
Abstract
Purpose
This paper describes a large-scale administration of the Patient-Reported Outcomes Measurement Information System (PROMIS) pediatric items to evaluate measurement characteristics.
Methods
Each child completed one of seven test forms containing items from a pool of 293 PROMIS items and four legacy scales. PROMIS items covered six domains (physical function, emotional distress, social role relationship, fatigue, pain, and asthma).
Results
From January 2007 to May 2008, 4,129 children aged 8–17 were enrolled. The sample was 51% female, 55% aged 8–12, 42% minority race and 17% were Hispanic ethnicity. Approximately, 35% of the children participating in the survey consulted a clinician for a chronic illness diagnosis or treatment within 6 months prior to study enrollment.
Conclusions
The final PROMIS pediatric item banks include physical function (n = 52 items), emotional distress (n = 35 items), social role relationships (n = 15 items), fatigue (n = 34 items), pain (n = 13 items), and asthma (n = 17 items). The initial calibration data were provided by a diverse set of children with varying health states (e.g., children with a variety of common chronic illnesses) and racial/ethnic backgrounds.


Similar content being viewed by others


Abbreviations
- PROMIS:
-
Patient-Reported Outcomes Measurement Information System
- IRB:
-
Institutional Review Board
- UNC:
-
University of North Carolina
- S&W:
-
The Children’s Hospital at Scott and White in Texas
- NC:
-
North Carolina
- PedsQL™:
-
Pediatric Quality of Life Inventory™
- HRQOL:
-
Health-related quality of life
- PRO:
-
Patient-reported outcomes
- ADD/ADHD:
-
Attention-deficit disorder/attention-deficit hyperactivity disorder
- GI:
-
Gastrointestinal disease
- Cardiac:
-
Cardiac disease
- ESRD:
-
End-stage renal disease
- Psych:
-
Psychological disease
- Rheum:
-
Rheumatologic disease
- CP:
-
Cerebral palsy
References
Ader, D. N. (2007). Developing the Patient-Reported Outcomes Measurement Information System (PROMIS). Medical Care, 45(Suppl 1), S1–S2.
Cella, D., Yount, S., Rothrock, N., Gershon, R., Cook, K., Reeve, B., et al. (2007). The Patient-Reported Outcomes Measurement Information System (PROMIS): Progress of an NIH roadmap cooperative group during its first two years. Medical Care, 45(Suppl 1), S3–S11.
Chan, K. S., Mangione-Smith, R., Burwinkle, T. M., Rosen, M., & Varni, J. W. (2005). The PedsQL™: Reliability and validity of the short-form generic core scales and asthma module. Medical Care, 43, 256–265.
Guyatt, G. H., Juniper, E. F., Griffith, L. E., Feeny, D. H., & Ferrie, P. J. (1997). Children and adult perceptions of childhood asthma. Pediatrics, 99(2), 165–168.
Juniper, E. F., Guyatt, G. H., Feeny, D. H., Ferrie, P. J., Griffith, L. E., & Townsend, M. (1996). Measuring quality of life in children with asthma. Quality of Life Research, 5(1), 35–46.
DeWalt, D., Rothrock, N., Yount, S., & Stone, A. A. (2007). PROMIS cooperative group: Evaluation of item candidates: The PROMIS qualitative item review. Medical Care, 45(Suppl 1), S12–S21.
Walsh, T. R., Irwin, D. E., Meier, A., Varni, J. W., & DeWalt, D. (2008). The use of focus groups in the development of the PROMIS Pediatric Item Bank. Quality of Life Research, 17, 725–735.
Irwin, D. E., Varni, J. W., Yeatts, K., & DeWalt, D. (2009). Cognitive interviewing methodology in the development of a pediatric item bank: A patient reported outcomes measurement information system (PROMIS) Study. Health and Quality of Life Outcomes, 7(3), 1–10.
Varni, J. W., Seid, M., & Rode, C. A. (1999). The PedsQL™: Measurement model for the pediatric quality of life inventory. Medical Care, 37, 126–139.
Ravens-Sieberer, U., Gosch, A., Rajmil, L., Erhart, M., Bruil, J., Duer, W., et al. (2005). KIDSCREEN-52 quality of life measure for children and adolescents. Expert Review of Pharmacoeconomics and Outcomes Research, 2005(5), 353–364.
European DISABKIDS Group. (2006). The DISABKIDS questionnaires: Quality of life questionnaires for children with chronic conditions. Berlin: Pabst Science Publishers.
www.pedsql.org. Accessed 10 June 2009.
kidscreen.diehauptstadt.de. Accessed 10 June 2009.
Varni, J. W., Seid, M., & Kurtin, P. S. (2001). PedsQL™ 4.0. Reliability and validity of the pediatric quality of life inventory™ version 4.0 generic core scales in healthy and patient populations. Medical Care, 39, 800–812.
Varni, J. W., Limbers, C. A., & Burwinkle, T. M. (2007). Impaired health-related quality of life in children and adolescents with chronic conditions: A comparative analysis of 10 disease clusters and 33 disease categories/severities utilizing the PedsQL™ 4.0 Generic Core Scales. Health and Quality of Life Outcomes, 5, 43.
Varni, J. W., Burwinkle, T. M., Rapoff, M. A., Kamps, J. L., & Olson, N. (2004). The PedsQL in pediatric asthma: Reliability and validity of the pediatric quality of life inventory generic core scales and asthma module. Journal of Behavioral Medicine, 27, 297–318.
Acknowledgments
We would like to acknowledge the contribution of Harry A. Guess, MD, PhD, to the conceptualization and operationalization of this research prior to his death. This work was funded by the National Institutes of Health through the NIH Roadmap for Medical Research, Grant 1U01AR052181-01. Information on the Patient-Reported Outcomes Measurement Information System (PROMIS) can be found at http://nihroadmap.nih.gov/ and http://www.nihpromis.org.
Author information
Authors and Affiliations
Corresponding author
Appendix: PROMIS pediatrics domain definitions
Appendix: PROMIS pediatrics domain definitions
Emotional health
Emotional distress commonly refers to unpleasant feelings or emotions that are experienced privately and, therefore, are good candidates for assessment as patient-reported outcomes. Emotional distress among children comprises feelings of anxiety, depression, and anger.
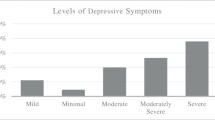
Depression
Depressive symptoms among children often include feelings of hopelessness, helplessness, and worthlessness. The PROMIS pediatrics item bank for depression focuses on negative mood (e.g., sadness), decrease in positive affect (e.g., loss of interest), negative views of the self (e.g., worthlessness, low self-esteem), and negative social cognition (e.g., loneliness, interpersonal alienation). This item bank is best characterized as depressive symptoms rather than a complete diagnostic test for depression which may include other physical manifestations.
Anxiety
Symptoms that best differentiate anxiety are those that reflect autonomic arousal and the experience of threat. Children often experience these feelings in a variety of contexts specific to their environment of home, school, and social activities. The PROMIS pediatric item bank for anxiety focuses on fear (e.g., fearfulness), anxious misery (e.g., worry), and hyperarousal (e.g., nervousness).
Anger
Anger is distinguished by attitudes of hostility and cynicism and is often associated with experiences of frustration impeding goal-directed behavior. Specific components relate to verbal and nonverbal evidence of interpersonal antagonism. The PROMIS pediatric item bank for anger focuses on angry mood (e.g., irritability, reactivity), and aggression (verbal and physical).
Social health
Social health is defined as perceived well-being regarding social activities and relationships, including the ability to relate to individuals, groups, communities, and society as a whole. The term “social health” is used here synonymously with “social function” and refers to a higher-order domain, with measurable subdomains. Components of social functioning include understanding and communication, getting along with people, participation in society, and performance of social roles.
Peer relationships
One common goal of childhood is success in socializing with others. This enables one to create positive relationships with family, friends, teachers, and colleagues. Social interaction with peers is the initial focus of PROMIS pediatric investigation in social health.
Physical function
Physical function is defined as one’s ability to carry out various activities, ranging from self-care (activities of daily living) to more challenging and vigorous activities that require increasing degrees of mobility, strength or endurance. Although several important aspect of physical function can be measured, the initial pediatric item banks will focus on (1) mobility and (2) upper extremity.
Mobility
This item banks focuses on activities of physical mobility such as getting out of bed or a chair to activities such as running.
Upper extremity
This item bank focuses on activities that require use of the upper extremity including shoulder, arm, and hand activities. Examples include writing, using buttons, or opening containers.
Pain
Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage. Pain is what the patient says it is—that is, the “gold standard” of pain assessment is self-report. Pain is divided conceptually into components of quality (referring to the nature, characteristics, intensity frequency, and duration of pain), interference with activities (impact upon physical, mental, and social activities), and avoidance behaviors (behaviors one engages into avoid, minimize, or reduce pain). The initial PROMIS pediatric item bank focuses on the interference impact of pain.
Fatigue
Fatigue is defined as an overwhelming, debilitating, and sustained sense of exhaustion that decreases one’s ability to carry out daily activities, including the ability to work effectively (for pediatric populations this primarily translates to school work) and to function at one’s usual level in family or social roles.
Asthma-specific symptoms
Asthma causes several symptoms for children that are not addressed in the generic item banks which include cough, wheeze, shortness of breath, and avoidance of triggers. Asthma is also associated with impacts such as missing school or activities with other children. The PROMIS pediatric asthma item bank focuses on symptoms specific to asthma.
Rights and permissions
About this article
Cite this article
Irwin, D.E., Stucky, B.D., Thissen, D. et al. Sampling plan and patient characteristics of the PROMIS pediatrics large-scale survey. Qual Life Res 19, 585–594 (2010). https://doi.org/10.1007/s11136-010-9618-4
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11136-010-9618-4