
Abstract
Introduction
Hyponatremia is a frequent comorbid condition of patients hospitalized for cirrhosis and a predictor of disease severity and mortality. This study evaluated the healthcare burden of hyponatremia among patients hospitalized for cirrhosis in the real world.
Methods
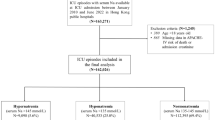
Hyponatremic (HN) patients (>-18 years of age) with cirrhosis were identified using the Premier Hospital Database (January 1, 2007 to March 31, 2010) and matched to non-HN patients with cirrhosis using a combination of exact patient characteristics and propensity score matching. Univariate and multivariate statistics were utilized to compare hospital resource utilization, cost, and 30-day hospital re-admission among patient cohorts.
Results
The study population included 21,864 subjects (HN 10,932; non-HN 10,932). The hospital length of stay (LOS) (7.63 ± 7.4 vs. 5.89 ± 6.2 days; P < 0.001), hospital cost ($13,842 ± $20,702 vs. $11,140 ± $20,562; P < 0.001), intensive care unit (ICU) LOS (4.58 ± 4.7 vs. 3.59 ± 4.4 days; P < 0.001), and ICU cost ($7,038 ± $7,781 vs. $5,360 ± $7,557; P < 0.001) were greater for the HN cohort, as was the 30-day re-admission rate (all cause: 31.1% vs. 24.8%; P < 0.001; hyponatremia related: 25.1% vs. 11.0%; P < 0.001). Multivariate analysis showed that hyponatremia was associated with a 29.5% increase in hospital LOS, a 26.6% increase in overall hospital cost, a 23.2% increase in S. ICU LOS, and a 28.6% increase in ICU cost. Additionally, hyponatremia was associated with an increased risk of 30-day hospital re-admission (all cause: odds ratio [OR] 1.37; confidence interval [CI] 1.28-1.46; P < 0.001; hyponatremia related: OR 2.68; CI 2.48-2.90; P < 0.001).
Conclusion
Hyponatremia in patients with cirrhosis is a predictor of increased hospital resource use and 30-day hospital re-admission, and represents a potential target for intervention to reduce healthcare expenditures for patients hospitalized for cirrhosis.
Similar content being viewed by others

References
Sigal SH. Hyponatremia in cirrhosis. J Hosp Med. 2012;7(Suppl. 4):S14–S17.
Angeli P, Wong F, Watson H, Ginès P; CAPPS Investigators. Hyponatremia in cirrhosis: Results of a patient population survey. Hepatology. 2006;44:1535–1542.
Fisher RA, Heuman DM, Harper AM, et al. Region 11 MELD Na exception prospective study. Ann Hepatol. 2012;11:62–67.
Kim WR, Biggins SW, Kremers WK, et al. Hyponatremia and mortality among patients on the liver-transplant waiting list. N Engl J Med. 2008;359:1018–1026.
Kim JH, Lee JS, Lee SH, et al. The association between the serum sodium level and the severity of complications in liver cirrhosis. Korean J Intern Med. 2009;24:106–112.
Kim WR, Brown RS Jr, Terrault NA, El-Serag H. Burden of liver disease in the United States: summary of a workshop. Hepatology. 2002;227–242.
Volk ML, Tocco RS, Bazick J, Rakoski MO, Lok AS. Hospital re-admissions among patients with decompensated cirrhosis. Am J Gastroenterol. 2012;107:247–252.
U.S. Department of Health and Human Services and National Institutes of Health. Action Plan for Liver Disease Research. NIH Publication No. 04-5491. 2004. Available at: http://www2.niddk.nih.gov/AboutNIDDK/ResearchAndPlanning/Liver_Disease/Action_Plan_For_Liver_Disease_Intro.htm. Accessed May 21 2012.
Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J Clin Epidemiol. 1992;45:613–619.
Nixon RM, Thompson SG. Parametric modeling of cost data in medical studies. Statist Med. 2004;23:1311–1331.
Wald R, Jaber BL, Price LL, Upadhyay A, Madias NE. Impact of hospital-associated hyponatremia on selected outcomes. Arch Intern Med. 2010;170:294–302.
Jenq CC, Tsai MH, Tian YC, et al. Serum sodium predicts prognosis in critically ill cirrhotic patients. J Clin Gastroenterol. 2010;44:220–226.
Zhang JY, Qin CY, Jia JD, Wang BE. Serum sodium concentration profile for cirrhotic patients and its effect on the prognostic value of the MELD score. Zhonghua Gan Zang Bing Za Zhi. 2012;20:108–111.
Shorr AF, Tabak YP, Johannes RS, Gupta V, Saltzberg MT, Costanzo MR. Burden of sodium abnormalities in patients hospitalized for heart failure. Cong Heart Fail. 2011;17:1–7.
Zilberberg MD, Exuzides A, Spalding J, et al. Epidemiology, clinical and economic outcomes of admission hyponatremia among hospitalized patients. Curr Med Res Opin. 2008;24:1601–1608.
Berman K, Tandra S, Forssell K, et al. Incidence and predictors of 30-day re-admission among patients hospitalized for advanced liver disease. Clin Gastroenterol Hepatol. 2011;9:254–259.
Cárdenas A, Ginès P, Marotta P, et al. Tolvaptan, an oral vasopressin antagonist, in the treatment of hyponatremia in cirrhosis. J Hepatol. 2012;56:571–578.
Okita K, Sakaida I, Okada M, et al. A multicenter, open-label, dose-ranging study to exploratively evaluate the efficacy, safety, and dose-response of tolvaptan in patients with decompensated liver cirrhosis. J Gastroenterol. 2010;45:979–987.
Fábrega E, Berja A, García-Unzueta MT, et al. Influence of aquaporin-1 gene polymorphism on water retention in liver cirrhosis. Scand J Gastroenterol. 2011;46:1267–1274.
Stone J, Hoffman, GJ. Medicare Hospital Readmissions: Issues, Policy Options and PPACA. (R40972). Washington, DC: Congressional Research Service. 2010. Available at: http://www.hospitalmedicine.org/AM/pdf/advocacy/CRS_Readmissions_Report.pdf. Accessed May 5 2012.
American Hospital Association. Hospital statistics: 2012 edition. Chicago, IL: American Hospital Association; 2012.
Author information
Authors and Affiliations
Corresponding author
Additional information
The original online version for this chapter can be found at www.advancesintherapy.com
Rights and permissions
About this article
Cite this article
Deitelzweig, S., Amin, A., Christian, R. et al. Hyponatremia-Associated Healthcare Burden Among US Patients Hospitalized for Cirrhosis. Adv Therapy 30, 71–80 (2013). https://doi.org/10.1007/s12325-012-0073-1
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12325-012-0073-1