
Abstract
Background
The recent emergence of the Coronavirus Disease (COVID-19) disease had been associated with reports of fungal infections such as aspergillosis and mucormycosis especially among critically ill patients treated with steroids. The recent surge in cases of COVID-19 in India during the second wave of the pandemic had been associated with increased reporting of invasive mucormycosis post COVID-19. There are multiple case reports and case series describing mucormycosis in COVID-19.
Purpose
In this review, we included most recent reported case reports and case-series of mucormycosis among patients with COVID-19 and describe the clinical features and outcome.
Results
Many of the mucormycosis reports were eported from India, especially in COVID-19 patients who were treated and recovered patients. The most commonly reported infection sites were rhino-orbital/rhino-cerebral mucormycosis. Those patients were diabetic and had corticosteroids therapy for controlling the severity of COVID-19, leading to a higher fatality in such cases and complicating the pandemic scenario. The triad of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), corticosteroid use and uncontrolled diabetes mellitus have been evident for significant increase in the incidence of angioinvasive maxillofacial mucormycosis. In addition, the presence of spores and other factors might play a role as well.
Conclusion
With the ongoing COVID-19 pandemic and increasing number of critically ill patients infected with SARS-CoV-2, it is important to develop a risk-based approach for patients at risk of mucormycosis based on the epidemiological burden of mucormycosis, prevalence of diabetes mellitus, COVID-19 disease severity and use of immune modulating agents including the combined use of corticosteroids and immunosuppressive agents in patients with cancer and transplants.
Similar content being viewed by others


Introduction
The current Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) infection is associated with a wide clinical spectrum of Coronavirus Disease 2019 (COVID-19) that ranges from being asymptomatic to severe disease requiring intensive care unit (ICU) admission [1,2,3,4,5,6,7]. The rate of admission to ICU is about 5% of all COVID-19 patients [8, 9]. Severe COVID-19 pneumonia is associated with immune dysregulation and cytokine syndrome leading to the increased use of immunomodulators [10, 11]. Emerging fungal infections such as aspergillosis were described in critically ill patients treated with steroids [12]. The mortality rate of SARS-CoV-2 infection in critically ill patients co-infected with aspergillosis was high [13].
Since the emergence of the COVID-19 pandemic, it has been suspected that mucormycosis might cause significant morbidity to infected patients. This was based on a retrospective analysis of SARS and influenza cases as suggested by Song et al. [14]. The more vulnerable individuals are those requiring hospitalization and intensive care, which represent advanced stage of their disease [15]. The recent surge in cases of COVID-19 in India during the second wave of the pandemic had been associated with increased reporting of invasive mucormycosis post COVID-19, of up to 9000 cases and are continuously being reported to be rising, popularly known as black fungal infection [16,17,18]. In this review, we describe the important risk factors, clinical presentation and outcome of mucormycosis in patients infected with SARS-CoV-2.
Incidence and prevalence
The occurrence of mucormycosis, a rare disease, in the general population was previously cited as 0.005 to 1.7 per million population [19]. However, the incidence of mucormycosis in India was reported to be 0.14/1000 diabetic patients which is 80 times higher than that reported in other parts of the world[20] and more than that in the general population based on computational-modeling [21]. Given the large number of diabetic patients in India of almost 62 million, mucormycosis has caused large public health burden in India [20]. In one study, diabetes mellitus was the underlying disease in 54–76% of mucormycosis cases with 8–22% presenting with diabetic ketoacidosis [22]. In addition, there had been geographic difference in the rate of diabetes mellitus among patients with mucormycosis in India. Even prior to COVID-19, the prevalence of diabetes mellitus was a major risk factor with regional differences ranging from 67% in North India to 22% among patients from the South of India [23]. The true incidence of rhino-orbital mucormycosis in COVID-19 patients is not known. However, there are multiple case reports describing mucormycosis in COVID-19 and most of these case reports are presently from India, especially in COVID-19 treated and recovered patients those were diabetic and corticosteroids were administered injudiciously for controlling severity of COVID-19, leading to a higher fatality in such cases and complicating the pandemic scenario [17, 18, 24,25,26,27,28,29,30,31,32,33,34,35,36,37].
Risk factors
There are multiple possible contributing factors for the development of mucormycosis among patients with COVID-19 and these include diabetes mellitus, obesity, use of corticosteroid, and the development of cytokine storms (Fig. 1). The triad of SARS-CoV-2, steroid and uncontrolled diabetes mellitus have contributed towards a significant increase in the incidence of angioinvasive maxillofacial mucormycosis [30]. However, the presence of spores and other factors might play a role as well [38]. The contribution of diabetes mellitus per se to the development of rhino-orbital-cerebral mucormycosis was the most common underlying comorbidity in 340 of 851 (40%) patients who were included in a meta-analysis, with an odds ratio (OR) of 2.49 (95% CI 1.77–3.54) compared to the next possible factor of having hematological malignancies with an OR of 0.76 (0.44–1.26) [19]. The role of Interleukin 6 blockers as a risk factor for mucormycosis is not clear [39]. Whether the combined use of steroids and interleukin 6 blockers will increase the risk of mucormycosis compared to the use of steroids alone needs more studies.

Possible contributing Factors for the development of Mucormycosis among COVID-19 patients
Clinical features and management
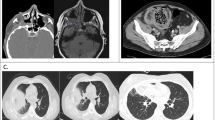
Literature review identified 30 publications of case reports and case series of mucormycosis among COVID-19 patients [24,25,26, 30, 31, 33,34,35,36,37, 40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55]. Of all the reports, 11 publications were from India [24,25,26, 30,31,32,33,34,35,36,37]. The most commonly reported infection sites were rhino-orbital/rhino-cerebral mucormycosis[24,25,26, 30, 32,33,34,35,36,37, 40, 42, 45, 47, 52,53,54]. Other presentations included pulmonary [31, 41, 43, 44, 49, 51, 55], cutaneous [46], disseminated [56] and gastrointestinal [48] diseases. The reported organisms were Rhizopus spp. [24, 31, 36, 41,42,43,44, 47, 49, 51, 55] and the others were reported as unspecified Mucorale [25, 26, 30, 33,34,35, 37, 40, 45, 48, 50, 52, 54]. The management of mucormycosis is usually difficult and requires urgent medical and surgical debridement while the choice of drug to treat mucormycosis is Amphotericin B [23, 57] and Amphotericin was used in 23 of the included studies [24,25,26, 30,31,32,33,34,35,36,37, 40,41,42,43,44, 46, 47, 49,50,51,52,53,54] and surgical debridement was reported in 20 of the included studies [24,25,26, 30, 32,33,34,35,36,37, 40, 44,45,46,47, 50,51,52,53,54]. The majority of the included patients in this review underwent surgical resection/debridement [24,25,26, 30, 32,33,34,35,36,37, 40, 44,45,46,47, 50,51,52,53,54].
Outcomes and prognosis
Before the COVID-19 era, mucormycosis is known for its poor prognosis, especially with delayed management may lead to a high mortality rate. There was no difference in the mortality between solid organ transplants and diabetes mellitus with a mortality of about 28%, (2/7 (28.57%) vs 5/18 (27.78%); p = 0.66 in patients with solid organ transplant and diabetes mellitus, respectively) [58]. However, another study showed higher mortality of 49% among diabetes mellitus patients compared to 30% among non-diabetic patients[58]. Morbidity and mortality were linked to the invasive nature of the underlying disease[59]. However, even with COVID-19, early intravenous anti-fungal treatment and surgical debridement were associated with favorable outcomes[26].
Discussion
The etiologic agent of mucormycosis are ubiquitous in nature and thus may easily be acquired, and its global epidemiology has been studied by several investigators, and may pose a threat during ongoing pandemic as has been observed in India [17, 23, 27, 57, 60, 61]. Due to the steep rise in cases of mucormycosis (black fungus infection) amid the second COVID-19 pandemic wave and its association with severe complications and associated higher fatality rate in post COVID-19 patients, this rare disease is now a notifiable disease in India. It is postulated that the use of non-sterile medical supplies might be associated with spore contamination and higher exposure of patients to mucormycosis [62, 63]. As summarized in Tables 1 and 2, most patients had severe COVID-19 pneumonia requiring intensive care, intubation and ventilation. In addition, most patients had underlying diabetes mellitus and received steroids [28, 64, 65]. The presence of diabetes mellitus is a major predisposing factor for mucormycosis as described in a meta-analysis among 600 (70%) of 851 patients with rhino-orbital–cerebral mucormycosis [19]. The presence of diabetes mellitus among patients with COVID-19 was estimated to be 17% in one study [66] and 9% in another study [67]. However, the presence of diabetes mellitus might be higher in other populations and may be more than 50% [4,5,6]. One meta-analysis showed that diabetes mellitus was associated with an odds ratio (OR) of 2.40 (95% CI 1.98–2.91) for severe disease [68], OR of 1.64 (95% CI 2.30–1.08) in a second meta-analysis [69], and an OR of 2.04, 95% CI 1.67–2.50 in a third meta-analysis [66]. Corticosteroid are currently the only medication that had shown conclusively to be effective in the treatment of COVID-19 in clinical trials therapy [70,71,72]. The RECOVERY trial utilized dexamethasone at a dose of 6 mg intravenous or oral once a day for treatment of COVID-19 [73]. Systemic steroids could further exaggerate the underlying glycemic control as well as impede the body’s immune system. The use of high dose corticosteroid had been used in patients with COVID-19 disease [74]and the use of such medications required assessment [75]. One study showed that adherence to the use of low dose corticosteroid and good glycemic control were important in having no mucormycosis among 1027 ICU patients despite the use of corticosteroids in 89% and that 40% had diabetes mellitus [76]. The presence of these pre-disposing factors in association with high fungal spore burden in certain localities and communities may set the perfect storm for the development of mucormycosis in patients with COVID-19 patients.
The outcome was favorable for patients who had surgical debridement in three case series [25, 26, 35]. With the ongoing COVID-19 pandemic and increasing number of critically ill patients infected with SARS-CoV-2, it is important to develop a risk-based approach for patients at risk of mucormycosis based on the epidemiological burden of mucormycosis, prevalence of diabetes mellitus, COVID-19 disease severity and use of immune modulating agents including the combined use of steroids and immunosuppressive agents in patients with cancer and transplants. A suggested approach for aspergillosis in COVID-19 was developed [77] and a similar approach is needed for mucormycosis in SARS-CoV-2 infected patients. Whether a mold prophylaxis is required in high-risk patients need further studies.
Early diagnosis of cases of mucormycosis, timely treatment with prescribed drugs and surgical operations, checking glycemic levels and judicious use of corticosteroids in patients with COVID-19 along with adopting appropriate hygienic and sanitization measures would aid in limiting the rising cases of this fungal infection. In-depth studies are required to investigate how COVID-19 is triggering mucormycosis infections in patients and why mainly most cases are being reported from India as compared to other countries amidst second wave of ongoing pandemic.
References
Chen N, Zhou M, Dong X, Qu J, Gong F, Han Y, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. 2020;395:507–13. https://doi.org/10.1016/S0140-6736(20)30211-7.
Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020;6736:1–9. https://doi.org/10.1016/S0140-6736(20)30566-3.
Nicastri E, D’Abramo A, Faggioni G, De Santis R, Mariano A, Lepore L, et al. Coronavirus disease (COVID-19) in a paucisymptomatic patient: Epidemiological and clinical challenge in settings with limited community transmission, Italy, February 2020. Eurosurveillance. 2020. https://doi.org/10.2807/1560-7917.ES.2020.25.11.2000230.
Al-Omari A, Alhuqbani WN, Zaidi ARZ, Al-Subaie MF, AlHindi AM, Abogosh AK, et al. Clinical characteristics of non-intensive care unit COVID-19 patients in Saudi Arabia: a descriptive cross-sectional study. J Infect Public Health. 2020;13:1639–44. https://doi.org/10.1016/j.jiph.2020.09.003.
Al Mutair A, Alhumaid S, Alhuqbani WN, Zaidi ARZ, Alkoraisi S, Al-Subaie MF, et al. Clinical, epidemiological, and laboratory characteristics of mild-to-moderate COVID-19 patients in Saudi Arabia: an observational cohort study. Eur J Med Res. 2020;25:61. https://doi.org/10.1186/s40001-020-00462-x.
AlJishi JM, Alhajjaj AH, Alkhabbaz FL, AlAbduljabar TH, Alsaif A, Alsaif H, et al. Clinical characteristics of asymptomatic and symptomatic COVID-19 patients in the Eastern Province of Saudi Arabia. J Infect Public Health. 2021;14:6–11. https://doi.org/10.1016/j.jiph.2020.11.002.
Dhama K, Khan S, Tiwari R, Sircar S, Bhat S, Malik YS, et al. Coronavirus disease 2019–COVID-19. Clin Microbiol Rev. 2020;33:1–48. https://doi.org/10.1128/CMR.00028-20.
Tirupathi R, Muradova V, Shekhar R, Salim SA, Al-Tawfiq JA, Palabindala V. COVID-19 disparity among racial and ethnic minorities in the US: a cross sectional analysis. Travel Med Infect Dis. 2020;38:101904. https://doi.org/10.1016/j.tmaid.2020.101904.
Al-Tawfiq JA, Leonardi R, Fasoli G, Rigamonti D. Prevalence and fatality rates of COVID-19: what are the reasons for the wide variations worldwide? Travel Med Infect Dis. 2020;35:101711. https://doi.org/10.1016/j.tmaid.2020.101711.
Giamarellos-Bourboulis EJ, Netea MG, Rovina N, Akinosoglou K, Antoniadou A, Antonakos N, et al. Complex immune dysregulation in COVID-19 patients with severe respiratory failure. Cell Host Microbe. 2020;27:992-1000.e3. https://doi.org/10.1016/j.chom.2020.04.009.
Guaraldi G, Meschiari M, Cozzi-Lepri A, Milic J, Tonelli R, Menozzi M, et al. Tocilizumab in patients with severe COVID-19: a retrospective cohort study. Lancet Rheumatol. 2020;2:e474–84. https://doi.org/10.1016/S2665-9913(20)30173-9.
Arastehfar A, Carvalho A, van de Veerdonk FL, Jenks JD, Koehler P, Krause R, et al. COVID-19 associated pulmonary aspergillosis (CAPA)—from immunology to treatment. J Fungi. 2020;6:1–17. https://doi.org/10.3390/jof6020091.
Lahmer T, Kriescher S, Herner A, Rothe K, Spinner CD, Schneider J, et al. Invasive pulmonary aspergillosis in critically ill patients with severe COVID-19 pneumonia: results from the prospective AspCOVID-19 study. PLoS ONE. 2021. https://doi.org/10.1371/journal.pone.0238825.
Song G, Liang G, Liu W. Fungal co-infections associated with global COVID-19 pandemic: a clinical and diagnostic perspective from China. Mycopathologia. 2020;185:599–606. https://doi.org/10.1007/s11046-020-00462-9.
Gangneux JP, Bougnoux ME, Dannaoui E, Cornet M, Zahar JR. Invasive fungal diseases during COVID-19: we should be prepared. J Mycol Med. 2020. https://doi.org/10.1016/j.mycmed.2020.100971.
BBC. Black fungus: India reports nearly 9,000 cases of rare infection—BBC News 2021. 2021. https://www.bbc.com/news/world-asia-india-57217246. Accessed 28 May 2021.
Singh AK, Singh R, Joshi SR, Misra A. Mucormycosis in COVID-19: a systematic review of cases reported worldwide and in India. Diabetes Metab Syndr Clin Res Rev. 2021. https://doi.org/10.1016/j.dsx.2021.05.019.
Biswas S. Mucormycosis: The “black fungus” maiming Covid patients in India—BBC News 2021. 2021. https://www.bbc.com/news/world-asia-india-57027829. Accessed 29 May 2021.
Jeong W, Keighley C, Wolfe R, Lee WL, Slavin MA, Kong DCM, et al. The epidemiology and clinical manifestations of mucormycosis: a systematic review and meta-analysis of case reports. Clin Microbiol Infect. 2019;25:26–34. https://doi.org/10.1016/j.cmi.2018.07.011.
Chander J, Kaur M, Singla N, Punia RPS, Singhal SK, Attri AK, et al. Mucormycosis: battle with the deadly enemy over a five-year period in India. J Fungi. 2018. https://doi.org/10.3390/jof4020046.
A. Chakrabarti, P. Sood DWD. Estimating fungal infection burden in India using computational models: mucormycosis burden as a case study. ESCMID. 2021.
Prakash H, Chakrabarti A. Epidemiology of mucormycosis in India. Microorganisms. 2021;9:1–12. https://doi.org/10.3390/microorganisms9030523.
Prakash H, Ghosh AK, Rudramurthy SM, Singh P, Xess I, Savio J, et al. A prospective multicenter study on mucormycosis in India: epidemiology, diagnosis, and treatment. Med Mycol. 2019;57:395–402. https://doi.org/10.1093/mmy/myy060.
Sarkar S, Gokhale T, Choudhury S, Deb A. COVID-19 and orbital mucormycosis. Indian J Ophthalmol. 2021;69:1002–4. https://doi.org/10.4103/ijo.IJO_3763_20.
Sen M, Lahane S, Lahane TP, Parekh R, Honavar SG. Mucor in a viral land: a tale of two pathogens. Indian J Ophthalmol. 2021;69:244–52. https://doi.org/10.4103/ijo.IJO_3774_20.
Sharma S, Grover M, Bhargava S, Samdani S, Kataria T. Post coronavirus disease mucormycosis: a deadly addition to the pandemic spectrum. J Laryngol Otol. 2021. https://doi.org/10.1017/S0022215121000992.
Chegini Z, Didehdar M, Khoshbayan A, Rajaeih S, Salehi M, Shariati A. Epidemiology, clinical features, diagnosis and treatment of cerebral mucormycosis in diabetic patients: a systematic review of case reports and case series. Mycoses. 2020;63:1264–82. https://doi.org/10.1111/myc.13187.
Bhatt K, Agolli A, Patel MH, Garimella R, Devi M, Garcia E, et al. High mortality co-infections of COVID-19 patients: mucormycosis and other fungal infections. Discoveries. 2021;9:e126. https://doi.org/10.15190/d.2021.5.
Dyer O. COVID-19: India sees record deaths as “black fungus” spreads fear. BMJ. 2021;373:n1238. https://doi.org/10.1136/bmj.n1238.
Moorthy A, Gaikwad R, Krishna S, Hegde R, Tripathi KK, Kale PG, et al. SARS-CoV-2, uncontrolled diabetes and corticosteroids—an unholy trinity in invasive fungal infections of the maxillofacial region? A retrospective, multi-centric analysis. J Maxillofac Oral Surg. 2021. https://doi.org/10.1007/s12663-021-01532-1.
Garg D, Muthu V, Sehgal IS, Ramachandran R, Kaur H, Bhalla A, et al. Coronavirus disease (Covid-19) associated mucormycosis (CAM): case report and systematic review of literature. Mycopathologia. 2021;186:289–98. https://doi.org/10.1007/s11046-021-00528-2.
Maini A, Tomar G, Khanna D, Kini Y, Mehta H, Bhagyasree V. Sino-orbital mucormycosis in a COVID-19 patient: a case report. Int J Surg Case Rep. 2021. https://doi.org/10.1016/j.ijscr.2021.105957.
Mehta S, Pandey A. Rhino-orbital mucormycosis associated with COVID-19. Cureus. 2020. https://doi.org/10.7759/cureus.10726.
Rao R, Shetty AP, Nagesh CP. Orbital infarction syndrome secondary to rhino-orbital mucormycosis in a case of COVID-19: clinico-radiological features. Indian J Ophthalmol. 2021;69:1627–30. https://doi.org/10.4103/ijo.IJO_1053_21.
Ravani SA, Agrawal GA, Leuva PA, Modi PH, Amin KD. Rise of the phoenix: Mucormycosis in COVID-19 times. Indian J Ophthalmol. 2021;69:1563–8. https://doi.org/10.4103/ijo.IJO_310_21.
Revannavar SM, Supriya P, Samaga L, Vineeth K. COVID-19 triggering mucormycosis in a susceptible patient: a new phenomenon in the developing world? BMJ Case Rep. 2021. https://doi.org/10.1136/bcr-2021-241663.
Saldanha M, Reddy R, Vincent MJ. Title of the article: paranasal mucormycosis in COVID-19 patient. Indian J Otolaryngol Head Neck Surg. 2021. https://doi.org/10.1007/s12070-021-02574-0.
Skiada A, Pavleas I, Drogari-Apiranthitou M. Epidemiology and diagnosis of mucormycosis: an update. J Fungi. 2020;6:1–20. https://doi.org/10.3390/jof6040265.
Candel FJ, Peñuelas M, Tabares C, Garcia-Vidal C, Matesanz M, Salavert M, et al. Fungal infections following treatment with monoclonal antibodies and other immunomodulatory therapies. Rev Iberoam Micol. 2020;37:5–16. https://doi.org/10.1016/j.riam.2019.09.001.
Alekseyev K, Didenko L, Chaudhry B. Rhinocerebral mucormycosis and COVID-19 pneumonia. J Med Cases. 2021;12:85–9. https://doi.org/10.14740/jmc3637.
Bellanger A-P, Navellou J-C, Lepiller Q, Brion A, Brunel A-S, Millon L, et al. Mixed mold infection with Aspergillus fumigatus and Rhizopus microsporus in a severe acute respiratory syndrome Coronavirus 2 (SARS-CoV-2) patient. Infect Dis Now. 2021. https://doi.org/10.1016/j.idnow.2021.01.010.
Dallalzadeh LO, Ozzello DJ, Liu CY, Kikkawa DO, Korn BS. Secondary infection with rhino-orbital cerebral mucormycosis associated with COVID-19. Orbit (London). 2021. https://doi.org/10.1080/01676830.2021.1903044.
Johnson AK, Ghazarian Z, Cendrowski KD, Persichino JG. Pulmonary aspergillosis and mucormycosis in a patient with COVID-19. Med Mycol Case Rep. 2021;32:64–7. https://doi.org/10.1016/j.mmcr.2021.03.006.
Kanwar A, Jordan A, Olewiler S, Wehberg K, Cortes M, Jackson BR. A fatal case of rhizopus azygosporus pneumonia following covid-19. J Fungi. 2021;7:1–6. https://doi.org/10.3390/jof7030174.
Karimi-Galougahi M, Arastou S, Haseli S. Fulminant mucormycosis complicating coronavirus disease 2019 (COVID-19). Int Forum Allergy Rhinol. 2021. https://doi.org/10.1002/alr.22785.
Khatri A, Chang KM, Berlinrut I, Wallach F. Mucormycosis after Coronavirus disease 2019 infection in a heart transplant recipient—case report and review of literature. J Med Mycol. 2021. https://doi.org/10.1016/j.mycmed.2021.101125.
Mekonnen ZK, Ashraf DC, Jankowski T, Grob SR, Vagefi MR, Kersten RC, et al. Acute invasive rhino-orbital mucormycosis in a patient with COVID-19-associated acute respiratory distress syndrome. Ophthal Plast Reconstr Surg. 2021;37:E40–2. https://doi.org/10.1097/IOP.0000000000001889.
Do Monte ES, Dos Santos MEL, Ribeiro IB, De Oliveira LG, Baba ER, Hirsch BS, et al. Rare and fatal gastrointestinal mucormycosis (Zygomycosis) in a COVID-19 patient: a case report. Clin Endosc. 2020;53:746–9. https://doi.org/10.5946/CE.2020.180.
Pasero D, Sanna S, Liperi C, Piredda D, Pietro BG, Casadio L, et al. A challenging complication following SARS-CoV-2 infection: a case of pulmonary mucormycosis. Infection. 2020. https://doi.org/10.1007/s15010-020-01561-x.
Pauli MA, Pereira LM, Monteiro ML, de Camargo AR, Rabelo GD. Painful palatal lesion in a patient with COVID-19. Oral Surg Oral Med Oral Pathol Oral Radiol. 2021. https://doi.org/10.1016/j.oooo.2021.03.010.
Placik DA, Taylor WL, Wnuk NM. Bronchopleural fistula development in the setting of novel therapies for acute respiratory distress syndrome in SARS-CoV-2 pneumonia. Radiol Case Rep. 2020;15:2378–81. https://doi.org/10.1016/j.radcr.2020.09.026.
Veisi A, Bagheri A, Eshaghi M, Rikhtehgar MH, Rezaei Kanavi M, Farjad R. Rhino-orbital mucormycosis during steroid therapy in COVID-19 patients: A case report. Eur J Ophthalmol. 2021. https://doi.org/10.1177/11206721211009450.
Waizel-Haiat S, Guerrero-Paz JA, Sanchez-Hurtado L, Calleja-Alarcon S, Romero-Gutierrez L. A case of fatal rhino-orbital mucormycosis associated with new onset diabetic ketoacidosis and COVID-19. Cureus. 2021. https://doi.org/10.7759/cureus.13163.
Werthman-Ehrenreich A. Mucormycosis with orbital compartment syndrome in a patient with COVID-19. Am J Emerg Med. 2021;42:264.e5-264.e8. https://doi.org/10.1016/j.ajem.2020.09.032.
Zurl C, Hoenigl M, Schulz E, Hatzl S, Gorkiewicz G, Krause R, et al. Autopsy proven pulmonary mucormycosis due to Rhizopus microsporus in a critically Ill COVID-19 patient with underlying hematological malignancy. J Fungi. 2021;7:1–4. https://doi.org/10.3390/jof7020088.
Hanley B, Naresh KN, Roufosse C, Nicholson AG, Weir J, Cooke GS, et al. Histopathological findings and viral tropism in UK patients with severe fatal COVID-19: a post-mortem study. Lancet Microbe. 2020;1:e245–53. https://doi.org/10.1016/S2666-5247(20)30115-4.
Cornely OA, Alastruey-Izquierdo A, Arenz D, Chen SCA, Dannaoui E, Hochhegger B, et al. Global guideline for the diagnosis and management of mucormycosis: an initiative of the European Confederation of Medical Mycology in cooperation with the Mycoses Study Group Education and Research Consortium. Lancet Infect Dis. 2019;19:e405–21. https://doi.org/10.1016/S1473-3099(19)30312-3.
Al-Obaidi M, Youssefi B, Bardwell J, Bouzigard R, Le CH, Zangeneh TT. A comparative analysis of mucormycosis in immunosuppressed hosts including patients with uncontrolled diabetes in the Southwest United States. Am J Med. 2021. https://doi.org/10.1016/j.amjmed.2021.04.008.
Bellazreg F, Hattab Z, Meksi S, Mansouri S, Hachfi W, Kaabia N, et al. Outcome of mucormycosis after treatment: report of five cases. New Microbes New Infect. 2015;6:49–52. https://doi.org/10.1016/j.nmni.2014.12.002.
Camara-Lemarroy CR, González-Moreno EI, Rodríguez-Gutiérrez R, Rendón-Ramírez EJ, Ayala-Cortés AS, Fraga-Hernández ML, et al. Clinical features and outcome of mucormycosis. Interdiscip Perspect Infect Dis. 2014. https://doi.org/10.1155/2014/562610.
Szarpak L. Mucormycosis - a serious threat in the COVID-19 pandemic? J Infect. 2021. https://doi.org/10.1016/j.jinf.2021.05.015.
Hartnett KP, Jackson BR, Perkins KM, Glowicz J, Kerins JL, Black SR, et al. A guide to investigating suspected outbreaks of mucormycosis in healthcare. J Fungi. 2019;5:69. https://doi.org/10.3390/jof5030069.
Alsuwaida K. Primary cutaneous mucormycosis complicating the use of adhesive tape to secure the endotracheal tube. Can J Anesth. 2002;49:880–2. https://doi.org/10.1007/BF03017426.
John TM, Jacob CN, Kontoyiannis DP. When uncontrolled diabetes mellitus and severe covid-19 converge: the perfect storm for mucormycosis. J Fungi. 2021. https://doi.org/10.3390/jof7040298.
Verma DK, Bali RK. COVID-19 and mucormycosis of the craniofacial skeleton: causal, contributory or coincidental? J Maxillofac Oral Surg. 2021;20:165–6. https://doi.org/10.1007/s12663-021-01547-8.
Giri M, Puri A, Wang T, Guo S. Comparison of clinical manifestations, pre-existing comorbidities, complications and treatment modalities in severe and non-severe COVID-19 patients: a systemic review and meta-analysis. Sci Prog. 2021. https://doi.org/10.1177/00368504211000906.
Yin T, Li Y, Ying Y, Luo Z. Prevalence of comorbidity in Chinese patients with COVID-19: systematic review and meta-analysis of risk factors. BMC Infect Dis. 2021. https://doi.org/10.1186/s12879-021-05915-0.
Li X, Zhong X, Wang Y, Zeng X, Luo T, Liu Q. Clinical determinants of the severity of COVID-19: A systematic review and meta-analysis. PLoS ONE. 2021. https://doi.org/10.1371/journal.pone.0250602.
Cheng S, Zhao Y, Wang F, Chen Y, Kaminga AC, Xu H. Comorbidities’ potential impacts on severe and non-severe patients with COVID-19: A systematic review and meta-analysis. Medicine (Baltimore). 2021;100:e24971. https://doi.org/10.1097/MD.0000000000024971.
Zhang W, Zhao Y, Zhang F, Wang Q, Li T, Liu Z, et al. The use of anti-inflammatory drugs in the treatment of people with severe coronavirus disease 2019 (COVID-19): the experience of clinical immunologists from China. Clin Immunol. 2020. https://doi.org/10.1016/j.clim.2020.108393.
McCreary EK, Coronavirus PJM, Disease, . Treatment: a review of early and emerging options. Open Forum Infect Dis. 2019;2020:7. https://doi.org/10.1093/ofid/ofaa105.
Russell CD, Millar JE, Baillie JK. Clinical evidence does not support corticosteroid treatment for 2019-nCoV lung injury. Lancet. 2020;395:473–5. https://doi.org/10.1016/S0140-6736(20)30317-2.
RECOVERY Collaborative Group. Dexamethasone in hospitalized patients with COVID-19—preliminary report. N Engl J Med. 2020. https://doi.org/10.1056/nejmoa2021436.
AlBahrani S, Al-Tawfiq JA, Jebakumar AZ, Alghamdi M, Zakary N, Seria M, et al. Clinical features and outcome of low and high corticosteroids in admitted COVID-19 patients. J Epidemiol Glob Health. 2021. https://doi.org/10.2991/jegh.k.210521.001.
Rodriguez-Morales AJ, Sah R, Millan-Oñate J, Gonzalez A, Montenegro-Idrogo JJ, Scherger S, et al. COVID-19 associated mucormycosis: the urgent need to reconsider the indiscriminate use of immunosuppressive drugs. Ther Adv Infect Dis. 2021. https://doi.org/10.1177/20499361211027065.
Mulakavalupil B, Vaity C, Joshi S, Misra A, Pandit RA. Absence of Case of Mucormycosis (March 2020–May 2021) under strict protocol driven management care in a COVID-19 specific tertiary care intensive care unit. Diabetes Metab Syndr Clin Res Rev. 2021;15:102169. https://doi.org/10.1016/j.dsx.2021.06.006.
Koehler P, Bassetti M, Chakrabarti A, Chen SCA, Colombo AL, Hoenigl M, et al. Defining and managing COVID-19-associated pulmonary aspergillosis: the 2020 ECMM/ISHAM consensus criteria for research and clinical guidance. Lancet Infect Dis. 2021. https://doi.org/10.1016/S1473-3099(20)30847-1.
Pakdel F, Ahmadikia K, Salehi M, Tabari A, Jafari R, Mehrparvar G, et al. Mucormycosis in patients with COVID-19: a cross-sectional descriptive multicenter study from Iran. Mycoses. 2021. https://doi.org/10.1111/myc.13334.
Singh RP, Gupta N, Kaur T, Gupta A. Rare case of gastrointestinal mucormycosis with colonic perforation in an immunocompetent patient with COVID-19. BMJ Case Rep. 2021;14:e244096. https://doi.org/10.1136/bcr-2021-244096.
Arjun R, Felix V, Niyas VKM, Kumar MAS, Krishnan RB, Mohan V, et al. COVID-19 associated rhino-orbital mucormycosis: a single centre experience of ten cases. QJM An Int J Med. 2021. https://doi.org/10.1093/qjmed/hcab176.
Saidha PK, Kapoor S, Das P, Gupta A, Kakkar V, Kumar A, et al. Mucormycosis of paranasal sinuses of odontogenic origin post COVID19 infection: a case series. Indian J Otolaryngol Head Neck Surg. 2021. https://doi.org/10.1007/s12070-021-02638-1.
Jain M, Tyagi R, Tyagi R, Jain G. Post-COVID-19 gastrointestinal invasive mucormycosis. Indian J Surg. 2021. https://doi.org/10.1007/s12262-021-03007-6.
Baskar HC, Chandran A, Reddy CS, Singh S. Rhino-orbital mucormycosis in a COVID-19 patient. BMJ Case Rep. 2021;14:e244232. https://doi.org/10.1136/bcr-2021-244232.
Patankar SH, Joshi AR, Muthe MM, Athawale A, Achhapalia Y. CT and MRI findings of invasive mucormycosis in the setting of COVID-19: experience from a single center in India. Am J Roentgenol. 2021. https://doi.org/10.2214/AJR.21.26205.
Sen M, Honavar SG, Bansal R, Sengupta S, Rao R, Kim U, et al. Epidemiology, clinical profile, management, and outcome of COVID-19-associated rhino-orbital-cerebral mucormycosis in 2826 patients in India - Collaborative OPAI-IJO Study on Mucormycosis in COVID-19 (COSMIC), Report 1. Indian J Ophthalmol. 2021;69:1670–92. https://doi.org/10.4103/ijo.IJO_1565_21.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Al-Tawfiq, J.A., Alhumaid, S., Alshukairi, A.N. et al. COVID-19 and mucormycosis superinfection: the perfect storm. Infection 49, 833–853 (2021). https://doi.org/10.1007/s15010-021-01670-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s15010-021-01670-1