
Abstract
Background
Little is known about current patterns of antithrombotic therapy in patients with atrial fibrillation (AF) undergoing percutaneous coronary intervention (PCI) in clinical practice in Germany.
Methods
The RIVA-PCI is a prospective, non-interventional, multicenter study with follow-up until hospital discharge including consecutive patients with AF undergoing PCI.
Results
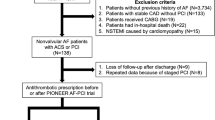
Between January 2018 and March 2020, 1636 patients (elective in 52.6%, non-ST elevation acute coronary syndrome [NSTE-ACS] in 39.3%, ST-elevation myocardial infarction in 8.2%) from 51 German hospitals were enrolled in the study. After PCI a dual antithrombotic therapy (DAT) consisting of OAC and a P2Y12 inhibitor was given to 66.0%, triple antithrombotic therapy (TAT) to 26.0%, dual antiplatelet therapy to 5.5%, and a mono-therapy to 2.5% of the patients. Non-vitamin K antagonist oral anticoagulants (NOACs) were given to 82.4% and vitamin K antagonists to 11.5% of the patients. In-hospital events included death in 12 cases (0.7%), myocardial infarction, stent thrombosis, and ischemic stroke in four (0.2%) patients each, while 2.8% of patients had bleeding complications. The recommended durations for DAT or TAT at discharge were 1 month (1.5%), 3 months (2.1%), 6 months (43.1%), and 12 months (45.6%), with a 6-month course of DAT (47.7%) most often recommended after elective PCI and a 12-month course of DAT (40.1%) after ACS.
Conclusion
The preferred therapy after PCI in patients with AF is DAT with a NOAC and clopidogrel. In-hospital ischemic and bleeding events were rare. The recommended durations for combination therapy vary considerably.
Zusammenfassung
Hintergrund
Über die aktuellen, im klinischen Alltag in Deutschland angewandten Schemata zur antithrombotischen Therapie bei Patienten mit Vorhofflimmern (VF), bei denen eine perkutane Koronarintervention (PCI) durchgeführt wird, ist nur wenig bekannt.
Methoden
Das RIVA-PCI-Register („Rivaroxaban in patients with atrial fibrillation undergoing PCI“) stellt eine prospektive nichtinterventionelle Multizenterstudie mit Nachbeobachtung bis zur Krankenhausentlassung dar und bezieht aufeinanderfolgende Patienten mit VF ein, bei denen eine PCI erfolgt.
Ergebnisse
Zwischen Januar 2018 und März 2020 wurden 1636 Patienten (elektiv in 52,6%, akutes Koronarsyndrom ohne ST-Strecken-Hebung [NSTE-ACS] in 39,3%, ST-Hebungs-Myokardinfarkt in 8,2% der Fälle) aus 51 deutschen Krankenhäusern in die Studie aufgenommen. Nach PCI wurde eine duale antithrombotische Therapie (DAT) mit oralen Antikoagulanzien (OAK) und einem P2Y12-Inhibitor bei 66,0%, eine dreifache („triple“) antithrombotische Therapie (TAT) bei 26,0%, eine duale Plättchenhemmung bei 5,5% und eine Monotherapie bei 2,5% der Patienten durchgeführt. Nicht-Vitamin-K-abhängige orale Antikoagulanzien (NOAC) wurden 82,4% und Vitamin-K-Antagonisten 11,5% der Patienten verordnet. Zu den Ereignissen während des stationären Aufenthalts zählten Tod in 12 Fällen (0,7%), Myokardinfarkt, Stentthrombose und ischämischer Schlaganfall jeweils bei 4 (0,2%) Patienten, während 2,8% der Patienten Blutungskomplikationen aufwiesen. Die empfohlene Dauer für die DAT oder TAT bei Entlassung betrug einen Monat (1,5%), 3 Monate (2,1%), 6 Monate (43,1%) bzw. 12 Monate (45,6%), dabei wurde meistens (47,7%) eine 6‑monatige DAT nach elektiver PCI und eine 12-monatige DAT (40,1%) nach ACS empfohlen.
Schlussfolgerung
Die bevorzugte Therapie nach PCI bei Patienten mit VF besteht in einer DAT mit einem NOAK und Clopidogrel. Ischämische und Blutungsereignisse während des stationären Aufenthalts waren selten. Die empfohlenen Dauern für die Kombinationstherapie variieren beträchtlich.



Similar content being viewed by others


References
Zeymer U, Annemans L, Danchin N et al (2019) Impact of known or new-onset atrial fibrillation on 2‑year cardiovascular event rate in patients with acute coronary syndromes: results from the prospective EPICOR Registry. Eur Heart J Acute Cardiovasc Care 8(2):121–129
Duerschmied D, Brachmann J, Darius H et al (2018) Antithrombotic therapy in patients with non-valvular atrial fibrillation undergoing percutaneous coronary intervention: should we change our practice after the PIONEER AF-PCI and RE-DUAL PCI trials? Clin Res Cardiol 107(7):533–538
Kirchhof P, Benussi S, Kotecha D et al (2016) 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur Heart J 37(38):2893–2962
Schomig A, Neumann FJ, Kastrati A et al (1996) A randomized comparison of antiplatelet and anticoagulant therapy after the placement of coronary-artery stents. N Engl J Med 334(17):1084–1089
Lip GY, Windecker S, Huber K et al (2014) Management of antithrombotic therapy in atrial fibrillation patients presenting with acute coronary syndrome and/or undergoing percutaneous coronary or valve interventions: a joint consensus document of the European Society of Cardiology Working Group on Thrombosis, European Heart Rhythm Association (EHRA), European Association of Percutaneous Cardiovascular Interventions (EAPCI) and European Association of Acute Cardiac Care (ACCA) endorsed by the Heart Rhythm Society (HRS) and Asia-Pacific Heart Rhythm Society (APHRS). Eur Heart J 35(45):3155–3179 (Document Reviewers, Storey RF, Bueno H, Collet JP, Fauchier L, Halvorsen S, Lettino M, Morais J, Mueller C, Potpara TS, Rasmussen LH, Rubboli A, Tamargo J, Valgimigli M, Zamorano JL)
Dewilde WJ, Oirbans T, Verheugt FW et al (2013) Use of clopidogrel with or without aspirin in patients taking oral anticoagulant therapy and undergoing percutaneous coronary intervention: an open-label, randomised, controlled trial. Lancet 381(9872):1107–1115
Gibson CM, Mehran R, Bode C et al (2016) Prevention of bleeding in patients with atrial fibrillation undergoing PCI. N Engl J Med 375(25):2423–2434
Cannon CP, Bhatt DL, Oldgren J et al (2017) Dual antithrombotic therapy with dabigatran after PCI in atrial fibrillation. N Engl J Med 377:1513–1524
Lopes RD, Heizer G, Aronson R et al (2019) Antithrombotic therapy after acute coronary syndrome or PCI in atrial fibrillation. N Engl J Med 380:1509–1524
Vranckx P, Valgimigli M, Eckardt L et al (2019) Edoxaban-based versus vitamin K antagonist-based antithrombotic regimen after successful coronary stenting in patients with atrial fibrillation (ENTRUST-AF PCI): a randomised, open-label, phase 3b trial. Lancet 394:1335–1343
Collet JP, Thiele H, Barbato E et al (2021) 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J 42(14):1289–1367
Cutlip DE, Windecker S, Mehran R et al (2007) Academic Research Consortium. Clinical end points in coronary stent trials: a case for standardized definitions. Circulation 115:2344–2351
Thygesen K, Alpert JS, Jaffe AS et al (2018) Fourth universal definition of myocardial infarction. Eur Heart J. https://doi.org/10.1016/j.gheart.2018.08.004
Schulman S, Kearon C et al (2005) Definition of major bleeding in clinical investigations of antihemostatic medicinal products in non-surgical patients. J Thromb Haemost 3(4):692–694
Mehran R, Rao SV, Bhatt DL et al (2011) Standardized bleeding definitions for cardiovascular clinical trials: a consensus report from the Bleeding Academic Research Consortium. Circulation 123(23):2736–2747
Valgimigli M, Bueno H, Byrne RA et al (2018) 2017 ESC focused update on dual antiplatelet therapy in coronary artery disease developed in collaboration with EACTS. Eur Heart J 39:213–260
Neumann FJ, Sousa-Uva M, Ahlsson A et al (2019) 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur Heart J 40(2):87–165
ACTIVE W Investigators, Connolly S, Pogue J, Hart R et al (2006) Clopidogrel plus aspirin versus oral anticoagulation for atrial fibrillation in the Atrial fibrillation Clopidogrel Trial with Irbesartan for prevention of Vascular Events (ACTIVE W): a randomised controlled trial. Lancet 367(9526):1903–1912
Lopes RD, Leonardi S, Wojdyla DM et al (2020) Stent thrombosis in patients with atrial fibrillation undergoing coronary stenting in the AUGUSTUS Trial. Circulation 141(9):781–783
Knuuti J, Wijns W, Saraste A et al. (2019) ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J 2020(41):407–477
Sarafoff N, Martischnig A, Wealer J et al (2013) Triple therapy with aspirin, prasugrel, and vitamin K antagonists in patients with drug-eluting stent implantation and an indication for oral anticoagulation. J Am Coll Cardiol 61(20):2060–2066
Alexander JH, Wojdyla D, Vora AN et al (2020) The risk/benefit tradeoff of antithrombotic therapy in patients with atrial fibrillation early and late after an acute coronary syndrome or percutaneous coronary intervention: insights from AUGUSTUS. Circulation 141(20):1618–1627
De Luca L, Bolognese L, Rubboli A et al (2021) Combinations of antithrombotic therapies prescribed after percutaneous coronary intervention in patients with acute coronary syndromes and atrial fibrillation: data from the nationwide MATADOR-PCI registry. Eur Heart J Cardiovasc Pharmacother 7(3):e45–e47
de la Torre Hernandez JM, Ferreiro JL, Lopez-Palop R et al (2021) Antithrombotic strategies in elderly patients with atrial fibrillation revascularized with drug-eluting stents: PACO-PCI (EPIC-15) registry. Int J Cardiol. https://doi.org/10.1016/j.ijcard.2021.05.036
Acknowledgements
List of investigators (in the order of the number of enrolled patients): Dr. med. Ralph Toelg, Segeberger Kliniken GmbH, Bad Segeberg; Prof. Dr. med. Harm Wienbergen, Klinikum Links der Weser Bremen, Bremen; Prof. Dr. med. Uwe Zeymer, Klinikum der Stadt Ludwigshafen, Ludwigshafen; Dr. med. Hans-Peter Hobbach, Kreisklinikum Siegen, Siegen; Dr. med. Alessandro Cuneo, Krankenhaus und MVZ Maria-Hilf Stadtlohn, Stadtlohn; Prof. Dr. med. Raffi Bekeredjian, Robert-Bosch-Klinikum, Stuttgart; Prof. Dr. med. OliverRitter, Klinikum Brandenburg Havel, Brandenburg; Prof. Dr. med. Birgit Hailer; Kath. Kliniken Essen-Nord-West gGmbH, Essen; Dr. med. Klaus Hertting, Krankenhaus Buchholz und Winsen GmbH, Buchholz; Prof. Dr. med. Marcus Hennersdorf, SLK-Kliniken Heilbronn GmbH, Heilbronn; Dr. med. Werner Scholz, Herz- und Diabeteszentrum, Bad Oeynhausen; PD. Dr. med. Peter Lanzer, Gesundheitszentrum Bitterfeld Wolfen, Bitterfeld; Prof. Dr. med. Harald Mudra, Städt. Krankenhaus Neuperlach-München, München; Dr. med. Markus Schwefer, Elblandkliniken Stifung & Co. KG Elblandklinikum Riesa, Riesa; Prof. Dr. med. Peter-Lothar Schwimmbeck, Klinikum Leverkusen, Leverkusen; Dr. med. Christoph Liebetrau, Kerckhoff-Klinik GmbH, Bad Nauheim; Dr. med. Steffen Schnupp, Klinikum Coburg, Coburg; Dr. med. Frank Hamann, Klinikum Konstanz, Konstanz; Prof. Dr. med. Rainer Zotz, Marienhausklinikum Bitburg-Neuenburg, Bitburg; Prof. Dr. med. Matthias Leschke, Klinikum Esslingen, Esslingen; Dr. med. Martin Dißmann, Vivantes Humboldt-Klinikum, Berlin; Dr. med. Christoph Kadel, Klinikum Frankfurt Höchst, Frankfurt; PD Dr. med. Michael Gross, Johanniter-Krankenhaus Genthin—Stendal gGmbH, Stendal; Dr. med. Dirk Härtel, Klinikum Lippe-Detmold, Detmold; PD. Dr. med. Sandra Erbs, Herzzentrum Leipzig GmbH, Leipzig; Prof. Dr. med. Ibrahim Akin, Universitätsklinikum Mannheim, Mannheim; Dr. med. Christopher Bengel, MTK Klinikum Bad Soden, Bad Soden; PD Dr. med. Lutz Büllesfeld; GFO Kliniken Bonn, St. Marien-Hospital, Bonn; Prof. Dr. med. Jan Torzewski; Herz- und Gefäßzentrum Oberallgäu-Kempten gGmbH, Kempten; Dr. med. Jan Guggemos, Gemeinschaftskrankenhaus Havelhöhe, Berlin; Prof. Dr. med. Werner Jung, Schwarzwald-Baar Klinikum, Villingen-Schwenningen; PD. Dr. med.Bernhard Witzenbichler, Helios Amper Klinikum Dachau, Dachau; Prof. Dr. med. Florian Bea, Krankenhaus Freudenstadt, Freudenstadt; PD. Dr. med. Marc Kollum, Hegau-Bodensee-Klinikum Singen, Singen; Prof. Dr. med.Rüdiger Dißmann, Klinikum Bremerhaven Reinkenheide, Bremerhaven; Dr. med. Murat Yildiz, Hospital zum Heiligen Geist, Fritzla; Prof. Dr. med. Dirk Sibbing, Klinikum der Universität München-Großhadern, München; Dr. med. Stefan Zimmermann, Klinikum Bayreuth GmbH, Bayreuth; Dr. med. Simon Ohm; Sana Kliniken Düsseldorf GmbH, Düsseldorf, PD Dr. med. Peter Nordbeck, Universitätsklinikum Würzburg, Würzburg; Dr. med. Jan Johannsen, Ostalb-Klinikum Aalen, Aaalen; Dr. med. Felix Schmidt, Klinikum Chemnitz GmbH, KH Küchwald, Chemnitz; Dr. med. Stefan Hoffmann, Klinikum Barnim GmbH Werner Forßmann Krankenhaus, Eberswalde; Dr. med. Bernhard Vieregge, Krankenhaus Neustadt am Rübenberge, Neustadt; Dr. med. Achim Gutersohn, St. Marienhospital Vechta, Vechta; Dr. med. Z. Hatahet, Kreisklinik Altötting, Altötting; Prof. Dr. med. Martin Andrassy, Fürst-Stirum-Klinik, Bruchsal; Dr. med. Norbert Kaul, Stiftungsklinikum Mittelrhein, Koblenz; Dr. med. Norbert Klein, Klinikum St. Georg gGmbH, Leipzig; Prof. Dr. med. Grigorios Korosoglou, GRN-Klinik Weinheim, Weinheim; Dr. med. Oliver Gastmann, Ilm-Kreis-Kliniken, Arnstadt-Ilmenau gGmbH, Arnstadt.
Funding
The RIVA-PCI registry has been supported by an unrestricted grant of the Bayer-Vital GmbH, Germany.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
U. Zeymer: speakers honoraria from Astra Zeneca, Bayer, BMS, Boehringer Ingelheim, Daicchi Sankyo, Pfizer, Sanofi; M. Hennersdorf: speakers honoraria from Astra Zeneca, Bayer, Berlin Chemie, Daiichi Sankyo. H. Wienbergen, H.-P. Hobbach, R. Toelg, A. Cuneo, R. Bekeredjian, O. Ritter, B. Hailer, K. Hertting, W. Scholtz, P. Lanzer, H. Mudra, M. Schwefer, P.‑L. Schwimmbeck, C. Liebetrau, H. Thiele, C. Claas, T. Riemer and R. Zahn declare that they have no competing interests.
For this article no studies with human participants or animals were performed by any of the authors. All studies performed were in accordance with the ethical standards indicated in each case.
Rights and permissions
About this article

Cite this article
Zeymer, U., Toelg, R., Wienbergen, H. et al. Current status of antithrombotic therapy and in-hospital outcomes in patients with atrial fibrillation undergoing percutaneous coronary intervention in Germany. Herz 48, 134–140 (2023). https://doi.org/10.1007/s00059-022-05099-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00059-022-05099-6
Keywords
- Atrial fibrillation
- Antithrombotic therapy
- Oral anticoagulation
- Percutaneous coronary intervention
- Registry