
Abstract
Few older adults regain their pre-fracture mobility after a hip fracture. Intervention studies evaluating effects on gait typically use short clinical tests or in-lab parameters that are often limited to gait speed only. Measurements of mobility in daily life settings exist and should be considered to a greater extent than today. Less than half of hip fracture patients regain their pre-fracture mobility. Mobility recovery is closely linked to health status and quality of life, but there is no comprehensive overview of how gait has been evaluated in intervention studies on hip fracture patients. The purpose was to identify what gait parameters have been used in randomized controlled trials to assess intervention effects on older people’s mobility recovery after hip fracture. This scoping review is a secondary paper that identified relevant peer-reviewed and grey literature from 11 databases. After abstract and full-text screening, 24 papers from the original review and 8 from an updated search and manual screening were included. Records were eligible if they included gait parameters in RCTs on hip fracture patients. We included 32 papers from 29 trials (2754 unique participants). Gait parameters were primary endpoint in six studies only. Gait was predominantly evaluated as short walking, with gait speed being most frequently studied. Only five studies reported gait parameters from wearable sensors. Evidence on mobility improvement after interventions in hip fracture patients is largely limited to gait speed as assessed in a controlled setting. The transition from traditional clinical and in-lab to out-of-lab gait assessment is needed to assess effects of interventions on mobility recovery after hip fracture at higher granularity in all aspects of patients’ lives, so that optimal care pathways can be defined.
Similar content being viewed by others


Introduction
The burden of hip fracture is high for the individual, the society, and the healthcare system. Each year, there are 1.6 million hip fractures worldwide, with the projected estimates rising to 6 million hip fractures by 2050 [1]. The global burden of hip fracture, one of the most serious consequences of osteoporosis [2], is estimated at 1.75 million disability adjusted life years lost [3], with high mortality, incident or aggravated disability, and need for long-term care [4, 5]. A hip fracture causes a sudden loss of function and optimization of care should start immediately [6]. After surgery, rehabilitation starts with the primary aim to get people back on their feet and mobile again. There are currently no pharmaceutical interventions available to improve mobility. Multidisciplinary hospital treatment including rapid mobilization is suggested as the first essential step for optimization of care immediately after a hip fracture [7, 8], with subsequent subacute exercise interventions to improve mobility [9]. Mobility may be further improved by interventions starting when rehabilitation periods typically end in most countries [10,11,12,13,14]. Significant predictors of poor functional outcomes include multiple medical, surgical, socioeconomic ,and system predictors, such as hand grip strength and frailty as two emerging ones in most recent literature [15]. To better understand the effects and consequences of all these diverse factors so that optimal care pathways can be defined, there is a need to accurately measure and describe mobility outcomes [11]. This need was already highlighted in the recommended core outcome set for hip fracture trials that included mobility as one of five recommended domains [16].
A recent Cochrane review including 40 randomized controlled trials (RCTs) evaluated rehabilitation for improving mobility after hip fracture [17]. The report concluded that it may be possible to gain clinically meaningful improvements in mobility in orthogeriatric hospitals and post-hospital settings, compared with conventional care. However, the Cochrane review focused mostly on high-level outcomes such as survival and care home admission. Potential effects on levels of physical mobility at a more granular level such as gait volume or gait quality were not evaluated. Although there are various methods available to quantify gait in controlled settings, these mostly provide snapshot performances that do not adequately reflect mobility in the real-world. Recently, digital mobility outcomes (DMOs) derived from sensor-based activity monitoring are increasingly being used as a means to capture mobility reliably and directly, both in controlled and in real-world settings [18]. DMOs refer to objectively derived measures from electronic systems in contrast to qualitative, paper-based, or self-reported measures [19], and DMOs representing walking after hip fracture could potentially be gait speed, step counts, cadence, step length, upright time, or activity patterns. However, there is no overarching review of the literature in this field of interest. Despite the obvious significance of mobility for hip fracture recovery, it is unclear to what extent gait parameters have been included in studies to evaluate intervention effects in hip fracture patients. Thus, the objective of this scoping review was to identify gait parameters including DMOs used in randomized controlled trials (RCTs) to assess the effect of interventions on mobility recovery after a hip fracture in older people.
Method
Protocol
The present review is an update and extension of an earlier scoping review performed by the Mobilise-D consortium that mapped existing evidence on the clinical utility of digital mobility outcomes (DMOs) in four patient populations [20]. In the present review, we describe studies that have used gait parameters, including DMOs, as primary, secondary, or exploratory endpoints in RCT studies on patients recovering from proximal femoral fracture (PFF). We followed the scoping review framework and protocol described in Polhemus et al. [20] and used the PRISMA statement as guide for writing this review.
Identifying relevant studies
The search strategy to identify relevant studies in the earlier scoping review has been described elsewhere [19, 20]. The study was registered through the Center for Open Science’s OSFRegistry (https://osf.io/k7395). In November 2019 and again in July 2021, a librarian searched for relevant studies between January 1999 and July 2021 in eleven databases for scientific and gray literature (MEDLINE, EMBASE, CINAHL, Cochrane Library, Scopus, Web of Science, IEEE Xplore, ACM Digital Library, ProQuest Dissertations, OpenGrey, National Information Center’s Projects in Progress Database). Similar searches were conducted in Google Scholar, while references for additional relevant studies up to December 2022 were collated manually. Search details are published as supplementary files for the primary publication and in the project repository [20, 21].
Selecting studies and charting the data
To be eligible, RCTs had to be conducted on participants with proximal femoral fracture and with a gait parameter as primary, secondary, or exploratory endpoint. Gait parameters were pre-defined in a list by internal panels of clinical, technical, and research experts, and a lower limit of 10 patients per study arm was set [20]. All interventions performed during hospital stay or after discharge were analyzed, whatever the control condition (another intervention, control, or sham condition), the delay between the surgery and the start of intervention, the duration of the studies, the length of follow-up, and settings. Only studies for which results were reported in English, German, Spanish, French, Italian, Portuguese, Danish, Norwegian, Swedish, Hebrew, Dutch, Catalan, and Russian were eligible. Conference abstracts were not eligible for inclusion.
After duplicate removal and training of all reviewers, we assessed eligibility through abstract and full-text screening. Consistency checks were performed before each screening phase. First, two reviewers independently screened titles and abstracts of the citations retrieved to identify potential eligible publications. The full-text documents were obtained and independently evaluated by two reviewers applying the full set of inclusion and exclusion criteria. Disagreements were resolved by consensus and by involving a third reviewer. Where different records from the same RCT were identified, they were treated as separate papers in the analyses. We used DistillerSR (Evidence Partners, Ottawa, Canada) and Cadima (Julius Kühn-Institut, Quedlinburg, Germany) for record screening and data management.
Data extraction and risk of bias assessment
We extracted information on study characteristics from each included study, including author; year of publication; country of study; type of intervention; timing of the initiation of intervention after surgery; duration of intervention; number of participants at baseline and at the end of the trial; description of gait outcomes and whether they were primary, secondary, or exploratory endpoints; gait assessment method (including equipment); time of the first gait assessment; and reported gait speed (m/sec) at first gait assessment (including instruction of speed) [22].
Data analysis
Data analysis consisted of a descriptive analysis, reporting on the general study information, interventions (context), gait parameters reported (purposes), and the overall results from the risk of bias assessment. The intervention arms in the RCTs are described in terms of type, consisting of surgical methods, exercise alone, exercise combined with another intervention, or other interventions. We also included an overview of the initiation (at admission, during hospital stay, early and late in the hip fracture trajectory) and duration of the interventions. The gait parameters are described in terms of test procedure, equipment used, and outcome measures reported, including which of the gait parameters were used as primary or secondary outcomes (or alternatively not specified).
Funding source
Part of the research was supported by the Mobilise-D project that has received funding from the Innovative Medicines Initiative 2 Joint Undertaking (JU) under grant agreement No. 820820. This JU receives support from the European Union’s Horizon 2020 research and innovation program and the European Federation of Pharmaceutical Industries and Associations (EFPIA).
Results
Study selection
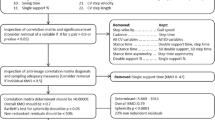
For the full-text review, we included 24 papers on PFF participants identified in the original scoping review [20]. The updated search and subsequent abstract screening of 275 new records added an additional 40 records, providing a total of 68 records for the full-text review, along with three additional papers resulting from a manual check. Of these, we included 32 papers from 29 different RCTs in the current review. The flowchart of study selection is presented in Fig. 1.

PRISMA 2020 flow diagram for updated systematic review including searches of databases, registers and other sources
Study characteristics
This review is based on 32 papers from 29 RCTs, with a combined total of 3648 participants (2754 unique participants). The study citations and key characteristics are presented in Table 1. The publication dates range from 2001 [26] to 2022 [29]. Participants in Sylliaas et al. [37] were a subset of the participants in Sylliaas et al. [36], with 100 of the original 150 participants included in the second phase of this two-phased RCT. Participants in three of the papers [49,50,51] were from the same RCT. Participants in the intervention group of Shi et al. [47] had the lowest mean age of 73.5 years, and the intervention group of Taraldsen and Thingstad et al. [9] had the highest mean age of 84.0 years.
Description of the interventions
The included RCTs varied widely in type of interventions (exercise alone, exercise combined with another intervention, and other non-exercise interventions) and timing of the intervention (at admission, during hospital stay, subacute, or later after hip fracture). Seventeen studies evaluated exercise interventions, two evaluated exercises combined with a second intervention, and eleven trials evaluated other types of interventions (see Table 1).
The seventeen studies reporting on exercise alone interventions included one early in-hospital exercise intervention in bed [32], seven subacute exercise interventions after discharge from hospital or during inpatient rehabilitation before 5 months [26, 27, 29, 33, 35, 36, 38], and nine exercise interventions starting either after ending the “routine” physical therapy or usual care [9, 23, 25, 34] or more than 5 months after the fracture [24, 28, 30, 31, 37]. Two studies reported on exercise combined with nutrition therapy [39] or education [40].
The remaining intervention studies included three drug trials [41,42,43], two magnetic or neuromuscular stimulation trials [44, 45], three trials evaluating different surgical methods [46,47,48], and one trial evaluating in-hospital geriatric treatment [49,50,51]. The longest follow-up was 17 years or until death in one of the interventions evaluating surgical methods [48]. The two remaining studies evaluated interventions using telephone follow-up, where one trial combined usual care with discharge coaching [52], and the other used motivational interviewing [53].
Gait tests and parameters
Gait was largely assessed during short walking distances, ranging from 3- to 15.25-m walks across studies (see Table 1). The methods for collecting gait parameters consisted mostly of simple standardized walk tests with equipment such as a stopwatch. Only eight out of 32 studies reported gait parameters from longer walks, i.e., more than 20 m or at least 3 min, measured using a GaitRite electronic mat [9, 51], a 30-m corridor test [42], a 30-m gait analysis [48], or longer recordings from accelerometer-based sensors (activPAL) [9, 33, 49, 50, 53], with one of these studies from an early in-hospital setting [49].
Gait speed was the most frequently reported gait parameter, in 28 out of 32 papers, with gait speed reported for the populations as low as 0.09 m/s during fast speed instruction 2 weeks after the fracture [35] (see Table 1). Fourteen of these 28 papers used normal gait speed instruction, seven used fast or maximum gait speed instruction, one used both normal and fast gait speed instructions, while the remaining six papers did not specify any particular gait speed instruction. Only three of the 32 papers included additional gait parameters from gait analysis, such as step length, cadence, double support time, single support time, base of support, percentage of single support, step width, walk ratio (step length/cadence), standard deviation of step velocity, single support asymmetry, swing time, steps per second, or step length for affected and non-affected leg [9, 35, 51]. One study included the distance walked during a 6-min walk test in addition to gait speed [29]. Five papers included accelerometer-based sensors and reported outcomes from real-world settings, reporting on daily steps, daily walking time, daily upright time, number of upright events, and length of upright events [9, 33, 49, 50, 53].
How long after the hip fracture gait was tested varied widely across the papers included in this review, and thus the gait speeds reported vary widely as well. Plotting the range of gait speeds (from instructed comfortable gait speeds) reported in the studies against the different phases of the post fracture period (see Fig. 2) indicates that gait speed in the acute phase is extremely low (< 0.3 m/s) and seems to steadily increase throughout the recovery period. The studies conducted at the chronic phase, 53 weeks or more after hip fracture, show levels of gait speed closer to normative data for older adults. Two of the papers report surprisingly high gait speeds of 1.6 m/sec (SD 0.2) for the intervention groups at 14 days [46] and 3 months post-surgery [47]. These are not included in Fig. 2.

Range of comfortable gait speeds reported after hip fracture during acute phase (weeks 1–2), subacute (weeks 3–6), post-acute (weeks 12–24), and chronic phase (from week 53)
Discussion
The results of this scoping review are based on 32 papers that included gait parameters as outcomes in intervention studies on older adults after hip fracture. This review is an update and extension of a previous scoping review originally including four patient groups [20].
Despite mobility recovery being the focus of rehabilitation after a hip fracture and walking in particular being a “gait keeper” function to most activities of daily living [16], our results indicate that most intervention studies conducted in hip fracture patients are not specifically designed to evaluate effects on gait parameters and physical mobility outcomes, with the current knowledge largely limited to a single parameter, namely gait speed. Gait speed is a robust measure of general health and function among older adults [54, 55], and commonly used as a measure of walking ability and functional mobility when evaluating interventions to improve mobility also after hip fracture [17]. However, while gait speed is a robust and useful measure, it is not a specific measure of walking ability. Using gait speed alone may not capture additional aspects of functional recovery after hip fracture [56].
Based on a recent expert consensus, physical mobility includes several domains that should be addressed, including gait volume, pace, cadence, asymmetry, gait phases, and gait variability [57]. This is also mirrored in a recent meta-ethnography of more than 120 qualitative studies summarizing patient perception of walking and mobility [58]. In this paper, patients largely agreed that aspects such as walking distance, perceived safety and balance concerns, and additional cognitive effort of walking are major features of walking capacity and affect walking activities, irrespective of their underlying conditions. Gait speed as such thus reflects an extremely narrow aspect of walking characteristics of older patients.
Despite the evidence for the importance of additional gait characteristics beyond gait speed, we found that gait speed by far was the most and often the only gait parameter reported in hip fracture trials. This might be because it is relatively easy to measure under supervised conditions. Furthermore, gait parameters were most often used as secondary outcomes in the RCTs in the hip fracture population rather than as primary outcome. A recently published Cochrane review evaluated effects of interventions to improve mobility after hip fracture and found moderate to high certainty for clinical meaningful increases of gait speed after mobility interventions in in-hospital and post-hospital settings [17]. Furthermore, another recent systematic review and meta-analysis on RCTs evaluating the effects of exercise interventions on physical function and mobility after hip fracture found that among fifteen included studies (from 12 different trials), gait speed was the primary outcome in only two of these trials, while a variety of strength, balance, and mobility tests were included as primary outcome in the other included trials [14]. In our current review, among 32 papers, we found only eight papers that included gait parameters from longer walks. Furthermore, only three intervention studies included instrumented physical mobility domains beyond gait speed, and only five made use of real-life DMOs. This indicates that despite DMOs being available, the transition from traditional clinical or in-lab to out-of-lab assessment has yet to be made. This transition is needed to assess effects of interventions on mobility recovery after hip fracture at higher granularity in all aspects of patients’ lives, so that optimal care pathways can be defined.
We found only two studies designed specifically to evaluate intervention effects on gait outcomes that reached sufficient numbers and showed treatment effects for the primary outcomes [9, 53]. One of these studies used daily number of steps and daily walking time as primary endpoints and found motivational interviewing to result in clinically meaningful improvements in these outcomes [53]. The other study found a significant effect of an exercise intervention on gait speed as primary endpoint, but no transfer effects on secondary real-life gait parameters such as daily upright time and the number of upright events [9]. The lack of transfer effects to real-world parameters observed in this study may have been caused by the nature of the exercise intervention that did not include specific training in real-world situations. This study underscores that traditional clinical or lab-based measures do not necessarily reflect gait performance in real-world in hip fracture patients, as well as the importance of including more domains of physical mobility than gait speed alone when assessing recovery of physical function after a hip fracture. Thus, the identification of a set of real-world walking parameters along with agreed definitions has important implications for the future of hip fracture intervention studies aiming to improve mobility [57]. The results in our review also highlight that we are still far from the necessary transition to include real-world unsupervised gait assessments in well-designed RCTs in the hip fracture population.
Limitations and future studies
There are some critical reflections regarding this review. Although it is a strength that we focused on studies in which gait parameters from instrumented measures were reported as endpoints, this constitutes a potential limitation as well. Although our results may not be generalizable to more general mobility parameters observed after a hip fracture or to patients with other adverse health conditions, our study allows an in-depth and updated analysis of gait parameters in hip fractures patients, including DMOs. Future RCTs aiming at assessing the effects of interventions on mobility recovery in hip fracture patients should include aspects of gait beyond gait speed alone as primary and secondary outcomes. Gait parameters measured by traditional clinical tests or in-lab and mobility measured in real-life settings should be included for the same patients to evaluate whether and how improvements in gait function may transfer to improvement of mobility in real-life settings and independence in daily life.
In summary, although existing evidence points to exercise as the main intervention to improve mobility recovery in older adults after hip fracture, our review shows that current evidence is rather unidimensional, with gait parameters used in clinical trials being largely limited to gait speed from short in-lab walks. Despite mobility being a key problem after hip fracture, few studies focus on it as a primary or even secondary outcome. Digital solutions for measuring mobility in real-world are still used only rarely, although recent developments in movement sensor algorithms allow easy detection of gait parameters from real-life settings. There is a need for larger and higher-quality RCTs, where gait parameters from real-world measures are used as primary endpoints, to advance knowledge on how to best regain mobility after a hip fracture and our ability to define optimal care pathways.
Data Availability
Data from the overarching scoping review are available on the following website: https://osf.io/k7395/.
References
Cooper C, Cole ZA, Holroyd CR, Earl SC, Harvey NC, Dennison EM et al (2011) Secular trends in the incidence of hip and other osteoporotic fractures. Osteoporos Int 22(5):1277–1288. https://doi.org/10.1007/s00198-011-1601-6
Cummings SR, Melton LJ (2002) Epidemiology and outcomes of osteoporotic fractures. Lancet 359(9319):1761–1767. https://doi.org/10.1016/S0140-6736(02)08657-9
Papadimitriou N, Tsilidis KK, Orfanos P, Benetou V, Ntzani EE, Soerjomataram I et al (2017) Burden of hip fracture using disability-adjusted life-years: a pooled analysis of prospective cohorts in the CHANCES consortium. Lancet Public Health 2(5):e239–ee46. https://doi.org/10.1016/s2468-2667(17)30046-4
Johnell O, Kanis JA (2004) An estimate of the worldwide prevalence, mortality and disability associated with hip fracture. Osteoporos Int 15(11):897–902. https://doi.org/10.1007/s00198-004-1627-0
Tajeu GS, Delzell E, Smith W, Arora T, Curtis JR, Saag KG et al (2014) Death, debility, and destitution following hip fracture. J Gerontol A Biol Sci Med Sci 69(3):346–353. https://doi.org/10.1093/gerona/glt105
Magaziner J, Chiles N, Orwig D (2015) Recovery after hip fracture: interventions and their timing to address deficits and desired outcomes--evidence from the Baltimore hip studies. Nestle Nutr Inst Workshop Ser 83:71–81. https://doi.org/10.1159/000382064
Prestmo A, Hagen G, Sletvold O, Helbostad JL, Thingstad P, Taraldsen K et al (2015) Comprehensive geriatric care for patients with hip fractures: a prospective, randomised, controlled trial. Lancet 385(9978):1623–1633. https://doi.org/10.1016/s0140-6736(14)62409-0
Handoll HH, Cameron ID, Mak JC, Panagoda CE, Finnegan TP (2021) Multidisciplinary rehabilitation for older people with hip fractures. Cochrane Database Syst Rev 11(11):CD007125. https://doi.org/10.1002/14651858.cd007125.pub3
Taraldsen K, Thingstad P, Dohl O, Follestad T, Helbostad JL, Lamb SE et al (2019) Short and long-term clinical effectiveness and cost-effectiveness of a late-phase community-based balance and gait exercise program following hip fracture. The EVA-Hip Randomised Controlled Trial. PLoS One 14(11):e0224971. https://doi.org/10.1371/journal.pone.0224971
Mangione KK, Craik RL, Kenny A, Memaj A, Miller MF, Chen M et al (2021) The effect of frailty on walking recovery after hip fracture: a secondary analysis of the community ambulation project. J Gerontol A Biol Sci Med Sci 76(11):e335–e3e9. https://doi.org/10.1093/gerona/glab044
Sheehan KJ, Smith TO, Martin FC, Johansen A, Drummond A, Beaupre L et al (2019) Conceptual framework for an episode of rehabilitative care after surgical repair of hip fracture. Phys Ther 99(3):276–285. https://doi.org/10.1093/ptj/pzy145
Gonzalez de Villaumbrosia C, Saez Lopez P, Martin de Diego I, Lancho Martin C, Cuesta Santa Teresa M, Alarcon T et al (2021) Predictive model of gait recovery at one month after hip fracture from a national cohort of 25,607 patients: the hip fracture prognosis (HF-Prognosis) tool. Int J Environ Res Public Health 18(7):3809. https://doi.org/10.3390/ijerph18073809
Auais MA, Eilayyan O, Mayo NE (2012) Extended exercise rehabilitation after hip fracture improves patients' physical function: a systematic review and meta-analysis. Phys Ther 92(11):1437–1451. https://doi.org/10.2522/ptj.20110274
Zhang X, Butts WJ, You T (2022) Exercise interventions, physical function, and mobility after hip fracture: a systematic review and meta-analysis. Disabil Rehabil 44(18):4986–4996. https://doi.org/10.1080/09638288.2021.1924299
Xu BY, Yan S, Low LL, Vasanwala FF, Low SG (2019) Predictors of poor functional outcomes and mortality in patients with hip fracture: a systematic review. BMC Musculoskelet Disord 20(1):568. https://doi.org/10.1186/s12891-019-2950-0
Haywood KL, Griffin XL, Achten J, Costa ML (2014) Developing a core outcome set for hip fracture trials. Bone Joint J 96-B(8):1016–1023. https://doi.org/10.1302/0301-620x.96b8.33766
Fairhall NJ, Dyer SM, Mak JC, Diong J, Kwok WS, Sherrington C (2022) Interventions for improving mobility after hip fracture surgery in adults. Cochrane Database Syst Rev 9(9):CD001704. https://doi.org/10.1002/14651858.cd001704.pub5
Rochester L, Mazza C, Mueller A, Caulfield B, McCarthy M, Becker C et al (2021) A roadmap to inform development, validation and approval of digital mobility outcomes: the Mobilise-D approach. Digit Biomark 4(Suppl 1):13–27. https://doi.org/10.1159/000512513
Polhemus AM, Bergquist R, Bosch de Basea M, Brittain G, Buttery SC, Chynkiamis N et al (2020) Walking-related digital mobility outcomes as clinical trial endpoint measures: protocol for a scoping review. BMJ Open 10:e038704. https://doi.org/10.1136/bmjopen-2020-038704
Polhemus A, Ortiz LD, Brittain G, Chynkiamis N, Salis F, Gassner H et al (2021) Walking on common ground: a cross-disciplinary scoping review on the clinical utility of digital mobility outcomes. NPJ Digit Med 4(1):149. https://doi.org/10.1038/s41746-021-00513-5
Polhemus AM. Mobilise-D scoping review OSF2021. https://osf.io/k7395
Higgins JP, Altman DG, Gotzsche PC, Juni P, Moher D, Oxman AD et al (2011) The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 343:d5928. https://doi.org/10.1136/bmj.d5928
Binder EF, Brown M, Sinacore DR, Steger-May K, Yarasheski KE, Schechtman KB (2004) Effects of extended outpatient rehabilitation after hip fracture: a randomized controlled trial. JAMA 292(7):837–846. https://doi.org/10.1001/jama.292.7.837
Mangione KK, Craik RL, Palombaro KM, Tomlinson SS, Hofmann MT (2010) Home-based leg-strengthening exercise improves function 1 year after hip fracture: a randomized controlled study. J Am Geriatr Soc 58(10):1911–1917. https://doi.org/10.1111/j.1532-5415.2010.03076.x
Mangione KK, Craik RL, Tomlinson SS, Palombaro KM (2005) Can elderly patients who have had a hip fracture perform moderate- to high-intensity exercise at home? Phys Ther 85(8):727–739
Mitchell SL (2001) Quadriceps function in elderly patients after proximal femoral fracture. Dissertation,. University of Glasgow
Moseley AM, Sherrington C, Lord SR, Barraclough E, St George RJ, Cameron ID (2009) Mobility training after hip fracture: a randomised controlled trial. Age Ageing 38(1):74–80. https://doi.org/10.1093/ageing/afn217
Mård M, Vaha J, Heinonen A, Portegijs E, Sakari-Rantala R, Kallinen M et al (2008) The effects of muscle strength and power training on mobility among older hip fracture patients. Adv Physiother 10(4):195–202. https://doi.org/10.1080/14038190801999570
Overgaard JA, Kallemose T, Mangione KK, Kristensen MT (2022) Six versus 12 weeks of outpatient physical therapy including progressive resistance training in cognitively intact older adults after hip fracture: a multicenter randomized controlled trial. J Gerontol A Biol Sci Med Sci 77(7):1455–1462. https://doi.org/10.1093/gerona/glab256
Portegijs E, Read S, Pakkala I, Kallinen M, Heinonen A, Rantanen T et al (2014) Sense of coherence: effect on adherence and response to resistance training in older people with hip fracture history. J Aging Phys Act 22(1):138–145. https://doi.org/10.1123/japa.2012-0229
Portegijs E, Kallinen M, Rantanen T, Heinonen A, Sihvonen S, Alen M et al (2008) Effects of resistance training on lower-extremity impairments in older people with hip fracture. Arch Phys Med Rehabil 89 (9):1667–1674. https://doi.org/10.1016/j.apmr.2008.01.026
Said CM, Delahunt M, Hardidge A, Smith P, Tran P, McDonald L et al (2021) Recumbent cycling to improve outcomes in people with hip fracture: a feasibility randomized trial. BMC Geriatr 21(1):394. https://doi.org/10.1186/s12877-021-02321-8
Senserrick C, Lawler K, Scroggie GD, Williams K, Taylor NF (2021) Three short sessions of physiotherapy during rehabilitation after hip fracture were no more effective in improving mobility than a single longer session: a randomised controlled trial. Physiotherapy 112:87–95. https://doi.org/10.1016/j.physio.2020.12.002
Sherrington C, Lord SR, Herbert RD (2004) A randomized controlled trial of weight-bearing versus non-weight-bearing exercise for improving physical ability after usual care for hip fracture. Arch Phys Med Rehabil 85(5):710–716. https://doi.org/10.1016/s0003-9993(03)00620-8
Sherrington C, Lord SR (2003) Herbert RD (2003) A randomised trial of weight-bearing versus non-weight-bearing exercise for improving physical ability in inpatients after hip fracture. Aust J Physiother 49(1):15–22. https://doi.org/10.1016/s0004-9514(14)60184-7
Sylliaas H, Brovold T, Wyller TB, Bergland A (2011) Progressive strength training in older patients after hip fracture: a randomised controlled trial. Age Ageing 40(2):221–227. https://doi.org/10.1093/ageing/afq167
Sylliaas H, Brovold T, Wyller TB, Bergland A (2012) Prolonged strength training in older patients after hip fracture: a randomised controlled trial. Age Ageing 41(2):206–212. https://doi.org/10.1093/ageing/afr164
van Ooijen MW, Roerdink M, Trekop M, Janssen TW, Beek PJ (2016) The efficacy of treadmill training with and without projected visual context for improving walking ability and reducing fall incidence and fear of falling in older adults with fall-related hip fracture: a randomized controlled trial. BMC Geriatr 16(1):215. https://doi.org/10.1186/s12877-016-0388-x
Han CY, Crotty M, Thomas S, Cameron ID, Whitehead C, Kurrle S et al (2021) Effect of individual nutrition therapy and exercise regime on gait speed, physical function, strength and balance, body composition, energy and protein, in injured, vulnerable elderly: a multisite randomized controlled trial (INTERACTIVE). Nutrients 13(9):3182. https://doi.org/10.3390/nu13093182
Tsauo JY, Leu WS, Chen YT, Yang RS (2005) Effects on function and quality of life of postoperative home-based physical therapy for patients with hip fracture. Arch Phys Med Rehabil 86(10):1953–1957. https://doi.org/10.1016/j.apmr.2005.04.020
Adunsky A, Chandler J, Heyden N, Lutkiewicz J, Scott BB, Berd Y et al (2011) MK-0677 (ibutamoren mesylate) for the treatment of patients recovering from hip fracture: a multicenter, randomized, placebo-controlled phase IIb study. Arch Gerontol Geriatr 53(2):183–189. https://doi.org/10.1016/j.archger.2010.10.004
Hedstrom M, Sjoberg K, Brosjo E, Astrom K, Sjoberg H, Dalen N (2002) Positive effects of anabolic steroids, vitamin D and calcium on muscle mass, bone mineral density and clinical function after a hip fracture. A randomised study of 63 women. J Bone Joint Surg Br 84(4):497–503. https://doi.org/10.1302/0301-620x.84b4.12434
Hofbauer LC, Witvrouw R, Varga Z, Shiota N, Cremer M, Tanko LB et al (2021) Bimagrumab to improve recovery after hip fracture in older adults: a multicentre, double-blind, randomised, parallel-group, placebo-controlled, phase 2a/b trial. Lancet Healthy Longev 2(5):e263–e274. https://doi.org/10.1016/s2666-7568(21)00084-2
Baek J, Park N, Lee B, Jee S, Yang S, Kang S (2018) Effects of repetitive peripheral magnetic stimulation over vastus lateralis in patients after hip replacement surgery. Ann Rehabil Med (1):42, 67–75. https://doi.org/10.5535/arm.2018.42.1.67
Lamb SE, Oldham JA, Morse RE, Evans JG (2002) Neuromuscular stimulation of the quadriceps muscle after hip fracture: a randomized controlled trial. Arch Phys Med Rehabil 83(8):1087–1092. https://doi.org/10.1053/apmr.2002.33645
Li H, Wang Q, Dai GG, Peng H (2018) PFNA vs. DHS helical blade for elderly patients with osteoporotic femoral intertrochanteric fractures. Eur Rev Med Pharmacol Sci 22(1 Suppl):1–7. https://doi.org/10.26355/eurrev_201807_15346
Shi H, Xiao L, Wang Z (2018) Curative effect of artificial femoral head replacement and its effect on hip joint function and complications of senile patients with femoral intertrochanteric fracture. Exp Ther Med 16(2):623–628. https://doi.org/10.3892/etm.2018.6214
Chammout GK, Mukka SS, Carlsson T, Neander GF, Stark AW, Skoldenberg OG (2012) Total hip replacement versus open reduction and internal fixation of displaced femoral neck fractures: a randomized long-term follow-up study. J Bone Joint Surg Am 94(21):1921–1928. https://doi.org/10.2106/jbjs.k.01615
Taraldsen K, Sletvold O, Thingstad P, Saltvedt I, Granat MH, Lydersen S et al (2014) Physical behavior and function early after hip fracture surgery in patients receiving comprehensive geriatric care or orthopedic care--a randomized controlled trial. J Gerontol A Biol Sci Med Sci 69(3):338–345. https://doi.org/10.1093/gerona/glt097
Taraldsen K, Thingstad P, Sletvold O, Saltvedt I, Lydersen S, Granat MH et al (2015) The long-term effect of being treated in a geriatric ward compared to an orthopaedic ward on six measures of free-living physical behavior 4 and 12 months after a hip fracture - a randomised controlled trial. BMC Geriatr 15:160. https://doi.org/10.1186/s12877-015-0153-6
Thingstad P, Taraldsen K, Saltvedt I, Sletvold O, Vereijken B, Lamb SE et al (2016) The long-term effect of comprehensive geriatric care on gait after hip fracture: the Trondheim Hip Fracture Trial--a randomised controlled trial. Osteoporos Int 27(3):933–942. https://doi.org/10.1007/s00198-015-3313-9
Langford DP, Fleig L, Brown KC, Cho NJ, Frost M, Ledoyen M et al (2015) Back to the future - feasibility of recruitment and retention to patient education and telephone follow-up after hip fracture: a pilot randomized controlled trial. Patient Prefer Adherence 9:1343–1351. https://doi.org/10.2147/ppa.s86922
O'Halloran PD, Shields N, Blackstock F, Wintle E, Taylor NF (2016) Motivational interviewing increases physical activity and self-efficacy in people living in the community after hip fracture: a randomized controlled trial. Clin Rehabil 30(11):1108–1119. https://doi.org/10.1177/0269215515617814
Abellan van Kan G, Rolland Y, Andrieu S, Bauer J, Beauchet O, Bonnefoy M et al (2009) Gait speed at usual pace as a predictor of adverse outcomes in community-dwelling older people an International Academy on Nutrition and Aging (IANA) Task Force. J Nutr Health Aging 13(10):881–889. https://doi.org/10.1007/s12603-009-0246-z
Studenski S, Perera S, Patel K, Rosano C, Faulkner K, Inzitari M et al (2011) Gait speed and survival in older adults. JAMA 305(1):50–58. https://doi.org/10.1001/jama.2010.1923
Izquierdo M, Duque G, Morley JE (2021) Physical activity guidelines for older people: knowledge gaps and future directions. Lancet Healthy Longev 2(6):e380–e3e3
Kluge F, Del Din S, Cereatti A, Gassner H, Hansen C, Helbostad JL et al (2021) Consensus based framework for digital mobility monitoring. PLoS One 16(8):e0256541. https://doi.org/10.1371/journal.pone.0256541
Delgado-Ortiz L, Polhemus A, Keogh A, Sutton N, Remmele W, Hansen C et al (2023) Listening to the patients’ voice: a conceptual framework of the walking experience. Age Ageing 52(1):afac233. https://doi.org/10.1093/ageing/afac233
Acknowledgements
The authors gratefully acknowledge the contribution from the abstract screeners in the original scoping review. Part of this work was supported by the Mobilise-D project that has received funding from the Innovative Medicines Initiative 2 Joint Undertaking (JU) under grant agreement No. 820820. This JU receives support from the European Union’s Horizon 2020 research and innovation program and the European Federation of Pharmaceutical Industries and Associations (EFPIA). Content in this publication reflects the authors’ view and neither IMI nor the European Union, EFPIA, or any Associated Partners are responsible for any use that may be made of the information contained herein.
Funding
Open access funding provided by OsloMet - Oslo Metropolitan University Part of this work was supported by the Mobilise-D project that has received funding from the Innovative Medicines Initiative 2 Joint Undertaking (JU) under grant agreement no. 820820. This JU receives support from the European Union's Horizon 2020 research and innovation program and the European Federation of Pharmaceutical Industries and Associations (EFPIA). Content in this publication reflects the authors’ view and neither IMI nor the European Union, EFPIA, or any Associated Partners are responsible for any use that may be made of the information contained herein.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical approval
For this type of study, formal consent is not required.
Competing interests
None.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
ESM 1
(PDF 218 kb)
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Taraldsen, K., Polhemus, A., Engdal, M. et al. Evaluation of mobility recovery after hip fracture: a scoping review of randomized controlled studies. Osteoporos Int 35, 203–215 (2024). https://doi.org/10.1007/s00198-023-06922-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-023-06922-4