
Abstract
Purpose
Trials for DCIS have not explored whether outcomes for patients with large disease burden requiring mastectomy are comparable to those of patients with lumpectomy-amenable disease. We aim to identify whether patients with DCIS larger than 5 cm and diffuse-type DCIS differ in breast cancer mortality (BCM) from patients with disease less than 5 cm.
Methods
Patients diagnosed with DCIS in the SEER program were assessed to identify factors prognostic of breast-cancer-specific survival using competing risks regression.
Results
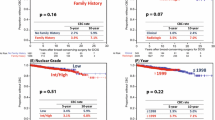
44,849 patients met criteria for the cumulative incidence estimate. On competing risks cumulative incidence approximation, the 10-year estimate for BCM for each group was 1.3%, 1.3%, 2.3%, and 5.1%, respectively, and the difference among groups was significant (p = 0.017). On competing risks regression of patients with known covariates, both diffuse-type disease and disease larger than 5 cm (hazard ratio [HR] = 6.2 and 1.7, p = 0.013 and p = 0.042, respectively) were associated with increased risk of BCM. After matching, DCIS > 5 cm and diffuse disease were associated with increased BCM relative to disease < 5 cm (HR = 1.69, p = 0.04). Among patients undergoing mastectomy for disease larger than 5 cm or diffuse disease, the 10-year cumulative incidence for BCM was 0.5% among patients undergoing bilateral mastectomy and 2.4% for patients undergoing unilateral mastectomy.
Conclusion
Patients with large and diffuse DCIS represent uncommon but poorly studied DCIS subgroups with worse prognoses than patients with disease smaller than 5 cm. Further studies are needed to elucidate the appropriate treatment for these patients.




Similar content being viewed by others


Availability of data and material
SEER data are publicly available.
Code availability
Can be provided upon request.
References
Punglia R, Bifolck K, Golshan M et al. (2018) Epidemiology, Biology, Treatment, and Prevention of Ductal Carcinoma In Situ (DCIS). Jnci Cancer Spectr. https://doi.org/10.1093/jncics/pky063.
Early Breast Cancer Trialists’ Collaborative Group (EBCTCG), Correa C, McGale P, Taylor C, Wang Y, Clarke M, et al. (2010) Overview of the randomized trials of radiotherapy in ductal carcinoma in situ of the breast. J Natl Cancer Inst Monogr. https://doi.org/10.1093/jncimonographs/lgq039.
Barrio AV, Van Zee KJ (2017) Controversies in the treatment of ductal carcinoma in situ. Annu Rev Med 68:197–211. https://doi.org/10.1146/annurev-med-050715-104920
Fisher B, Costantino J, Redmond C, Fisher E, Margolese R, Dimitrov N et al (1993) Lumpectomy compared with lumpectomy and radiation therapy for the treatment of intraductal breast cancer. N Engl J Med 328:1581–1586. https://doi.org/10.1056/NEJM199306033282201
Donker M, Litière S, Werutsky G et al (2013) Breast-conserving treatment with or without radiotherapy in ductal carcinoma In Situ: 15-year recurrence rates and outcome after a recurrence, from the EORTC 10853 randomized phase III trial. J Clin Oncol Off J Am Soc Clin Oncol 31:4054–4059. https://doi.org/10.1200/JCO.2013.49.5077
Holmberg L, Garmo H, Granstrand B, Ringberg A, Arnesson L-G, Sandelin K et al (2008) Absolute risk reductions for local recurrence after postoperative radiotherapy after sector resection for ductal carcinoma in situ of the breast. J Clin Oncol Off J Am Soc Clin Oncol 26:1247–1252. https://doi.org/10.1200/JCO.2007.12.7969
Houghton J, George WD, Cuzick J et al (2003) Radiotherapy and tamoxifen in women with completely excised ductal carcinoma in situ of the breast in the UK, Australia, and New Zealand: randomised controlled trial. Lancet Lond Engl 362:95–102. https://doi.org/10.1016/s0140-6736(03)13859-7
Fisher B, Dignam J, Wolmark N et al (1998) Lumpectomy and radiation therapy for the treatment of intraductal breast cancer: findings from National Surgical Adjuvant Breast and Bowel Project B-17. J Clin Oncol Off J Am Soc Clin Oncol 16:441–452. https://doi.org/10.1200/JCO.1998.16.2.441
Cuzick J, Sestak I, Pinder SE et al (2011) Effect of tamoxifen and radiotherapy in women with locally excised ductal carcinoma in situ: long-term results from the UK/ANZ DCIS trial. Lancet Oncol 12:21–29. https://doi.org/10.1016/S1470-2045(10)70266-7
McGuire KP, Santillan AA, Kaur P et al (2009) Are mastectomies on the rise? A 13-year trend analysis of the selection of mastectomy versus breast conservation therapy in 5865 patients. Ann Surg Oncol 16:2682–2690. https://doi.org/10.1245/s10434-009-0635-x
Silverstein MJ, Barth A, Poller DN et al (1990) Ten-year results comparing mastectomy to excision and radiation therapy for ductal carcinoma in situ of the breast. Eur J Cancer Oxf Engl 1995(31A):1425–1427. https://doi.org/10.1016/0959-8049(95)00283-o
Ward EM, DeSantis CE, Lin CC et al (2015) Cancer statistics: breast cancer in situ. CA Cancer J Clin 65:481–495. https://doi.org/10.3322/caac.21321
Gray RJ (1988) A class of $k$-sample tests for comparing the cumulative incidence of a competing risk. Ann Stat 16:1141–1154. https://doi.org/10.1214/aos/1176350951
Ho DE, Imai K, King G, Stuart EA (2007) Matching as nonparametric preprocessing for reducing model dependence in parametric causal inference. Polit Anal 15:199–236. https://doi.org/10.1093/pan/mpl013
Morrow M, Bucci C, Rademaker A (1998) Medical contraindications are not a major factor in the underutilization of breast conserving therapy. J Am Coll Surg 186:269–274. https://doi.org/10.1016/S1072-7515(97)00153-1
Schmale I, Liu S, Rayhanabad J et al (2012) Ductal carcinoma in situ (DCIS) of the breast: perspectives on biology and controversies in current management. J Surg Oncol 105:212–220. https://doi.org/10.1002/jso.22020
Solin LJ (2019) Management of ductal carcinoma in situ (dcis) of the breast: present approaches and future directions. Curr Oncol Rep 21:33. https://doi.org/10.1007/s11912-019-0777-3
Narod SA, Iqbal J, Giannakeas V et al (2015) Breast cancer mortality after a diagnosis of ductal carcinoma in situ. JAMA Oncol 1:888–896. https://doi.org/10.1001/jamaoncol.2015.2510
Glencer AC, Wong JM, Hylton NM et al (2021) Modulation of the immune microenvironment of high-risk ductal carcinoma in situ by intralesional pembrolizumab injection. Npj Breast Cancer 7:59. https://doi.org/10.1038/s41523-021-00267-z
Yi M, Krishnamurthy S, Kuerer HM et al (2008) Role of primary tumor characteristics in predicting positive sentinel lymph nodes in patients with ductal carcinoma in situ or microinvasive breast cancer. Am J Surg 196:81–87. https://doi.org/10.1016/j.amjsurg.2007.08.057
Satagopan JM, Ben-Porat L, Berwick M et al (2004) A note on competing risks in survival data analysis. Br J Cancer 91:1229–1235. https://doi.org/10.1038/sj.bjc.6602102
O’Keefe TJ, Wallace AM (2020) Surveillance, Epidemiology, and End Results program underestimates breast cancer-specific mortality after ductal carcinoma in situ diagnosis. Breast Cancer Res Treat 182:761–762. https://doi.org/10.1007/s10549-020-05733-z
Acknowledgements
We acknowledge the National Cancer Institute, specifically the SEER team, for granting us access to SEER data for this analysis.
Funding
Olivier Harismendy is supported by awards from the National Cancer Institute (U01CA196406 and P30CA023100).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interst
There are no conflicts of interest to disclose.
Ethics approval
Deferred by UCSD IRB.
Informed consent
Informed consent could not be obtained due to the use of public, de-identified data.
Consent to participate
Unable to obtain due to use of public, deidentified data.
Consent for publication
Unable to obtain due to use of public, deidentified data.
Human and animal participate
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
About this article

Cite this article
O’Keefe, T.J., Harismendy, O. & Wallace, A.M. Large and diffuse ductal carcinoma in situ: potentially lethal subtypes of “preinvasive” disease. Int J Clin Oncol 27, 121–130 (2022). https://doi.org/10.1007/s10147-021-02036-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10147-021-02036-1