
Abstract
Purpose
Hyperglycaemia is common in the critically ill. The objectives of this study were to determine the prevalence of critical illness-associated hyperglycaemia (CIAH) and recognised and unrecognised diabetes in the critically ill as well as to evaluate the impact of premorbid glycaemia on the association between acute hyperglycaemia and mortality.
Methods
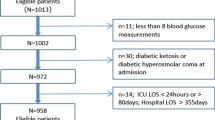
In 1,000 consecutively admitted patients we prospectively measured glycated haemoglobin (HbA1c) on admission, and blood glucose concentrations during the 48 h after admission, to the intensive care unit. Patients with blood glucose ≥7.0 mmol/l when fasting or ≥11.1 mmol/l during feeding were deemed hyperglycaemic. Patients with acute hyperglycaemia and HbA1c <6.5 % (48 mmol/mol) were categorised as ‘CIAH’, those with known diabetes as ‘recognised diabetes’, and those with HbA1c ≥6.5 % but no previous diagnosis of diabetes as ‘unrecognised diabetes’. The remainder were classified as ‘normoglycaemic’. Hospital mortality, HbA1c and acute peak glycaemia were assessed using a logistic regression model.
Results
Of 1,000 patients, 498 (49.8 %) had CIAH, 220 (22 %) had recognised diabetes, 55 (5.5 %) had unrecognised diabetes and 227 (22.7 %) were normoglycaemic. The risk of death increased by approximately 20 % for each increase in acute glycaemia of 1 mmol/l in patients with CIAH and those with diabetes and HbA1c levels <7 % (53 mmol/mol), but not in patients with diabetes and HbA1c ≥7 %. This association was lost when adjusted for severity of illness.
Conclusions
Critical illness-associated hyperglycaemia is the most frequent cause of hyperglycaemia in the critically ill. Peak glucose concentrations during critical illness are associated with increased mortality in patients with adequate premorbid glycaemic control, but not in patients with premorbid hyperglycaemia. Optimal glucose thresholds in the critically ill may, therefore, be affected by premorbid glycaemia.

Similar content being viewed by others

Abbreviations
- ADA:
-
American Diabetes Association
- ANOVA:
-
Analysis of variance
- APACHE:
-
Acute physiology and chronic health evaluation
- BMI:
-
Body mass index
- CIAH:
-
Critical illness-associated hyperglycaemia
- EASD:
-
European Association for the Study of Diabetes
- HbA1c :
-
Glycated haemoglobin
- ICU:
-
Intensive care unit
- OGTT:
-
Oral glucose tolerance test
References
Dungan KM, Braithwaite SS, Preiser JC (2009) Stress hyperglycaemia. Lancet 373:1798–1807
Deane AM, Horowitz M (2013) Dysglycaemia in the critically ill-significance and management. Diabetes Obes Metab 15:792–801
Cely CM, Arora P, Quartin AA, Kett DH, Schein RM (2004) Relationship of baseline glucose homeostasis to hyperglycemia during medical critical illness. Chest 126:879–887
Umpierrez GE, Isaacs SD, Bazargan N, You X, Thaler LM, Kitabchi AE (2002) Hyperglycemia: an independent marker of in-hospital mortality in patients with undiagnosed diabetes. J Clin Endocrinol Metab 87:978–982
Rady MY, Johnson DJ, Patel BM, Larson JS, Helmers RA (2005) Influence of individual characteristics on outcome of glycemic control in intensive care unit patients with or without diabetes mellitus. Mayo Clin Proc 80:1558–1567
Van den Berghe G, Wilmer A, Milants I, Wouters PJ, Bouckaert B, Bruyninckx F, Bouillon R, Schetz M (2006) Intensive insulin therapy in mixed medical/surgical intensive care units: benefit versus harm. Diabetes 55:3151–3159
Egi M, Bellomo R, Stachowski E, French CJ, Hart GK, Hegarty C, Bailey M (2008) Blood glucose concentration and outcome of critical illness: the impact of diabetes. Crit Care Med 36:2249–2255
Vincent JL, Preiser JC, Sprung CL, Moreno R, Sakr Y (2010) Insulin-treated diabetes is not associated with increased mortality in critically ill patients. Crit Care 14:R12
Falciglia M, Freyberg RW, Almenoff PL, D’Alessio DA, Render ML (2009) Hyperglycemia-related mortality in critically ill patients varies with admission diagnosis. Crit Care Med 37:3001–3009
Krinsley JS, Egi M, Kiss A, Devendra AN, Schuetz P, Maurer PM, Schultz MJ, van Hooijdonk RT, Kiyoshi M, Mackenzie IM, Annane D, Stow P, Nasraway SA, Holewinski S, Holzinger U, Preiser JC, Vincent JL, Bellomo R (2013) Diabetic status and the relation of the three domains of glycemic control to mortality in critically ill patients: an international multicenter cohort study. Crit Care 17:R37
Krinsley JS (2006) Glycemic control, diabetic status, and mortality in a heterogeneous population of critically ill patients before and during the era of intensive glycemic management: six and one-half years experience at a university-affiliated community hospital. Semin Thorac Cardiovasc Surg 18:317–325
Inzucchi SE, Bergenstal RM, Buse JB, Diamant M, Ferrannini E, Nauck M, Peters AL, Tsapas A, Wender R, Matthews DR, American Diabetes Association & European Association for the Study of Diabetes (2012) Management of hyperglycemia in type 2 diabetes: a patient-centered approach: position statement of the American Diabetes Association (ADA) and the European Association for the Study of diabetes (EASD). Diabetes Care 35:1364–1379
Keegan MT, Goldberg ME, Torjman MC, Coursin DB (2009) Perioperative and critical illness dysglycemia–controlling the iceberg. J Diabetes Sci Technol 3:1288–1291
Krinsley JS, Meyfroidt G, van den Berghe G, Egi M, Bellomo R (2012) The impact of premorbid diabetic status on the relationship between the three domains of glycemic control and mortality in critically ill patients. Curr Opin Clin Nutr Metab Care 15:151–160
Clement S, Braithwaite SS, Magee MF, Ahmann A, Smith EP, Schafer RG, Hirsch IB, American Diabetes Association Diabetes in Hospitals Writing Committee (2004) Management of diabetes and hyperglycemia in hospitals. Diabetes Care 27:553–591
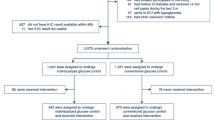
NICE-SUGAR Study Investigators, Finfer S, Chittock DR, Su SY, Blair D, Foster D, Dhingra V, Bellomo R, Cook D, Dodek P, Henderson WR, Hebert PC, Heritier S, Heyland DK, McArthur C, McDonald E, Mitchell I, Myburgh JA, Norton R, Potter J, Robinson BG, Ronco JJ (2009) Intensive versus conventional glucose control in critically ill patients. N Engl J Med 360:1283–1297
Alberti KGMM, Zimmet PZ (1998) Definition, diagnosis and classification of diabetes mellitus and its complications. part 1: diagnosis and classification of diabetes mellitus. Provisional report of a WHO consultation. Diabet Med 15:539–553
van den Berghe G, Wouters P, Weekers F, Verwaest C, Bruyninckx F, Schetz M, Vlasselaers D, Ferdinande P, Lauwers P, Bouillon R (2001) Intensive insulin therapy in critically ill patients. N Engl J Med 345:1359–1367
Preiser JC, Devos P, Ruiz-Santana S, Melot C, Annane D, Groeneveld J, Iapichino G, Leverve X, Nitenberg G, Singer P, Wernerman J, Joannidis M, Stecher A, Chiolero R (2009) A prospective randomised multi-centre controlled trial on tight glucose control by intensive insulin therapy in adult intensive care units: the Glucontrol study. Intensive Care Med 35:1738–1748
Gornik I, Vujaklija-Brajkovic A, Renar IP, Gasparovic V (2010) A prospective observational study of the relationship of critical illness associated hyperglycaemia in medical ICU patients and subsequent development of type 2 diabetes. Crit Care 14:R130
American Diabetes Association (2013) Diagnosis and classification of diabetes mellitus. Diabetes Care 36(Suppl 1):S67–S74
Horowitz M, O’Donovan D, Jones KL, Feinle C, Rayner CK, Samsom M (2002) Gastric emptying in diabetes: clinical significance and treatment. Diabet Med 19:177–194
Chapman MJ, Nguyen NQ, Deane AM (2013) Gastrointestinal dysmotility: evidence and clinical management. Curr Opin Clin Nutr Metab Care 16:209–216
Dunstan DW, Zimmet PZ, Welborn TA, De Courten MP, Cameron AJ, Sicree RA, Dwyer T, Colagiuri S, Jolley D, Knuiman M, Atkins R, Shaw JE (2002) The rising prevalence of diabetes and impaired glucose tolerance: the Australian diabetes, obesity and lifestyle study. Diabetes Care 25:829–834
Kosiborod M, Inzucchi SE, Krumholz HM, Xiao L, Jones PG, Fiske S, Masoudi FA, Marso SP, Spertus JA (2008) Glucometrics in patients hospitalized with acute myocardial infarction: defining the optimal outcomes-based measure of risk. Circulation 117:1018–1027
Stegenga ME, Vincent JL, Vail GM, Xie J, Haney DJ, Williams MD, Bernard GR, van der Poll T (2010) Diabetes does not alter mortality or hemostatic and inflammatory responses in patients with severe sepsis. Crit Care Med 38:539–545
Egi M, Bellomo R, Stachowski E, French CJ, Hart GK, Taori G, Hegarty C, Bailey M (2011) The interaction of chronic and acute glycemia with mortality in critically ill patients with diabetes. Crit Care Med 39:105–111
Capes SE, Hunt D, Malmberg K, Gerstein HC (2000) Stress hyperglycaemia and increased risk of death after myocardial infarction in patients with and without diabetes: a systematic overview. Lancet 355:773–778
McGinn JT Jr, Shariff MA, Bhat TM, Azab B, Molloy WJ, Quattrocchi E, Farid M, Eichorn AM, Dlugacz YD, Silverman RA (2011) Prevalence of dysglycemia among coronary artery bypass surgery patients with no previous diabetic history. J Cardiothorac Surg 6:104
Wexler DJ, Nathan DM, Grant RW, Regan S, Van Leuvan AL, Cagliero E (2008) Prevalence of elevated hemoglobin A1c among patients admitted to the hospital without a diagnosis of diabetes. J Clin Endocrinol Metab 93:4238–4244
Sacks DB (2012) Measurement of hemoglobin A(1c): a new twist on the path to harmony. Diabetes Care 35:2674–2680
Sacks DB (2013) Hemoglobin A1c in diabetes: panacea or pointless? Diabetes 62:41–43
Antonelli M, Bonten M, Chastre J, Citerio G, Conti G, Curtis JR, De Backer D, Hedenstierna G, Joannidis M, Macrae D, Mancebo J, Maggiore SM, Mebazaa A, Preiser JC, Rocco P, Timsit JF, Wernerman J, Zhang H (2012) Year in review in intensive care medicine 2011: I. nephrology, epidemiology, nutrition and therapeutics, neurology, ethical and legal issues, experimentals. Intensive Care Med 38:192–209
Egi M, Bellomo R, Stachowski E, French CJ, Hart G, Stow P (2006) Blood glucose on day of intensive care unit admission as a surrogate of subsequent glucose control in intensive care. J Crit Care 21:197–202
Schlenk F, Graetz D, Nagel A, Schmidt M, Sarrafzadeh AS (2008) Insulin-related decrease in cerebral glucose despite normoglycemia in aneurysmal subarachnoid hemorrhage. Crit Care 12:R9
Acknowledgments
The authors acknowledge the assistance of biostatiscians Ms Kylie Lange and Ms Suzanne Edwards (University of Adelaide). Dr. Mark Plummer is supported by a Dawes Scholarship (co-funded University of Adelaide and Royal Adelaide Hospital) and Dr. Adam Deane is supported by a National Health and Medical Research Council of Australia (NHMRC) Early Career Fellowship. Data collection was supported by a project grant from the Diabetes Australia Research Trust. These data were presented in abstract form at the European Society of Intensive Care Medicine 26th Annual Congress (Paris).
Conflicts of interest
M.H. has participated in advisory boards and/or symposia for Novo/Nordisk, Sanofl-Aventis, Novartis, Eli-Lilly, Boehringer Ingelheim, AstraZeneca, Satlogen and Meyer Nutraceuticals. M.P.P., R.B., C.E.C., C.E.A., K.S., B.J.R., J.P.R., M.J.C and A.M.D have no duality of interests to declare.
Author information
Authors and Affiliations
Corresponding author
Additional information
Take-home message: Peak glucose concentrations during critical illness are associated with increased mortality in patients with adequate premorbid glycaemic control, but not in patients with premorbid hyperglycaemia as determined by HbA1c. Optimal glucose thresholds in the critically ill may, therefore, be affected by premorbid glycaemia so that clinicians should consider the admission HbA1c when targeting glycaemic control.
Electronic supplementary material
Below is the link to the electronic supplementary material.
134_2014_3287_MOESM1_ESM.png
Fig. 1. Hospital mortality vs acute glycaemia when categorised according to premorbid glycaemia (HbA1c) adjusted for age, BMI, APACHE II and admission type (medical/surgical). After adjustment the interaction term peak BGL*HbA1c interaction was no longer significant (P = 0.13). The model was an adequate fit (Hosmer and Lemeshow goodness of fit test). Slope estimates for each category were HbA1c < 6 % (42 mmol/mol), odds ratio = 1.05 (95 % CI 0.97, 1.13), P = 0.22; 6 % ≤ HbA1c < 7 % (53 mmol/mol), odds ratio = 1.13 (95 % CI 1.02, 1.25), P = 0.016; and HbA1c ≥ 7 %, odds ratio = 0.97 (95 % CI 0.86, 1.09), P = 0.575.(PNG 731 kb)
Rights and permissions
About this article

{kind=link}
Cite this article
Plummer, M.P., Bellomo, R., Cousins, C.E. et al. Dysglycaemia in the critically ill and the interaction of chronic and acute glycaemia with mortality. Intensive Care Med 40, 973–980 (2014). https://doi.org/10.1007/s00134-014-3287-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-014-3287-7