
Abstract
Influenza surveillance is usually based on nationally organized sentinel networks of physicians and on hospital reports. This study aimed to test a different report system, based on parents’ phone contact to the research team and in home collection of samples by a dedicated team. The identification of influenza and other respiratory viruses in children who attended a Hospital Emergency Department was also recorded. Real-time PCR and reverse transcription PCR were performed for influenza A and B, parainfluenza 1-4, adenovirus, human metapneumovirus, respiratory syncytial virus A and B, rhinovirus, enterovirus, group 1 coronaviruses, group 2 coronaviruses, and human bocavirus. One hundred children were included, 64 from the day care centers and 36 from the Hospital. Overall, 79 samples were positive for at least one respiratory virus. Influenza A (H3) was the virus most frequently detected: 25 cases, 20 of these in children under 5 years of age (ten from day care centers and ten who went to the hospital) which was higher than those reported by the National Influenza Surveillance Programme for this age. Conclusion: The results obtained in this study suggest that a surveillance system based on parents’ reports could complement the implanted system of the National Influenza Surveillance Programme.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Acute respiratory infections have globally the highest mortality in children and are estimated that about five million children under five die annually with viral respiratory infections [12]. These infections account not only for increased mortality but also for increased morbidity in this age group, being responsible for about one quarter and up to half, respectively, of all hospitalizations and general practitioner consultations in European countries during the winter, besides the considerable impact they have on parents’ quality of life [2, 18].
In the northern hemisphere, influenza viruses continue to be a major cause of respiratory tract infection during epidemic periods that occur usually in winter, despite the recommended vaccine schedule every year. In children, influenza vaccination is not a common practice, although the use of live influenza vaccines in this age group seems promising to reduce the annual impact of this infection [1]. An efficient surveillance system for the detection of influenza infections in children will be, therefore, desirable in order to check for vaccine efficacy.
Given these important impacts of seasonal influenza epidemics and the always present threat of a new influenza pandemic, public health surveillance systems, which routinely collect information on the disease incidence and genetic and antigenic viral characterization, have been implemented since the 1950s. Usually, these systems are based mainly on nationally organized sentinel networks of physicians, covering at least 1 to 5 % of the population in their countries, and on hospital reports of clinically suspected or laboratory-confirmed influenza cases [5]. In Portugal, the National Influenza Surveillance Programme aims to collect, analyze, and disseminate information on influenza activity, identifying and characterizing influenza virus in circulation in each season, as well as performing the identification of emerging viruses with pandemic potential that pose a risk to public health. In this way, it seeks to contribute to decrease the morbidity and mortality associated with infection and its complications. The data from the National Influenza Surveillance Programme also allow orientation for prevention and control of influenza. The surveillance programme integrates the clinical and virological component enabling: (1) to estimate the morbidity of the disease through determining the weekly incidence rates of influenza-like illness and identification of outbreaks in population under observation; (2) identify and characterize the virus influenza strains circulating and quantify their presence in the population under observation, during the period of influenza activity; (3) through the information gathered and after its evaluation, promote intervention at health services in actions for prevention and therapy advising. The information and biological samples for laboratorial diagnosis came from the general practitioner network and from emergency units that are located in Portugal mainland, Azores and Madeira islands [10, 16].
However, this and other similar systems imply a general practitioner, pediatrician, or hospital consultation, requiring child’s exit from home in epidemic period, with potential virus transmission to and from other children. Therefore, an additional surveillance system to avoid this outdoor consultation could be an interesting approach, keeping the registry of influenza activity but potentially reducing transmission. This direct approach to the population could also avoid some bias on the registry, since medical consultations will probably receive more serious cases and are also very dependent on parental anxiety.
The project “Environment and Health in children day care centers” (ENVIRH), where this study is nested, is a multidisciplinary project with the purpose of studying the health impact of indoor air environment in children in day care centers. One of the key points of this project was the study of the role of viral respiratory infections at day care center level, particularly influenza. To accomplish this, the study included parents’ phone contact to the research team whenever a child had symptoms of respiratory infection, in order to collect respiratory samples for virology analysis. The main objective of this study was to test the compliance of the parents to this report system and to see if this strategy would improve the detection, in preschool children, during epidemic periods, when compared with current surveillance systems for influenza. The detection of other circulating respiratory viruses was the second objective of the study.
In the second year of the study, the circulating viruses at day care centers were compared with the detected viruses in children who attended a Hospital Emergency Department with respiratory infections. This Hospital approach would also test influenza detection by an Emergency Department team and would allow comparison with the results of the National Program, which also includes several hospitals.
Material and methods
Study design
The study included ten day care centers in Lisbon, selected by the ENVIRH team, through a cluster analysis, in the second phase of the project, according to the concentrations of CO2, temperature, and humidity, in the indoor air (data not presented). Parents were informed of the project both by open sessions, realized in all day care centers and conducted by a virologist of the ENVIRH team, and by a leaflet distributed to all parents. In these open sessions, a brief review of the importance of the respiratory infections in children was provided, with a special emphasis on the epidemiology of influenza infections. Parents were invited to participate in the study by calling to the ENVIRH team (a free call by a dedicated line) whenever their children presented at least two of the following clinical signs: fever, wheezing, cough, or nasal congestion. Parents’ informed consents were obtained, and the study was approved by the Ethics Committee of Nova Medical School, Lisbon. The clinical evolution was sought by a phone call to the parents some weeks after the specimen collection.
The study was performed in two periods, from February to May 2011 and from November 2011 to April 2012. The first period, partially covering the 2011 winter and spring, was intended to be an experimental period to check for the parents’ interest in this project and the feasibility of the alert system implemented with the study.
In the second period, along with the samples collected at home, children attending the Emergency Department of the Hospital da Luz, with the same clinical signs mentioned above, were also included.
Data from influenza activity
Data collected from the National Influenza Surveillance Programme for the winter 2011/2012 was used for comparison with the results obtained with the surveillance system tested in this study [10].
Biological samples
Two swabs were collected from each child, nasopharyngeal and oropharyngeal, and immediately pooled into viral transport medium (Vircell's Transport Medium for virus, Chlamydia and Mycoplasma).
Regarding the children from day care centers, samples were collected at their homes, after parents’ call to the ENVIRH team, within the first 48 h after the beginning of the clinical signs.
At the hospital, swabs were collected from children who were admitted with respiratory tract infection. Parents were informed about the study and asked to participate.
Virological methods
Nucleic acid extraction
Viral nucleic acid was extracted using the “EZ1 Virus mini Kit v2.0” according to the manufacturer’s instructions. A starting volume of 400 μL was used to elute 60 μL of viral RNA/DNA, and 5 mL of this eluate was used for each PCR reaction, with a 25-μL final reaction volume.
PCR for respiratory viruses
The quadriplex influenza A/B/H5 real-time PCR assay that includes an internal control (bacteriophage MS2) has been detailed elsewhere [4, 9]. Three additional multiplex real-time (Taqman) PCR assays were employed to detect the following respiratory viruses: respiratory syncytial virus (RSV) A and B, parainfluenza (PIV) types 1/3 and adenovirus (panel 2), enterovirus, rhinovirus, human metapneumovirus (hMPV) and PIV types 2/4 (panel 3), and group 1 coronaviruses (HCoV-229E and HCoV-NL63) and group 2 coronaviruses (HCoV-OC43 and HCoV-HKU1) (panel 4) [3, 6, 17]. Superscript™ III Platinum one-step Invitrogen enzyme (Cat.No. 11732-088) was used for the reverse transcription and subsequent PCR amplification step—0.8 μL of enzyme per 25-μL volume PCR reaction. All assays shared identical amplification conditions (50 °C for 30 min, 95 °C for 2 min, 45 cycles at 95 °C for 15 s, and 60 °C for 1 min), allowing all four panels to run simultaneously on the same instrument. Primer and probe sequences and concentrations for multiplex panels 2 to 4 and for the monoplex bocavirus assay are available on request from the authors. Amplification reactions and detection of PCR products were performed using the Rotorgene™ PCR system acquiring the fluorescence on FAM, JOE, CY5, and ROX channels at each cycle. Samples and negative control (molecular grade water) were individually spiked with MS2 bacteriophage internal control (4,600 pfu per extraction) prior to nucleic acid extraction to identify any inhibitors. Positive controls for all panels were made from a combination of recombinant plasmids and from known positive specimens, diluted to give a cycle threshold value of 20–25. Negative controls were extracted molecular grade water.
Results
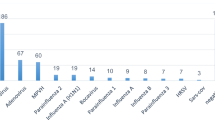
A total of 764 children, from ten day care centers, had parents’ permission to participate in the study, but only 64 from eight centers reported respiratory symptoms to the study team. Additionally, 36 children from the Hospital were also included in the second period. Therefore, a total of 100 children were included, all but three were under 5 years of age, the exceptions being three children of the same day care room, who were 7 years old. Overall, 79 samples were positive for at least one respiratory virus, 62 for a single agent and 17 for two or more viruses. Influenza A (H3) was the virus most frequently detected (22 positive samples), followed respectively by hMPV, rhinovirus, adenovirus, enterovirus, human bocavirus, PIV 1/3, RSV, group 1 coronavirus, influenza B, group 2 coronavirus, and PIV 2/4 (Table 1).
The distribution by year and locality of sample collection (day care center or Hospital) is also represented in Table 1. In this table and in the second period of the study, some differences between the two populations can be observed, concerning the frequency of the different viruses, but the low number of positive samples for each virus is insufficient to draw conclusions. The only exceptions were the adenovirus, detected more frequently at the hospital (p = 0.007; Fisher’s exact test).
In the second period of the study and due to the worsening of the clinical situation, eight children of the day care group went to an Emergency Department of a hospital in the Lisbon area, five with influenza infection (four A and one B), one with a rhinovirus infection and two with viral negative results, but none was hospitalized.
In the group of children who went to the Emergency Department of the Hospital da Luz, 6 out of 36 were hospitalized, two with an adenovirus infection, one with an influenza A infection, one with a metapneumovirus infection, one with a rhinovirus, and one with viral negative result.
Influenza activity
The first case positive for influenza, in day care children and at the hospital, was respectively on weeks 9 (28th of February 2012) and 7 (14th of February 2012).
This project detected 25 cases of influenza infection, 20 of these under 5 years of age and all of them positive for influenza A (the three influenza B cases were detected in older children of the same day care room and these were the exceptions described above). When comparing with the report from the National Influenza Surveillance Programme, it can be observed that the number of detected cases by the project in children under five (0–4) was higher than the cases reported by the National Programme; actually, 10 out of the 11 positive cases at the day care centers were in children under five, and the same result was obtained with the samples collected at the Hospital (10/11 positive samples), while the National Programme detected only five cases in this age group.
Discussion
The primary objective of this study was to test a surveillance system for respiratory infections in children and to check if parents’ collaboration, coupled with a sample collection by a dedicated team, could add important information to that obtained from the National Programme for Flu Surveillance.
Looking into the data from the 2011/2012 report of the National Influenza Surveillance Programme [10], it can be observed that the number of cases from the group of children under five was low, which contrasts with the concept that children have an important role in the dissemination of influenza viruses during epidemics. One possible explanation could be the operation mode of the National Programme, mainly based in general practitioners, working voluntarily as sentinel physicians for the sending of respiratory samples. In Portugal, many parents prefer to consult pediatricians, instead of the general practitioners, which may have contributed to the lower representation of children under five.
In this study, even with a low parents’ compliance (the number of reported infections was below the expected number of respiratory infections for the population under study: 64 reported infections for a population of 764 children with parents’ permission to participate), the approach used was more effective than the National Programme in detecting influenza infections in these younger children. In fact, the current project detected ten cases in children from the day care centers, while the National Programme had only five confirmed infections. Interestingly, ten additional cases were detected at the Hospital da Luz (a private hospital), suggesting that few parents consulted the Emergency Departments of the National health system that collaborate in the influenza surveillance programme, during this season, or not all cases were swabbed for laboratory diagnosis.
Therefore, a surveillance system at day care centers could complement the implanted system of the National Influenza Surveillance Programme, providing an increased representation of pediatric samples and the respective viral isolates, and avoiding unnecessary outdoor consultations. At a first glance, this may seem rather difficult to achieve, since it demands a sample collection at home by a laboratory technician, every time a call is received for notification. However, it should be emphasized that all the collections of the current work were easily performed by a single technician, covering a population of 764 children, within the first 48 h after the call. Naturally, would parents’ adherence be better, one technician could be insufficient to cover all the calls, but even with this level of parents’ cooperation, the results were promising, as previously described. Another adding value of this system is the fact that, being more a population based than the actual health service based system, it allows the coverage of influenza cases that do not recur to a health care center or hospital. Nevertheless, it is important to state that these results are based only in one season, and that although promising, the continuous evaluation of the day care centre system, in other seasons, with the predominance of other influenza viruses, with different levels of intensity and epidemic period durations is necessary.
Another interesting approach, with the same objectives (being a population-based system and avoiding unnecessary outdoor consultations), used parent-collected specimens with promising results [13]. This system would have the obvious advantage of sparing the research staff for the home collections, but other disadvantages, such as the quality of specimen collection (despite another paper of the same author stating that parents’ collections have similar quality [14]) or the associated costs with the swabs distribution and the fast transport back to the laboratory should also be taken into consideration. Moreover, in this study, the possibility of the research staff to visit the home to assist with or perform specimen collections was available when required. Anyway, this one or a similar system could be another alternative to complement the flu surveillance in pediatric ages.
In the first year of the project, there were no influenza detections, which are explained by the fact that the project started in February 2011, after the flu epidemic of that year. Therefore, no comparison with the National Programme could be done in this first year.
Concerning the second objective of this study, the identification of the viruses responsible for respiratory infections that do not require hospital attendance, we may observe that all the viruses were detected in at least one of the years. Therefore, these results are in agreement with previous published papers, where the use of sensitive molecular biology techniques detects the circulation in the community of the great majority of the described respiratory viruses [7, 8, 11, 15]. As it can be seen from the results, despite this approach being primarily described for influenza surveillance, it can identify the circulation of other viruses as well. This may bring useful epidemiological and clinical information, for instance in identifying early RSV circulation. Parents’ reports were based on the detection of common and unspecific respiratory symptoms, and therefore, this system can detect all the viral respiratory infections and not exclusively influenza.
In this work, viruses were detected in more than two thirds of the respiratory infections in children not attending the hospital (47/64), a rate not statistically different from the hospital rate (32/36). This difference can be even lower, if we consider the eight children of the day care center group who finally attended a hospital, as part of the hospital population. The reasons for the negative results could be the presence of other viruses not included in the panels, bacterial infections, or even non-infectious causes, since the criteria for patients’ selection were broad, therefore increasing sensitivity for study inclusion but decreasing specificity for viral detection. False-negative results for technical reasons can also be another explanation for, at least, some of the negative results.
Comparing the results obtained in 2012 at the Hospital and at the day care centers, some differences between the two populations could be observed, concerning the frequency of the different viruses. Examples are the adenovirus and the RSV, more frequent in children attending the Hospital, or the enterovirus, detected only in children staying at home or kept going to the day care center. However, only the adenovirus, linked to hospital attending, displayed a statistical difference between the two populations. Interestingly, two out of the six inpatients children had adenovirus infections, contributing to this idea that adenovirus could be linked to severity. However, it should be mentioned that this statistical difference changes from p = 0.007 to p = 0.045 (Fisher’s exact test) if we consider the moving of eight children who attended the Emergency Department of a Hospital in the Lisbon area to the hospital population. Therefore, excluding this tendency of the adenovirus, the low number of samples does not allow us to draw conclusions regarding the differences of the etiologic agents between the two populations. In conclusion, the results obtained in this study suggest that a surveillance system based on parents’ report could complement the implanted system of the National Influenza Surveillance Program, improving significantly the number of viral detections in young children. However, this should be confirmed by a subsequent study, covering a larger population, before solid recommendations can be done. All the respiratory viruses searched in this study were found to circulate in the community, at least in one of the periods, causing acute respiratory infections in young children that were usually mild but responsible for keeping most of the children and parents at home and, in some cases, for a hospital consultation or even hospitalization.
Abbreviations
- DNA:
-
Deoxyribonucleic acid
- ENVIRH:
-
project “Environment and Health in children day care centers”
- hMPV:
-
Human metapneumovirus
- PCR:
-
Polymerase chain reaction
- PIV:
-
Parainfluenza virus
- RNA:
-
Ribonucleic acid
- RSV:
-
Respiratory syncytial virus
References
Ambrose CS, Wu X, Knuf M, Wutzler P (2012) The efficacy of intranasal live attenuated influenza vaccine in children 2 through 17 years of age: a meta-analysis of 8 randomized controlled studies. Vaccine 30(5):886–892
Chow MY, Morrow AM, Booy R, Leask J (2013) Impact of children's influenza-like illnesses on parental quality of life: a qualitative study. J Paediatr Child Health 49(8):664–670
Dare R, Sanghavi SK, Bullotta A, Kneightley MC, St.George K, Wadowsky RM, Paterson DJ, McCurry KR, Reinhart TA, Husain S a, Rinaldo CR (2007) Diagnosis of human metapneumovirus infection in immunosuppressed lung transplant recipients and children evaluated for pertussis. J Clin Microbiol 45(2):548–552
Ellis JS, Curran MD (2011) Simultaneous molecular detection and confirmation of influenza A H5, with internal control. Methods Mol Biol 665:161–181
European Centre for Disease Prevention and Control (ECDC) [Internet]: Weekly influenza surveillance overview (WISO). Availabe from: http://ecdc.europa.eu/en/publications/surveillance_reports/influenza/Pages/weekly_influenza_surveillance_overview.aspx
Heim A, Ebnet C, Harste G, Pring-Akerblom P (2003) Rapid and quantitative detection of human adenovirus DNA by real-time PCR. J Med Virol 70:228–239
Henrickson KJ, Hoover S, Kehl KS, Hua W (2004) National disease burden of respiratory viruses detected in children by polymerase chain reaction. Pediatr Infect Dis J 23(1 Suppl):S11–S18
Huijskens EG, Biesmans RC, Buiting AG, Obihara CC, Rossen JW (2012) Diagnostic value of respiratory virus detection in symptomatic children using real-time PCR. Virol J 9:276
Hutchinson EC, Curran MD, Read EK, Gog JR, Digard P (2008) Mutational analysis of cis-acting RNA signals in segment 7 of influenza A virus. J Virol 82(23):11869–11879
Instituto Nacional de Saúde Dr. Ricardo Jorge (INSA) (2013) A gripe em Portugal na época 2011/2012. Relatório do Programa Nacional de Vigilância da Gripe. [The influenza season in Portugal in 2011/2012. Report of the national influenza surveillance programme]. Lisbon: INSA. Portuguese. Available from: http://hdl.handle.net/10400.18/1183
Jartti T, Söderlund-Venermo M, Hedman K, Ruuskanen O, Makela M (2013) New molecular virus detection methods and their clinical value in lower respiratory tract infections in children. Paediatr Respir Rev 14(1):38–45
Kesson AM (2007) Respiratory viral infections. Paediatr Respir Rev 8:240–248
Lambert SB, Allen KM, Druce JD, Birch CJ, Mackay IM, Carlin JB, Carapetis JR, Sloots TP, Nissen MD, Nolan TM (2007) Community epidemiology of human metapneumovirus, human coronavirus NL63, and other respiratory viruses in healthy preschool-aged children using parent-collected specimens. Pediatrics 120(4):e929–e937
Lambert SB, Whiley DM, O'Neill NT, Andrews EC, Canavan FM, Bletchly C, Siebert DJ, Sloots TP, Nissen MD (2008) Comparing nose-throat swabs and nasopharyngeal aspirates collected from children with symptoms for respiratory virus identification using real-time polymerase chain reaction. Pediatrics 122(3):e615–e620
Martin ET, Fairchok MP, Stednick ZJ, Kuypers J, Englund JA (2013) Epidemiology of multiple respiratory viruses in childcare attendees. J Infect Dis 207(6):982–989
Portuguese Laboratory Network for the Diagnosis of Influenza Infection. Contribution of the Portuguese Laboratory Network for the Diagnosis of Influenza A(H1N1)pdm09 Infection during the 2009/10 and 2010/11 influenza seasons (2012) Euro Surveill. 17(27):pii=20211. Available online: http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=20211
Tanner HE, Curran MD, Boxall EH, Osman H (2012) Viral respiratory infections during the 2009 influenza A(H1N1) outbreak in the West Midlands Region, UK. Epidemiol Infect 140(9):1551–1556
Tregoning JS, Schwarze J (2010) Respiratory viral infections in infants: causes, clinical symptoms, virology, and immunology. Clin Microbiol Rev 23(1):74–98
Acknowledgments
This study was supported by a grant from Fundação para a Ciência e Tecnologia (PTDC/SAU-ESA/100275/2008, project “Environment and Health in children day care centers”—ENVIRH).
The authors would like to thank all the children and their parents for the participation in the study and the nurses of the Emergency Department of the Hospital da Luz for the collection of biological samples at the hospital.
Conflict of interest
The authors declare that there is no conflict of interest and they have no financial relationship with the organization that sponsored the research.
Author information
Authors and Affiliations
Corresponding author
Additional information
Communicated by David Nadal
What is new in your paper on the basis what is already known in the field?
Influenza surveillance in Europe is based mainly on nationally organized sentinel networks of physicians and on hospital reports of clinically suspected or laboratory-confirmed influenza cases. This is an efficient system for adults but probably less for young children. To our knowledge, this is the first European report showing that a surveillance system based on parents’ report to a dedicated team can improve significantly the surveillance of influenza infections in young children and could complement the implanted system of the National Influenza Surveillance Program.
Rights and permissions
About this article
Cite this article
Paixão, P., Piedade, C., Papoila, A. et al. Improving influenza surveillance in Portuguese preschool children by parents’ report. Eur J Pediatr 173, 1059–1065 (2014). https://doi.org/10.1007/s00431-014-2285-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00431-014-2285-7