
Abstract
Summary
We examined whether low income was associated with an increased likelihood of treatment qualification for osteoporotic fracture probability determined by Canada FRAX in women aged ≥50 years. A significant negative linear association was observed between income and treatment qualification when FRAX included bone mineral density (BMD), which may have implications for clinical practice.
Introduction
Lower income has been associated with increased fracture risk. We examined whether lower income in women was associated with an increased likelihood of treatment qualification determined by Canada FRAX®.
Methods
We calculated 10-year FRAX probabilities in 51,327 Canadian women aged ≥50 years undergoing baseline BMD measured by dual energy x-ray absorptiometry 1996–2001. FRAX probabilities for hip fracture ≥3 % or major osteoporotic fracture (MOF) ≥20 % were used to define treatment qualification. Mean household income from Canada Census 2006 public use files was used to categorize the population into quintiles. Logistic regression analyses were used to model the association between income and treatment qualification.
Results
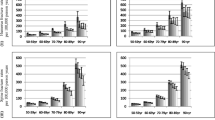
Percentages of women who qualified for treatment based upon high hip fracture probability increased linearly with declining income quintile (all p trend <0.001), but this was partially explained by older age among lower income quintiles (p trend <0.001). Compared to the highest income quintile, women in the lowest income quintile had a greater likelihood of treatment qualification based upon high hip fracture probability determined with BMD (age-adjusted odds ratio [OR], 1.34; 95 % confidence intervals (CI), 1.23–1.47) or high MOF fracture probability determined with BMD (age-adjusted OR, 1.31; 95 % CI, 1.18–1.46). Differences were nonsignificant when FRAX was determined without BMD, implying that BMD differences may be the primary explanatory factor.
Conclusions
FRAX determined with BMD identifies a larger proportion of lower income women as qualifying for treatment than higher income women.


Similar content being viewed by others


References
Wilkinson RG, Marmot MG (eds) (1998) Social determinants of health: the solid facts. WHO European Region, Copenhagen
Wilkinson R, Pickett K (2009) The Spirit level: Why more equal societies almost always do better. Allen Lane, London, UK
Meyer HE, Henriksen C, Falch JA, Pedersen JI, Tverdal A (1995) Risk factors for hip fracture in a high incidence area: a case–control study from Oslo, Norway. Osteoporos Int 5:239–246
Bacon WE, Hadden WC (2000) Occurrence of hip fractures and socioeconomic position. J Aging Health 12:193–203
Farahmand BY, Persson PG, Michaelsson K, Baron JA, Parker MG, Ljunghall S (2000) Socioeconomic status, marital status and hip fracture risk: a population-based case–control study. Osteoporos Int 11:803–808
Brennan SL, Henry MJ, Kotowicz MA, Nicholson GC, Zhang Y, Pasco JA (2011) Incident hip fracture and social disadvantage in an Australian population aged 50 years or greater. Bone 48:607–610
Jones S, Johansen A, Brennan J, Butler J, Lyons RA (2004) The effect of socioeconomic deprivation on fracture incidence in the United Kingdom. Osteoporos Int 15:520–524
Zingmond DS, Soohoo NF, Silverman SL (2006) The role of socioeconomic status on hip fracture. Osteoporos Int 17:1562–1568
Guilley E, Herrmann F, Rapin C-H, Hoffmeyer P, Rizzoli R, Chevalley T (2010) Socioeconomic and living conditions are determinants of hip fracture incidence and age occurrence among community-dwelling elderly. Osteoporos Int 18:2010
Icks A, Haastert B, Wildner M, Becker C, Rapp K, Dragano N, Meyer G, Rosenbauer J (2009) Hip fractures and area level socioeconomic conditions: a population-based study. BMC Public Health 9:1,471
Wilson R, Chase GA, Chrischilles EA, Wallace RB (2006) Hip fracture risk among community-dwelling elderly people in the United States: a prospective study of physical, cognitive and socioeconomic indicators. Am J Public Health 96:1210–1218
Johnell O, Borgstrom F, Jonsson B, Kanis J (2007) Latitude, socioeconomic prosperity, mobile phones and hip fracture risk. Osteoporos Int 18:333–337
Syddall HE, Evandrou M, Dennison EM, Cooper C, Sayer AA (2012) Social inequalities in osteoporosis and fracture among community-dwelling older men and women: findings from the Hertfordshire cohort study. Arch Osteoporos 7:37–48
Kanis JA, Oden A, Johansson H, Borgstrom F, Strom O, McCloskey E (2009) FRAX and its applications to clinical practice. Bone 44:734–743
Ward H, Tarasuk V, Mendelson R, McKeown-Eyssen G (2007) An exploration of socioeconomic variation in lifestyle factors and adiposity in the Ontario Food Survey through structural equation modeling. Int J Behav Nutr Physical Activity 4:5864–5868
Anand SS, Razak F, Davis AD, Jacobs R, Vuksan V, Teo K, Yusuf S (2006) Social disadvantage and cardiovascular disease: development of an index and analysis of age, sex, and ethnicity effects. Int J Epidemiol 35:1239–1245
Leslie WD, Morin S, Lix LM, Johansson H, Oden A, McCloskey E, Kanis JA, For the Manitoba Bone Density Program (2011) Fracture risk assessment without bone density measurement in routine clinical practice. Osteoporos Int 23:75–85
Brennan SL, Leslie WD, Lix LM (2012) Associations between adverse social position and bone mineral density in women aged 50 years or older: data from the Manitoba Bone Density Program. Osteoporos Int(February)
Papaioannou A, Morin S, Cheung AM, Atkinson S, Brown JP, Feldman S et al (2010) 2010 clinical practice guidelines for the diagnosis and management of osteoporosis in Canada: summary. CMAJ 182:1864–1873
Dawson-Hughes B, Tosteson AN, Melton LJ (2008) Implications of absolute fracture risk assessment for osteoporosis practice guidelines in the USA. Osteoporos Int 19:449
Dawson-Hughes B, Looker AC, Tosteson AN, Johansson H, Kanis JA, Melton LJ III (2009) The potential impact of new National Osteoporosis Foundation guidance on treatment patterns. Osteoporos Int.
Roos NP, Shapiro E (1999) Revisiting the Manitoba Centre for Health Policy and Evaluation and its population-based health information system. Med Care 37:JS10–JS14
Roos NP (1999) Establishing a population data-based policy unit. Med Care 37
Leslie WD, Metge C (2003) Establishing a regional bone density program: lessons from the Manitoba experience. J Clin Densitom 6:275–282
Leslie WD, Lix LM, Johansson H, Oden A, McCloskey E, Kanis JA, Manitoba Bone Density Program (2010) Independent clinical validation of a Canadian FRAX tool: fracture prediction and model calibration. J Bone Miner Res 25:2350–2358
Leslie WD, Majumdar SR, Lix LM, Johansson H, Oden A, McCloskey E, Kanis JA, Manitoba Bone Density Program (2012) High fracture probability with FRAX usually indicates densitometric osteoporosis: implications for clinical practice. Osteoporos Int 23:391–397
Demeter S, Leslie WD, Lix L, MacWilliam L, Finlayson GS, Reed M (2007) The effect of socioeconomic status on bone density testing in a public health-care system. Osteoporos Int 18:153–158
Demeter S, Reed M, Lix L, MacWilliam L, Leslie WD (2005) Socioeconomic status and the utilization of diagnostic imaging in an urban setting. CMAJ 173:1173–1177
Neuner JM, Zhang X, Sparapani R, Laud PW, Nattinger AB (2007) Racial and socioeconomic disparities in bone density testing before and after hip fracture. J Gen Int Med 22:1239–1245
Ellis J, Mullan J, Worsley A, Pai N (2012) The role of health literacy and social networks in arthritis patients' health information-seeking behavior: A qualitative study. Int J Family Med doi: 10.1155/2012/397039:6 pages.
Buchbinder R, Batterham R, Ciciriello S, Newman S, Horgan B, Ueffing E, Rader T, Tugwell PS, Osborne RH (2011) Health literacy: What is it and why is it important to measure? J Rheumatol 38:1791–1797
Williams J, Clemens S, Oleinikova K, Tarvin K (2003) The skills for life survey: a national needs and impact survey of literacy, numeracy and ICT skills. In Skills Department for Education and Skills (ed). DES, London.
White S (2008) Assessing the nation's health literacy. Key concepts and findings of the National Assessment of Adult Literacy (NAAL). In. AMA, US.
(2007) Health literacy in Canada: Initial results from the International Adult Literacy and Skills Survey 2007. In. Canadian Council on Learning, Ottawa, ON.
Cook PF, Emiliozzi S, McCabe MM (2007) Telephone counseling to improve osteoporosis treatment adherence: an effectiveness study in community practice settings. Am J Med Qual 22:445–456
Warriner AH, Curtis JR (2009) Adherence to osteoporosis treatments: room for improvement. Curr Opin Rheumatol 21:356–362
Mustard CA, Derksen S, Berthelot JM, Wolfson M (1999) Assessing ecologic proxies for household income: a comparison of household and neighbourhood level income measures in the study of population health status. Health Place 5:157–171
Acknowledgments
The authors are indebted to Manitoba Health for the provision of data (HIPC File Number 2012/2013-15). The results and conclusions are those of the authors, and no official endorsement by Manitoba Health is intended or should be inferred. This article has been reviewed and approved by the members of the Manitoba Bone Density Program Committee. SL Brennan is supported by a National Health and Medical Research Council (NHMRC) of Australia Early Career Fellowship (1012472) and a 2012 Dyason Fellowship from The University of Melbourne. LM Lix is supported by a Manitoba Research Chair.
Conflicts of interest
Sharon L Brennan has no disclosures. William D Leslie has served on advisory boards for Novartis, Amgen, and Genzyme and received unrestricted research grants and speaker fees from Amgen. Lisa M Lix has received an unrestricted research grant from Amgen.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Brennan, S.L., Leslie, W.D. & Lix, L.M. Is lower income associated with an increased likelihood of qualification for treatment for osteoporosis in Canadian women?. Osteoporos Int 25, 273–279 (2014). https://doi.org/10.1007/s00198-013-2467-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-013-2467-6