
Abstract
Purpose
An increase in PaCO2 is the element that defines sleep hypoventilation (SH). We queried if patients with SH, and those with PaCO2 increases during sleep for shorter time periods than SH (shamSH) differed from the patients without SH (noSH) in other ways.
Methods
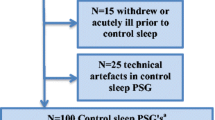
This was a retrospective re-analysis of data from 100 stable inpatients with COPD with and without chronic hypercapnic respiratory failure. COPD was defined by criteria of the Global initiative for Chronic Obstructive Lung Disease (GOLD). For this study, SH was defined by an increase in PaCO2 ≥ 1.33 kPa to a value exceeding 6.7 kPa for ≥ 10 min (≥ 20 epochs of 30 s). Patients fulfilling the increase in PaCO2 for less than 10 min (1–19 epochs) were designated shamSH. All patients had daytime arterial blood gases, lung function tests, and polysomnography (PSG) with transcutaneous CO2 (PtcCO2).
Results
Of 100 patients, 25 had PtcCO2 increase ≥ 1.33 kPa. One never exceeded 6.7 kPa, 15 had SH, and 9 shamSH. SH and shamSH patients had extra CO2 load (= PtcCO2*time) both during and between the SH periods compared to the noSH group, the SH group more than the shamSH group.
Conclusion
Using CO2 load as a measure of severity of sleep hypoventilation, SH patients have worse hypoventilation than the shamSH. Both shamSH and SH groups have extra CO2 load during and between SH periods, indicating that the SH/shamSH patients may represent a separate group of true hypoventilators during sleep.



Similar content being viewed by others
References
Berry RB, Budhiraja R, Gottlieb DJ, Gozal D, Iber C, Kapur VK, Marcus CL, Mehra R, Parthasarathy S, Quan SF, Redline S, Strohl KP, Davidson Ward SL, Tangredi MM, American Academy of Sleep M (2012) Rules for scoring respiratory events in sleep: update of the 2007 AASM Manual for the Scoring of Sleep and Associated Events. Deliberations of the Sleep Apnea Definitions Task Force of the American Academy of Sleep Medicine. J Clin Sleep Med 8(5):597–619. https://doi.org/10.5664/jcsm.2172
O'Donoghue FJ, Catcheside PG, Ellis EE, Grunstein RR, Pierce RJ, Rowland LS, Collins ER, Rochford SE, McEvoy RD, Australian trial of Noninvasive Ventilation in Chronic Airflow Limitation i (2003) Sleep hypoventilation in hypercapnic chronic obstructive pulmonary disease: prevalence and associated factors. Eur Respir J 21(6):977–984
Tarrega J, Anton A, Guell R, Mayos M, Samolski D, Marti S, Farrero E, Prats E, Sanchis J (2011) Predicting nocturnal hypoventilation in hypercapnic chronic obstructive pulmonary disease patients undergoing long-term oxygen therapy. Respiration 82(1):4–9. https://doi.org/10.1159/000321372
Holmedahl NH, Overland B, Fondenes O, Ellingsen I, Hardie JA (2014) Sleep hypoventilation and daytime hypercapnia in stable chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis 9:265–275. https://doi.org/10.2147/COPD.S57576
Mackay IF (1943) The influence of posture on the pulmonary blood volume and the alveolar gas tensions. J Physiol 102(2):228–238
Bulow K (1963) Respiration and wakefulness in man. Acta Physiol Scand Suppl 209:1–110
Mulloy E, McNicholas WT (1996) Ventilation and gas exchange during sleep and exercise in severe COPD. Chest 109(2):387–394
Birchfield RI, Sieker HO, Heyman A (1958) Alterations in blood gases during natural sleep and narcolepsy; a correlation with the electroencephalographic stages of sleep. Neurology 8(2):107–112
Birchfield RI, Sieker HO, Heyman A (1959) Alterations in respiratory function during natural sleep. J Lab Clin Med 54:216–222
Leitch AG, Clancy LJ, Leggett RJ, Tweeddale P, Dawson P, Evans JI (1976) Arterial blood gas tensions, hydrogen ion, and electroencephalogram during sleep in patients with chronic ventilatory failure. Thorax 31(6):730–735
Koo KW, Sax DS, Snider GL (1975/5) Arterial blood gases and pH during sleep in chronic obstructive pulmonary disease. Am J Med 58(5):663–670
Funding
Financial support was received from the Norwegian Extra Foundation for Health and Rehabilitation, LHL’s Research fund, Glittreklinikken LHL helse as and the Norwegian national centre of excellence in home mechanical ventilation. Minor grants received from the Norwegian lung medicine society/Takeda Nycomed, Major Eckbo’s endowments and the University of Bergen.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
PSG hardware and software were provided by ResMed Norway.
Conflict of interest
This was not an industry-supported study. Nils H. Holmedahl received lecture honorarium from Glaxo Smith Kline and a grant from the Norwegian Lung Medicine Society/Takeda Nycomed. Britt Øverland, Ove Fondenes, and Ivar Ellingsen declare that they have no conflict of interest.
Ethical approval
Written informed consent was obtained from all individual participants included in the study. The study protocol was approved by the Regional Ethics Committee in south-eastern Norway (S-09053c 299/124). Clinical trial registration number: NCT00888342.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Ellingsen, I., Fondenes, O., Øverland, B. et al. The severity of sleep hypoventilation in stable chronic obstructive pulmonary disease. Sleep Breath 25, 243–249 (2021). https://doi.org/10.1007/s11325-020-02097-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11325-020-02097-y