and Sekiya and Nagasaki (1998) determined the step length/step frequency-ratio in healthy young women with mean ages of 21 and 23 years respectively. At similar walking speeds, the length/frequency-ratio of young women was systematically larger than of the older women in the present study. Thus, although no development in the step length–frequency relationship with age was demonstrated in women aged 65 or older, a difference in stepping patterns does exist between aged and young women. Possibly, the difference is caused by a reduction of lower-extremity muscle strength in older women in combination with a difference in physical activity that may be expected between young and older women. More data is needed to determine at which age range older women develop a decrease in step length.
Multiple task interference effects were demonstrated for the total group of older women. The interference effects imply that attention resources were limited in the studied group of older women and/or that the allocation of attention resources to the different tasks was affected. However, an interference effect on the step length/step frequency-ratio existed only for task situations in which subjects carried a tray with a glass of water. During walking while simultaneously performing the auditive Stroop task, the older women merely reduced gait speed and did not reduce step length. Apparently, the physically active older women were also not inclined to adopt a “cautious gait” during walking situations with added cognitive difficulty. During walking with tray task, all subjects managed to walk back and forth without spilling any water. However, subjects did change their stepping patterns. The reduced step length that was observed during walking with tray task most likely was induced by the need to adequately perform the added motor component. By reducing step length the peak accelerations at the level of the trunk become smaller (cf. see inverted pendulum models and data as described by Zijlstra and Hof (1997), thus decreasing the effort to stabilize the tray.
The presented data suggest that, in the absence of severe pathological conditions or a sedentary life style, the mechanisms underlying the production of stepping patterns in older women remain unaltered with increasing age. However, more data is needed to properly address the latter issue. The data presented in this paper give a fair indication of walking patterns in physically active older Dutch women and may be used for comparing normal gait with pathological gait or gait in “frail” older women. To our knowledge, the present study is the first to report data on the linear regression between step length and step frequency of older women. Based on the results, the linear regression equation variables seem suitable parameters for describing stepping patterns in older women. For all subjects, a strong linear relationship between step length and step frequency existed for walking at different speeds. Sekiya and Nagasaki (1998) already demonstrated the test-retest reliability of the step length/step frequency-ratio in young adults and suggested the ratio as a reliable measure for evaluating aging walking patterns. The results of the present study demonstrate that aging processes per se do not influence the relationship between step length and step frequency. Changes in the step length–frequency relationship may therefore be useful in identifying pathological gait.
Conclusion
The results of the present study do not indicate systematic changes of the step length–frequency relationship with age in physically active community-dwelling older women. Even in complex situations in which one or more tasks are to be performed simultaneously during walking, older women of different ages do not differ in multiple task interference effects on the step length–frequency relationship. Thus, the results imply that aging processes per se are not responsible for the tendency of some older women to walk with reduced step length, or to walk with longer periods of double limb support in attempting to reduce the balance-control challenge during walking.
References
Aizen E (2001) Cautious gait and fear of falling in the elderly. Harefuah 140:1091–1115
Alexander BH, Rivara FP, Wolf ME (1992) The cost and frequency of hospitalization for fall-related injuries in older adults. Am J Public Health 82:1020–1023
Bloem BR, Gussekloo J, Lagaay AM et al (2000) Idiopathic senile gait disorders are signs of subclinical disease. J Am Geriatr Soc 48:1098–1101
Elble RJ, Thomas SS, Higgins C, Colliver J (1991) Stride-dependent changes in gait of older people. J Neurol 238:1–5. doi:10.1007/BF00319700
Elble RJ, Hughes L, Higgins C (1992) The syndrome of senile gait. J Neurol 239:71–75. doi:10.1007/BF00862975
Giladi N, Herman T, Reider-Groswasser II et al (2005) Clinical characteristics of elderly patients with a cautious gait of unknown origin. J Neurol 252:300–306. doi:10.1007/s00415-005-0641-2
Hulet C, Hurwitz DE, Andriacchi TP et al (2000) Functional gait adaptations in patients with painful hip. Rev Chir Orthop Reparative Appar Mot 86:581–589
Kavanagh JJ, Barrett RS, Morrison S (2004) Upper body accelerations during walking in healthy young and elderly men. Gait Posture 20:291–298. doi:10.1016/j.gaitpost.2003.10.004
Lindemann U, Najafi B, Zijlstra W et al (2008) Distance to achieve steady state walking speed in frail elderly persons. Gait Posture 27:91–96. doi:10.1016/j.gaitpost.2007.02.005
McGibbon CA, Krebs DE (2002) Compensatory gait mechanics in patients with unilateral knee arthritis. J Rheumatol 29:2410–2419
Menz HB, Lord SR, Fitzpatrick RC (2003) Age-related differences in walking stability. Age Ageing 32:137–142. doi:10.1093/ageing/32.2.137
Morris ME, Iansek R, Matyas TA, Summers JJ (1994) The pathogenesis of gait hypokinesia in Parkinson’s disease. Brain 117:1169–1181. doi:10.1093/brain/117.5.1169
Murray MP, Kory RC, Clarkson BH (1969) Walking patterns in healthy old men. J Gerontol 24:169
Nagasaki H, Itoh H, Hashizume K, Furuna T (1996) Walking patterns and finger rhythm of older adults. Percept Mot Skills 82:435–447
Nutt JG (2001) Classification of gait and balance disorders. Adv Neurol 87:135–141
Nutt JG, Marsden CD, Thompson PD (1993) Human walking and higher-level gait disorders, particularly in the elderly. Neurology 43:268–279
Oberg T, Karsznia A, Oberg K (1993) Basic gait parameters: reference data for normal subjects, 10–79 years of age. J Rehabil Res Dev 30:210–223
Richardson JK, Thies SB, DeMott TK, shton-Miller JA (2005) Gait analysis in a challenging environment differentiates between fallers and nonfallers among older patients with peripheral neuropathy. Arch Phys Med Rehabil 86:1539–1544. doi:10.1016/j.apmr.2004.12.032
Sekiya N, Nagasaki H (1998) Reproducibility of the walking patterns of normal young adults: test-retest reliability of the walk ratio (step-length/step-rate). Gait Posture 7:225–227. doi:10.1016/S0966-6362(98)00009-5
Sekiya N, Nagasaki H, Ito H, Furuna T (1997) Optimal walking in terms of variability in step length. J Orthop Sports Phys 26:266–272
Sudarsky L (2006) Psychogenic gait disorders. Semin Neurol 26:351–356. doi:10.1055/s-2006-945523
Timiras PS (1994) Disuse and aging: same problem, different outcomes. J Gravit Physiol 1:5–7
van den Akker-Scheek I, Stevens M, Bulstra SK et al (2007) Recovery of gait after short-stay total hip arthroplasty. Arch Phys Med Rehabil 88:361–367. doi:10.1016/j.apmr.2006.11.026
Vorhies D, Riley BE (1993) Deconditioning. Clin Geriatr Med 9:745–763
Wall JC, Hogan DB, Turnbull GI, Fox RA (1991) The kinematics of idiopathic gait disorder. A comparison with healthy young and elderly females. Scand J Rehabil Med 23:159–164
Woollacott M, Shumway-Cook A (2002) Attention and the control of posture and gait: a review of an emerging area of research. Gait Posture 16:1–14. doi:10.1016/S0966-6362(01)00156-4
Zijlstra W (2004) Assessment of spatio-temporal parameters during unconstrained walking. Eur J Appl Physiol 92:39–44. doi:10.1007/s00421-004-1041-5
Zijlstra W, Hof AL (1997) Displacement of the pelvis during human walking: experimental data and model predictions. Gait Posture 6:249–262. doi:10.1016/S0966-6362(97)00021-0
Zijlstra W, Rutgers AW, Hof AL, Van Weerden TW (1995) Voluntary and involuntary adaptation of walking to temporal and spatial constraints. Gait Posture 3:13–18. doi:10.1016/0966-6362(95)90804-2
Zijlstra W, Rutgers AW, Van Weerden TW (1998) Voluntary and involuntary adaptation of gait in Parkinson’s disease. Gait Posture 7:53–63. doi:10.1016/S0966-6362(97)00037-4
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Zijlstra, A., de Bruin, E.D., Bruins, N. et al. The step length–frequency relationship in physically active community-dwelling older women. Eur J Appl Physiol 104, 427–434 (2008). https://doi.org/10.1007/s00421-008-0795-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-008-0795-6