
Abstract
Background
Due to the increased incidence of morbid obesity, the demand for bariatric surgery is increasing. Therefore, the methods for optimising perioperative care for the improvement of surgical outcome and to increase efficacy are necessary. The aim of this prospective matched cohort study is to objectify the effect of the fast-track surgery (FTS) programme in patients undergoing primary Laparoscopic Roux-en-Y Gastric Bypass (LRYGB) surgery compared to conventional perioperative care (CPC).
Methods
This study compared the perioperative outcome data of two groups of 75 consecutive morbid obese patients who underwent a primary LRYGB according to international guidelines in the periods January 2011–April 2011 (CPC group) and April 2012–June 2012 (FTS group). The two groups were matched for age and sex. Primary endpoints were surgery and hospitalisation time, while secondary endpoints were intraoperative medication use and complication rates.
Results
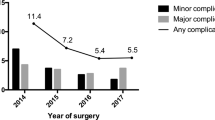
Baseline patient characteristics for age, sex, weight and ASA classification were similar (p > 0.05) for CPC and FTS patients. BMI and waist circumference were significantly lower (p < 0.05) in the FTS compared to CPC. The total time from arrival at the operating room to the arrival at the recovery was reduced from 119 to 82 min (p < 0.001). Surgery time was reduced from 80 to 56 min (p < 0.001); mean hospital stay was reduced from 65 to 43 h (p < 0.001). Major complications occurred in 3 versus 4 % in the FTS and CPC, respectively.
Conclusions
The introduction of a fast-track programme after primary LRYGB improves short-term recovery and may reduces direct hospital-related resources.

Similar content being viewed by others


References
Statistiek CBv. StatLine Home; Tabellen per thema; Leefstijl, preventief onderzoek: persoonskenmerken. In 2012.
Haslam DW, James WP. Obesity. Lancet. 2005;366(9492):1197–209.
Terranova L, Busetto L, Vestri A, et al. Bariatric surgery: Cost-effectiveness and budget impact. Obes Surg. 2012;22(4):646–53.
Bult MJ, van Dalen T, Muller AF. Surgical treatment of obesity. Eur J Endocrinol/Eur Fed Endocr Soc. 2008;158(2):135–45.
Padwal R, Klarenbach S, Wiebe N, et al. Bariatric surgery: a systematic review of the clinical and economic evidence. J Gen Intern Med. 2011;26(10):1183–94.
Sussenbach SP, Padoin AV, Silva EN, et al. Economic benefits of bariatric surgery. Obes Surg. 2012;22(2):266–70.
Buchwald H, Williams SE. Bariatric surgery worldwide 2003. Obes Surg. 2004;14(9):1157–64.
Buchwald H, Oien DM. Metabolic/bariatric surgery worldwide 2008. Obes Surg. 2009;19(12):1605–11.
Teeuwen PH, Bleichrodt RP, Strik C, et al. Enhanced recovery after surgery (ERAS) versus conventional postoperative care in colorectal surgery. J Gastrointest Surg: Off J Soc Surg Aliment Tract. 2010;14(1):88–95.
Spanjersberg WR, Reurings J, Keus F, et al. Fast track surgery versus conventional recovery strategies for colorectal surgery. Cochrane Database Syst Rev. 2011;2:CD007635.
Grantcharov TP, Kehlet H. Laparoscopic gastric surgery in an enhanced recovery programme. Br J Surg. 2010;97(10):1547–51.
Jacobsen HJ, Bergland A, Raeder J, et al. High-volume bariatric surgery in a single center: safety, quality, cost-efficacy and teaching aspects in 2,000 consecutive cases. Obes Surg. 2012;22(1):158–66.
Raeder J. Bariatric procedures as day/short stay surgery: is it possible and reasonable? Curr Opin Anaesthesiol. 2007;20(6):508–12.
Bamgbade OA, Adeogun BO, Abbas K. Fast-track laparoscopic gastric bypass surgery: outcomes and lessons from a bariatric surgery service in the United Kingdom. Obes Surg. 2012;22(3):398–402.
Lemanu DP, Srinivasa S, Singh PP, et al. Optimizing perioperative care in bariatric surgery patients. Obes Surg. 2012;22(6):979–90.
Bergland A, Gislason H, Raeder J. Fast-track surgery for bariatric laparoscopic gastric bypass with focus on anaesthesia and peri-operative care. Experience with 500 cases. Acta Anaesthesiol Scand. 2008;52(10):1394–9.
Kehlet H, Wilmore DW. Evidence-based surgical care and the evolution of fast-track surgery. Ann Surg. 2008;248(2):189–98.
Fried M, Hainer V, Basdevant A, et al. Inter-disciplinary European guidelines on surgery of severe obesity. Int J Obes. 2007;31(4):569–77.
Lonroth H. Laparoscopic gastric bypass. Obes Surg. 1998;8(6):563–5.
McCarty TM, Arnold DT, Lamont JP, et al. Optimizing outcomes in bariatric surgery: Outpatient laparoscopic gastric bypass. Ann Surg. 2005;242(4):494–8. discussion 498-501.
Elliott JA, Patel VM, Kirresh A, et al. Fast-track laparoscopic bariatric surgery: a systematic review. Updat Surg. 2013;65(2):85–94.
Freeman AL, Pendleton RC, Rondina MT. Prevention of venous thromboembolism in obesity. Expert Rev Cardiovasc Ther. 2010;8(12):1711–21.
Dobesh PP, Wittkowsky AK, Stacy Z, et al. Key articles and guidelines for the prevention of venous thromboembolism. Pharmacotherapy. 2009;29(4):410–58.
Clements RH, Yellumahanthi K, Ballem N, et al. Pharmacologic prophylaxis against venous thromboembolic complications is not mandatory for all laparoscopic Roux-en-Y gastric bypass procedures. J Am Coll Surg. 2009;208(5):917–21. discussion 921-913.
Saravanakumar K, Rao SG, Cooper GM. Obesity and obstetric anaesthesia. Anaesthesia. 2006;61(1):36–48.
Schug SA, Raymann A. Postoperative pain management of the obese patient. Best Pract Res Clin Anaesthesiol. 2011;25(1):73–81.
Practice guidelines for acute pain management in the perioperative setting: an updated report by the American Society of Anesthesiologists Task Force on Acute Pain Management. Anesthesiology 2012;116(2): 248–273.
Cottam DR, Fisher B, Atkinson J, et al. A randomized trial of bupivicaine pain pumps to eliminate the need for patient controlled analgesia pumps in primary laparoscopic Roux-en-Y gastric bypass. Obes Surg. 2007;17(5):595–600.
Kahokehr A, Sammour T, Srinivasa S, et al. Systematic review and meta-analysis of intraperitoneal local anaesthetic for pain reduction after laparoscopic gastric procedures. Br J Surg. 2011;98(1):29–36.
Sovik TT, Aasheim ET, Kristinsson J, et al. Establishing laparoscopic Roux-en-Y gastric bypass: Perioperative outcome and characteristics of the learning curve. Obes Surg. 2009;19(2):158–65.
Lemanu DP, Singh PP, Berridge K, et al. Randomized clinical trial of enhanced recovery versus standard care after laparoscopic sleeve gastrectomy. Br J Surg. 2013;100(4):482–9.
Conflict of Interest
The authors declare that they have no conflict of interest and no funding was provided.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Funding
This study was performed without grants or fees.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Dogan, K., Kraaij, L., Aarts, E.O. et al. Fast-Track Bariatric Surgery Improves Perioperative Care and Logistics Compared to Conventional Care. OBES SURG 25, 28–35 (2015). https://doi.org/10.1007/s11695-014-1355-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-014-1355-2