
Abstract
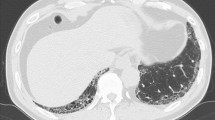
An 80-year-old woman positive for myeloperoxidase-antineutrophil cytoplasmic antibody (MPO-ANCA) was admitted with a 3-month history of fever, general malaise, and weight loss, after unsuccessful treatment with antibiotics. Upon admission, her fever persisted, and there was concomitant deterioration of renal function without active urine sediments. Furthermore, she developed hemoptysis, and chest computed tomography (CT) scan revealed bilateral diffuse alveolar hemorrhage. Although a renal biopsy was not performed because of her dementia, we initially suspected microscopic polyangiitis (MPA) on the basis of her clinical course. Because of her poor general condition, she was administered a low dose of prednisolone. Although her fever subsided, she suffered from intractable alveolar hemorrhage and eventually died from respiratory failure. During the autopsy, fibrinoid necrosis was restricted to medium-sized arteries, including the arcuate arteries of the kidneys and the bronchial arteries, without necrotizing crescentic glomerulonephritis and alveolar capillaritis. Therefore, polyarteritis nodosa (PAN) was diagnosed. It is important to distinguish between MPA and PAN because they can lead to life-threatening complications, and their treatment strategies and prognosis are different. When a patient presents with MPO-ANCA, alveolar hemorrhage, and acute renal failure with little evidence of glomerulonephritis, a differential diagnosis of PAN should be made; however, it is difficult to do so without pathological findings. Therefore, pathological examination should be carried out whenever possible.


Similar content being viewed by others


References
Jennette JC, Falk RJ, Andrassy K, Bacon PA, Churg J, Gross WL, et al. Nomenclature of systemic vasculitides. Proposal of an international consensus conference. Arthritis Rheum. 1994;37:187–92.
Kirkland GS, Savige J, Wilson D, Heale W, Sinclair RA, Hope RN. Classical polyarteritis nodosa and microscopic polyarteritis with medium vessel involvement—a comparison of the clinical and laboratory features. Clin Nephrol. 1997;47:176–80.
Samarkos M, Loizou S, Vaiopoulos G, Davies KA. The clinical spectrum of primary renal vasculitis. Semin Arthritis Rheum. 2005;35:95–111.
Kaur JS, Goldberg JP, Schrier RW. Acute renal failure following arteriography in a patient with polyarteritis nodosa. JAMA. 1982;247:833–4.
Kamali S, Gul A, Poyanli A, Cefle A, Sayarlioglu M, Inanc M, et al. A patient with classical polyarteritis nodosa evolving into end stage renal failure. Ren Fail. 2003;25:1037–41.
Williams AJ, Newland AC, Marsh FP. Acute renal failure with polyarteritis nodosa and multiple myeloma. Postgrad Med J. 1985;61:445–8.
Handa R, Wali JP, Gupta SD, Dinda AK, Aggarwal P, Wig N. Classical polyarteritis nodosa and microscopic polyangiitis—a clinicopathologic study. JAPI. 2001;49:314–9.
Falk RJ, Jennette JC. Anti-neutrophil cytoplasmic autoanti-bodies with specificity for myeloperoxidase in patients with systemic vasculitis and idiopathic necrotizing and crescentic glomerulonephritis. N Engl J Med. 1988;318:1651–7.
Jennette JC, Falk RJ. Small-vessel vasculitis. N Engl J Med. 1997;337:1512–23.
Guilpain P, Servettaz A, Goulvestre C, Barrieu S, Borderie D, Chereau C, et al. Pathogenic effects of anti-myeloperoxidase antibodies in patients with microscopic polyangitis. Arth Rheumatol. 2007;56:2455–63.
Ballow JE. Renal vasculitis. Curr Opin Nephrol Hypertens. 1993;2:231–7.
Lie JT. A rational approach to classification and pathologic diagnosis. Pathol Annu. 1989;24:25–114.
Guo X, Gopalan R, Ugbarugba S, Stringer H, Heisler M, Foreman M, et al. Hepatitis B-related polyarteritis nodosa complicated by pulmonary hemorrhage. Chest. 2001;119:1608–10.
Nick J, Tuder R, May R, Fisher J. Polyarteritis nodosa with pulmonary vasculitis. Am J Respir Crit Care Med. 1996;153:450–3.
Matsumoto T, Homma S, Okada M, Kuwabara N, Kira S, Hoshi T, et al. The lung in polyarteritis nodosa: a pathologic study of 10 cases. Hum Pathol. 1993;24:717–24.
Menon Y, Singh R, Cuchacovich R, Espinoza L. Pulmonary involvement in hepatitis B-related polyarteritis nodosa. Chest. 2002;122:1497–8.
Conflict of interest
The authors have declared that no conflict of interest exists.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Sakaguchi, Y., Uehata, T., Kawabata, H. et al. An autopsy-proven case of myeloperoxidase-antineutrophil cytoplasmic antibody-positive polyarteritis nodosa with acute renal failure and alveolar hemorrhage. Clin Exp Nephrol 15, 281–284 (2011). https://doi.org/10.1007/s10157-010-0386-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10157-010-0386-9