
Abstract
Background
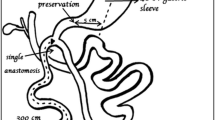
Although the duodenal switch (DS) has been the most effective weight loss surgical procedure, it is a small minority of the total bariatric surgical cases performed. Modifications that can make the operation technically simpler and reduce a long-term risk of short bowel syndrome would be of benefit. The aim of this study was to detail our initial experience with a modified DS called stomach intestinal pylorus sparing (SIPS) procedure.
Methods
Data from patients who underwent a primary SIPS procedure performed by two surgeons at two centers from January 2013 to August 2014 were retrospectively analyzed. All revisions of prior bariatric procedures were excluded. Regression analyses were performed for all follow-up weight loss data.
Results
One hundred twenty-three patients were available. One hundred two patients were beyond 1 year postoperative, with data available for 64 (62 % followed up). The mean body mass index (BMI) was 49.4 kg/m2. Two patients had diarrhea (1.6 %), four had abdominal hematoma (3.2 %), and one had a stricture (0.8 %) in the gastric sleeve. Two patients (1.6 %) were readmitted within 30 days. One patient (0.8 %) was reoperated due to an early postoperative ulcer. At 1 year, patients had an average change in BMI of 19 units (kg/m2), which was compared to an average of 38 % of total weight loss or 72 % of excess weight loss.
Conclusions
Modification of the classic DS to one with a single anastomosis and a longer common channel had effective weight loss results. Morbidity seems comparable to other stapling reconstructive procedures. Future analyses are needed to determine whether a SIPS procedure reduces the risk of future small bowel obstructions and micronutrient deficiencies.

Similar content being viewed by others


References
Hess DS, Hess DW, Oakley RS. The biliopancreatic diversion with the duodenal switch: results beyond 10 years. Obes Surg. 2005;15(3):408–16.
Buchwald H, Avidor Y, Braunwald E, et al. Bariatric surgery: a systematic review and meta-analysis. JAMA. 2004;292(14):1724–37.
Sanchez-Pernaute A, Herrera MA, Perez-Aguirre ME, et al. Single anastomosis duodeno-ileal bypass with sleeve gastrectomy (SADI-S). One to three-year follow-up. Obes Surg. 2010;20(12):1720–6.
Sánchez-Pernaute A, Rubio MÁ, Cabrerizo L, Ramos-Levi A, Pérez-Aguirre E, Torres A. Single-anastomosis duodenoileal bypass with sleeve gastrectomy (SADI-S) for obese diabetic patients. Surg Obes Relat Dis. 2015;11(5):1092–8.
Nightingale J, Woodward JM. Guidelines for management of patients with a short bowel. Gut. 2006;55 Suppl 4:v1–12.
Scopinaro N, Marinari G, Camerini G, et al. Biliopancreatic diversion for obesity: state of the art. Surg Obes Relat Dis. 2005;1(3):317–28.
Marceau P, Hould FS, Simard S, et al. Biliopancreatic diversion with duodenal switch. World J Surg. 1998;22(9):947–54.
Risstad H, Sovik TT, Engstrom M, et al. Five-year outcomes after laparoscopic gastric bypass and laparoscopic duodenal switch in patients with body mass index of 50 to 60: a randomized clinical trial. JAMA Surg. 2015;150(4):352–61.
Buchwald H, Estok R, Fahrbach K, et al. Weight and type 2 diabetes after bariatric surgery: systematic review and meta-analysis. Am J Med. 2009;122(3):248–56. e5.
Sjostrom L, Lindroos AK, Peltonen M, et al. Lifestyle, diabetes, and cardiovascular risk factors 10 years after bariatric surgery. N Engl J Med. 2004;351:2683–93. United States: 2004 Massachusetts Medical Society.
Christou NV, Sampalis JS, Liberman M, et al. Surgery decreases long-term mortality, morbidity, and health care use in morbidly obese patients. Ann Surg. 2004;240(3):416–23. discussion 23–4.
Sugerman HJ, Wolfe LG, Sica DA, et al. Diabetes and hypertension in severe obesity and effects of gastric bypass-induced weight loss. Ann Surg. 2003;237(6):751–6. discussion 7–8.
DiGiorgi M, Rosen DJ, Choi JJ, et al. Re-emergence of diabetes after gastric bypass in patients with mid- to long-term follow-up. Surg Obes Relat Dis. 2010;6(3):249–53.
Chikunguwo SM, Wolfe LG, Dodson P, et al. Analysis of factors associated with durable remission of diabetes after Roux-en-Y gastric bypass. Surg Obes Relat Dis. 2010;6(3):254–9.
Arterburn DE, Bogart A, Sherwood NE, et al. A multisite study of long-term remission and relapse of type 2 diabetes mellitus following gastric bypass. Obes Surg. 2013;23(1):93–102.
Weiner RA, Theodoridou S, Weiner S. Failure of laparoscopic sleeve gastrectomy—further procedure? Obes Facts. 2011;4 Suppl 1:42–6.
Olchowski S, Timms MR, O’Brien P, et al. More on mini-gastric bypass. Obes Surg. 2001;11(4):532.
Fisher BL, Buchwald H, Clark W, et al. Mini-gastric bypass controversy. Obes Surg. 2001;11(6):773–7.
Noun R, Skaff J, Riachi E, et al. One thousand consecutive mini-gastric bypass: short- and long-term outcome. Obes Surg. 2012;22(5):697–703.
Georgiadou D, Sergentanis TN, Nixon A, et al. Efficacy and safety of laparoscopic mini gastric bypass. A systematic review. Surg Obes Relat Dis. 2014;10(5):984–91.
Rutledge R, Walsh TR. Continued excellent results with the mini-gastric bypass: six-year study in 2,410 patients. Obes Surg. 2005;15(9):1304–8.
Csendes A, Burgos AM, Smok G, et al. Latest results (12-21 years) of a prospective randomized study comparing Billroth II and Roux-en-Y anastomosis after a partial gastrectomy plus vagotomy in patients with duodenal ulcers. Ann Surg. 2009;249(2):189–94.
Tu BL, Kelly KA. Surgical treatment of Roux stasis syndrome. J Gastrointest Surg. 1999;3(6):613–7.
Health Quality Ontario. Small bowel transplant: an evidence-based analysis. Ont Health Technol Assess Ser. 2003;3(1):1–72.
Gayer G, Barsuk D, Hertz M, et al. CT diagnosis of afferent loop syndrome. Clin Radiol. 2002;57(9):835–9.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
This article does not contain any studies with human participants or animals performed by any of the authors.
Conflict of Interest
Brian Mitzman has no conflicts of interest to declare. Daniel Cottam is a teaching consultant for Medtronic/Covidien and Vision Medical Sciences. Richie Goriparthi has no conflicts of interest to declare. Samuel Cottam has no conflicts of interest to declare. Hinali Zaveri has no conflicts of interest to declare. Amit Surve has no conflicts of interest to declare. Mitchell Roslin is a teaching consultant for Johnson & Johnson Incorporated and Medtronic/Covidien Limited where he receives compensation. He is also in the scientific advisory board at SurgiQuest and ValenTx and has stocks options in them.
Informed Consent
For this type of retrospective study, formal consent is not required.
Grants
No grants were provided for this study.
Rights and permissions
About this article

Cite this article
Mitzman, B., Cottam, D., Goriparthi, R. et al. Stomach Intestinal Pylorus Sparing (SIPS) Surgery for Morbid Obesity: Retrospective Analyses of Our Preliminary Experience. OBES SURG 26, 2098–2104 (2016). https://doi.org/10.1007/s11695-016-2077-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-016-2077-4