
Abstract
Electronic cigarette or vaping product use–associated lung injury (EVALI) is a toxic inhalational injury that surged in late 2019 and early 2020, immediately prior to the coronavirus disease 2019 (COVID-19) pandemic. Although EVALI cases have significantly decreased, they are still encountered, especially among adolescents. While several characteristic imaging findings and patterns of EVALI have been described, some of them can overlap with the imaging features of COVID-19 pneumonia. We provide a comprehensive review of EVALI that includes the latest updates and highlight the important role of radiologists as contributors to the appropriate and timely care of pediatric patients with this diagnosis.
Similar content being viewed by others


Introduction
Electronic cigarettes, or e-cigarettes, also known as vapes or vape pens (among other monikers), were first introduced in the United States in 2007 and were originally marketed as a safer alternative to cigarettes [1]. E-cigarettes are devices that aerosolize substances for inhalation [2]. The basic construct of an e-cigarette consists of three components: a battery, a reservoir (cartridge) for the substance to be vaped, and a heating element to vaporize the substance. Numerous vaping products exist, including flavoring additives, nicotine compounds, tetrahydrocannabinol (THC) oils and waxes [2]. The use of vaping products has risen precipitously since their introduction, particularly among adolescents [3]. Based on data from the National Youth Tobacco Survey (NYTS), the number of high-school and middle-school students who reported e-cigarette usage in 2011 was 1.5% and 0.6%, respectively, and by 2018 this had risen to 20.8% (3.1 million students) and 4.9% (570,000 students), respectively [3]. In fact, the reported use of e-cigarettes among high-school and middle-school students in 2018 reflected an increase of 78% and 48%, respectively, compared to the previous year and prompted the U.S. surgeon general to declare the use of e-cigarettes an epidemic among the youth [4]. More recent NYTS data from 2021 reported e-cigarette use in only 11.3% (1.7 million) and 2.8% (320,000) of high-school and middle-school students, respectively, though it was stated that these data cannot be compared to previous yearly results given the changes in how the survey had to be administered during the coronavirus disease 2019 (COVID-19) pandemic [5, 6].
Cases linking e-cigarette use to lung injury were initially reported in 2012 [7]. A dramatic increase in cases of e-cigarette or vaping product use–associated lung injury (EVALI) occurred between March 2019 and February 2020, peaking in September 2019 [8]. During this surge, the U.S. Centers for Disease Control and Prevention (CDC) recorded a total of 2,807 patient hospitalizations and 68 deaths [8]. The majority of the reported EVALI cases involved patients younger than 25 years, and approximately 15% of all hospitalizations were in children younger than 18; most of them were male [8]. The number of reported cases of EVALI has declined since early 2020 and the CDC stopped tracking cases in February 2020, just prior to the COVID-19 pandemic [8].
The preponderance of cases of EVALI, which is a toxic inhalational injury, has been among patients who report a history of vaping THC-containing products exclusively or THC- and nicotine-containing products combined [8]. A minority of cases has been among patients who reported using nicotine-containing vaping products only [8]. Numerous e-cigarette brands are available with variable compositions of THC- and nicotine-containing products. While vaping-product sources are wide-ranging, pediatric patients often report obtaining cartridges from friends, relatives or dealers (local or online) [2, 9]. Among the various additives to vaping products, vitamin E acetate has been strongly linked to cases of EVALI [8]. Vitamin E acetate has been utilized as a diluting agent for THC oils sold by informal sources to increase profits [8, 10]. Once heated by vape pens, vitamin E acetate can decompose to ketene gas, which has been shown to cause acute lung injury in animal testing [10]. Vitamin E acetate has been detected in bronchoalveolar lavage (BAL) specimens of patients with EVALI, including a series that demonstrated its presence in 94% of patients compared to none in the control group of healthy volunteers [11]. Given the heterogeneity of available vaping products, other additives might also play a role in the variable presentations and imaging patterns of EVALI [2, 8, 10].
Clinical findings
The clinical presentation of children with EVALI is variable and symptoms can overlap with other entities, including infectious processes (such as COVID-19), other environmental/chemical exposures and autoimmune diseases [2]. Respiratory and constitutional symptoms include cough, shortness of breath, dyspnea on exertion and chest pain, as well as fever, fatigue, chills and weight loss [2, 9, 10, 12,13,14,15]. Nausea, vomiting, abdominal pain and diarrhea are also very common and have been reported as the initial isolated symptomology in several cases [2, 9, 10, 12,13,14,15]. Physical exam findings can include tachypnea and hypoxia [13]. Laboratory findings are nonspecific, and can include elevated inflammatory markers such as erythrocyte sedimentation rate (ESR), C-reactive protein (CRP) and lactate dehydrogenase (LDH), along with elevated white blood cell count and transaminases [10, 13].
Though EVALI is a diagnosis of exclusion, the CDC diagnostic criteria include both clinical and radiologic elements: e-cigarette use or “dabbing” (superheated inhalation of aerosolized substances with high THC concentration) during the 90 days before symptom onset, pulmonary opacities on chest radiographs or ground-glass opacities on CT, and absence of pulmonary infection or other plausible alternative diagnoses [8]. If pulmonary infection is present, a diagnosis of probable EVALI can be still assigned if the clinical team believes it is not the sole cause of the lung injury [8].
Imaging findings
Given the frequent respiratory symptoms, chest radiography is typically the first imaging study obtained. The most common finding on radiographs is bilateral opacities, typically ground-glass, with or without consolidation [2, 12,13,14]. These opacities are usually symmetrical, often with lower lobe predominance [2, 12,13,14]. However, chest radiographs can be normal in a minority of patients at the time of presentation, which makes radiographs less sensitive for the assessment of EVALI [15].
Non-contrast CT of the chest is a much better modality to further characterize and show the extent of pulmonary findings seen on chest radiography or when no radiographic abnormality is detected in the setting of known vaping exposure [2, 12, 15]. Chest CT angiogram might be considered if pulmonary embolism is on the clinical differential diagnosis [2]. Children who present with gastrointestinal complaints exclusively might be initially evaluated with abdominopelvic CT, which by virtue of the field-of-view typically includes portions of the lower lungs [12, 15]. Several imaging series have indicated that detection of abnormalities in the lung bases on abdomen/pelvis CT triggered the initial consideration of EVALI in those patients [12].
Chest CT findings of EVALI include ground-glass opacities that are usually bilateral and diffuse, with lower lobe predominance, with or without associated consolidation (Figs. 1, 2, 3 and 4) [2, 12, 14, 16,17,18]. A large case series of 160 adolescents and adults found a positive correlation between the degree of consolidation and severity of lung injury in patients with higher frequency of vaping [17]. Subpleural and lobular sparing are frequently observed, findings that are commonly identified among cases of acute and subacute lung injury [2, 9, 10, 12,13,14,15,16,17]. Although peribronchovascular sparing has also been described with EVALI, it has not been reported in patients with other causes of acute and subacute lung injury [2, 15, 17]. The subpleural and peribronchovascular sparing is attributed anatomically to the locations of the peripheral and axial interstitia, respectively [15], as well as the physiological lymphatic clearance (Figs. 2 and 3) [17]. The lobular sparing has been attributed to the zonal distribution of lung injury [2]. Mixed patterns of parenchymal and airway-centric disease also occur [17]. In addition, a reverse-halo (atoll) sign (central ground-glass opacity surrounded by dense consolidation of a crescentic shape or a complete ring) [12, 14, 18], diffuse ill-defined or ground-glass centrilobular nodules with apical predominance [2, 12, 13, 17], interlobular septal thickening [2, 12, 15, 17, 18] and a crazy-paving pattern [2, 15, 17] have all been reported. Mediastinal and hilar lymphadenopathy has also been frequently observed [2, 13, 15,16,17]. Pleural effusions occur in a minority of cases [2, 12,13,14,15,16,17], and the effusions are typically small [17].

15-year-old boy with e-cigarette or vaping product use–associated lung injury (EVALI). He presented with cough along with fever and reported vaping tetrahydrocannabinol (THC) since 7th–8th grade and obtaining cartridges from informal sources. a Posteroanterior chest radiograph shows ground-glass opacities of bibasilar predominance, with a subtle component of consolidation. b Axial chest CT in lung window performed 1 day after chest radiograph demonstrates scattered bibasilar ground-glass opacities and consolidative opacities in both lower lobes (white arrows) with lobular sparing (black arrows) and volume loss (i.e. alveolar collapse) evident by the posterior displacement of both major fissures. The overall pattern is compatible with diffuse alveolar damage

16-year-old girl with e-cigarette or vaping product use–associated lung injury (EVALI). She presented with fevers, cough, shortness of breath, vomiting and weight loss and reported tetrahydrocannabinol (THC) dabbing for 3 months prior to presentation. a Posteroanterior chest radiograph shows ground-glass opacities of bibasilar predominance. b Axial chest CT in lung window performed the same day demonstrates bibasilar ground-glass opacities involving all pulmonary lobes along with subpleural sparing (white arrows) and an atoll sign (black arrow). The overall pattern is consistent with organizing pneumonia

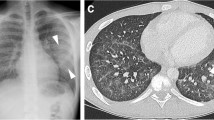
16-year-old boy with e-cigarette or vaping product use–associated lung injury (EVALI). He presented with nausea, vomiting, chest pain, fever, night sweats and diarrhea and reported vaping tetrahydrocannabinol (THC) and nicotine for more than 1 year. a Posteroanterior chest radiograph demonstrates diffuse subtle ground-glass opacities bilaterally. b Axial chest CT in lung window performed 1 day later shows diffuse ground-glass opacities involving all pulmonary lobes along with subpleural (white arrows) and peribronchovascular sparing (black arrows). The overall appearance is most compatible with a hypersensitivity pneumonitis-like pattern

14-year-old girl with e-cigarette or vaping product use–associated lung injury (EVALI). She presented with nausea, vomiting, shortness of breath, fever and cough and reported vaping tetrahydrocannabinol (THC) for about 6 months. a Axial chest CT in mediastinum window shows pleural effusions bilaterally (arrows). b Axial chest CT in lung window shows extensive interlobular septal thickening (arrows), scattered ground-glass opacities and diffuse centrilobular nodules involving all pulmonary lobes. The overall appearance is most consistent with acute eosinophilic pneumonia-like pattern
Computed tomography imaging findings of EVALI reflect varying degrees and stages of acute lung injury, with patterns of organizing pneumonia (typically), diffuse alveolar damage, hypersensitivity pneumonitis-like pattern and acute eosinophilic pneumonia, among others, being encountered (Figs. 1, 2, 3 and 4) [12, 14, 17]. While several patterns demonstrate symmetrical and diffuse, often basilar-predominant ground-glass opacities or consolidation, some salient findings are more typical in one pattern compared to the others [17]. For instance, lobular sparing with evidence of alveolar collapse are common in diffuse alveolar damage; pronounced interlobular septal thickening along with bilateral small-to-moderate pleural effusions with or without centrilobular ground-glass nodules are characteristic of acute eosinophilic pneumonia; and sparing (subpleural or lobular), with or without atoll sign, sometimes with centrilobular ground-glass nodules, are common in organizing pneumonia [12, 17].
Pathology findings
The pathology findings of EVALI, ascertained via BAL and biopsies predominantly compiled from adults, reflect a spectrum of acute lung injury [19, 20]. BAL specimens most often show inflammatory findings, frequently with macrophages [10]. Based on some initial reported cases of EVALI with BAL specimens demonstrating lipid-laden macrophages, some investigators hypothesized that EVALI was caused by a form of exogenous lipoid pneumonia secondary to inhalation or aspiration of oils within vaping products [10, 17, 21, 22]. However, further histopathological reviews of the lipid-laden macrophages were more consistent with accumulation of endogenous lipids secondary to epithelial injury, referred to as endogenous lipoid pneumonia, a process that has been described in other forms of acute lung injury and infections [10, 23,24,25,26]. To date, no cases of exogenous lipoid pneumonia have been confirmed on pathology [2, 10]. Biopsy specimens also show findings along the spectrum of acute lung injury including acute fibrinous and organizing pneumonia, organizing pneumonia and diffuse alveolar damage [10]. Although in some patients with EVALI the imaging distribution of lung injury resembles and mimics a hypersensitivity pneumonitis-like pattern, no cases of hypersensitivity pneumonitis have been confirmed on histopathology (Fig. 3) [10, 17]. The spectrum of features among biopsies is related to the duration and magnitude of the lungs’ exposure to the noxious inhaled agents over time [10, 17]. Overall, the observed pathology findings are not specific to EVALI, and patterns certainly overlap with those of other inhalational exposures, infections and systemic diseases [10, 17].
Treatment and clinical course
Most patients diagnosed with EVALI are treated with respiratory therapy and oral or intravenous glucocorticoid therapy [9]. Respiratory support varies based on the severity of lung injury, with supplemental oxygen via nasal cannula being the most frequent measure [9]. More invasive therapy, including bilevel positive airway pressure (BiPAP), intubation with mechanical ventilation and extracorporeal membrane oxygenation (ECMO) might be required in those with severe lung injury [9]. Most patients improve with treatment and cessation of vaping [2, 9, 14, 15]. Abnormalities observed on imaging usually resolve within a few months [15]. In addition, spirometry in EVALI patients, which sometimes shows decreased forced expiratory volume in the first second (FEV1) and mild-to-moderate decrease in diffusion capacity, shows variable improvement at follow-up [14]. Although follow-up CT could have a role in assessing adolescents with EVALI, as has been suggested for the adult population [16], it is not part of the routine follow-up evaluation of pediatric patients; however, its performance could be pursued on a case-by-case basis.
The radiologist’s role
While cases of EVALI started to drop precipitously immediately prior to the COVID-19 pandemic — as a result of improved health care provider education, increased public awareness, identification of vitamin E acetate as the likely inciting agent, removal of vitamin E acetate from vaping products, and the role of law enforcement [17] — this diagnosis can still be encountered, especially among the adolescent population. Because imaging studies are often performed based on initial pulmonary or gastrointestinal complaints, the radiologist reviewing these studies might be the first to suggest a possible diagnosis of EVALI, particularly if these patients were previously healthy [9, 12]. Therefore, it is important for radiologists to be cognizant of the spectrum of imaging characteristics and patterns found with EVALI.
The overall heterogeneity of the imaging findings encountered among adolescents with EVALI is thought to be the result of a multitude of variables that can contribute to lung injury such as the substances vaped, which vary in composition; the concentrations of their components; as well as the device utilized, which can affect particle size or byproducts of combustion dependent on the heating element of the device itself [2]. Other factors such as frequency and duration of vaping, along with the amount of aerosol inhaled and user susceptibilities, can also contribute to the heterogeneous appearance of the imaging findings in EVALI [2].
Because EVALI cases have continued to present during the COVID-19 pandemic, it is important to note that the imaging features of both entities can overlap [17, 19] (Table 1). Briefly, typical radiographic findings of COVID-19 pneumonia include patchy bilateral ground-glass opacities (sometimes rounded), with or without consolidation, with a central or peripheral distribution and of lower-lobe predominance — though diffuse distributions are occasionally encountered (Fig. 5) [19, 27] — which might be indistinguishable from the radiographic appearance of EVALI with bilateral symmetrical ground-glass and consolidative opacities, also of basilar predominance [12]. On chest radiography, COVID-19 pneumonia in young children might also manifest with bronchial wall thickening and a peribronchial distribution of opacities [27, 28], though this nonspecific finding has been described with other viral infections as a reflection of lower airways inflammation.

16-year-old obese boy who presented with diarrhea, cough and shortness of breath. He was exposed to COVID-19 at school and had a positive reverse transcription polymerase chain reaction (RT-PCR) test 2 days before imaging. a Posteroanterior chest radiograph performed 2 days before chest CT demonstrates rounded opacities of basilar and peripheral predominance bilaterally. b Axial chest CT in lung window shows rounded consolidative opacities involving all pulmonary lobes, predominantly with peripheral distribution, and halo signs in the lower lobes (arrows). The overall findings are typical of COVID-19 pneumonia
Many similarities between the imaging appearance of COVID-19 pneumonia and EVALI exist on CT as well. However, some features might help in distinguishing the two entities. While both manifest with bilateral ground-glass opacities, with or without consolidation, the presence of subpleural, peribronchovascular and lobular sparing frequently seen in EVALI [12, 13, 15, 17] is a feature not commonly reported with COVID-19 pneumonia [17, 19]. An airway-centric pattern of lung injury with centrilobular nodules, typically with an upper lung predominance, has been described in EVALI but not in COVID-19 pneumonia [17]. The atoll sign has been mainly reported in EVALI (Fig. 2) [12, 14], while the halo sign (a region of consolidation with surrounding ground-glass) has been mostly reported in COVID-19 pneumonia (Fig. 5) [19]. Lymphadenopathy might be present in EVALI patients [13, 17] but is less common in pediatric patients with COVID-19 pneumonia [17, 19, 28]. Last, pleural effusions are sometimes found in EVALI patients but are uncommon in COVID-19 pneumonia [17, 19]. In summary, if subpleural, lobular or peribronchovascular sparing; upper-lobe-predominant centrilobular ground-glass nodules; or an atoll sign are encountered on CT, the diagnosis of EVALI could be favored over COVID-19 pneumonia or at least brought up in the differential diagnosis to prompt further investigation regarding the specific use of e-cigarettes/vapes. Ultimately, the diagnosis of COVID-19 pneumonia is primarily made based on a positive RT-PCR or a positive serology [27, 28].
Although multisystem inflammatory syndrome in children (MIS-C) is a result of excessive immune response following COVID-19 infection and typically affects multiple organ systems, its imaging findings can overlap with some EVALI and COVID-19 pulmonary manifestations [29,30,31]. The most reported thoracic imaging features in MIS-C include cardiomegaly caused by cardiac dysfunction, along with ground-glass opacities and bilateral pleural effusions attributable to pulmonary edema, volume overload and third-spacing of fluid (Fig. 6). Compared to COVID-19 pneumonia and EVALI, pleural effusions are far more frequently observed in children with MIS-C [30]. In addition, perihilar and peribronchial thickening, presumably from airways inflammation, are common chest radiographic findings among children with MIS-C [29] and are also frequently reported with COVID-19 infection [27] but not with EVALI.

15-year-old girl recently diagnosed with colitis. She presented with fluid refractory shock and tested positive for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) immunoglobulin G (IgG) antibodies. a Axial chest CT in mediastinum window shows bilateral pleural effusions (arrows) and mild enlargement of the right and left ventricles, qualitatively. Pericardial effusion was also present (not shown). b Axial chest CT in lung window shows predominantly central ground-glass opacities involving all pulmonary lobes (arrows), in keeping with pulmonary edema/volume overload. The overall findings are typical of MIS-C associated with COVID-19
Conclusion
Despite the significant decrease in EVALI cases since early 2020, much work remains as our understanding of this new diagnosis of exclusion and its inciting elements continues to expand. Although characteristic imaging features and patterns of EVALI have been described, their appearance can overlap with those of lung injury from infectious etiologies, particularly COVID-19 pneumonia, and other inhalational toxicants. Radiologists play an important role by recognizing the imaging findings that can be encountered with EVALI and can ultimately help expedite appropriate and effective care in pediatric patients with this diagnosis.
References
Cooke A, Fergeson J, Bulkhi A, Casale TB (2015) The electronic cigarette: the good, the bad, and the ugly. J Allergy Clin Immunol Pract 3:498–505
Kligerman S, Raptis C, Larsen B et al (2020) Radiologic, pathologic, clinical, and physiologic findings of electronic cigarette or vaping product use–associated lung injury (EVALI): evolving knowledge and remaining questions. Radiology 294:491–505
Cullen KA, Ambrose BK, Gentzke AS et al (2018) Notes from the field: use of electronic cigarettes and any tobacco product among middle and high school students — United States, 2011–2018. MMWR Morb Mortal Wkly Rep 67:1276–1277
Wang TW, Gentzke AS, Neff LJ et al (2021) Characteristics of e-cigarette use behaviors among U.S. youth, 2020. JAMA Netw Open 4:e2111336
Park-Lee E, Ren C, Sawdey MD et al (2021) Notes from the field: e-cigarette use among middle and high school students — National Youth Tobacco Survey, United States, 2021. MMWR Morb Mortal Wkly Rep 70:1387–1389
Center for Tobacco Products (2022) Results from the annual National Youth Tobacco Survey (NYTS). U.S. Food and Drug Administration website. https://www.fda.gov/tobacco-products/youth-and-tobacco/results-annual-national-youth-tobacco-survey. Accessed 24 Jan 2022
McCauley L, Markin C, Hosmer D (2012) An unexpected consequence of electronic cigarette use. Chest 141:1110–1113
U.S. Centers for Disease Control and Prevention (2021) Smoking & tobacco use: electronic cigarettes. CDC website. https://www.cdc.gov/tobacco/basic_information/e-cigarettes/index.htm. Accessed 15 Jun 2022
Rao DR, Maple KL, Dettori A et al (2020) Clinical features of e-cigarette, or vaping, product use–associated lung injury in teenagers. Pediatrics 146:e20194104
Smith ML, Gotway MB, Crotty Alexander LE, Hariri LP (2021) Vaping-related lung injury. Virchows Arch 478:81–88
Blount BC, Karwowski MP, Shields PG et al (2020) Vitamin E acetate in bronchoalveolar-lavage fluid associated with EVALI. N Engl J Med 382:697–705
Artunduaga M, Rao D, Friedman J et al (2020) Pediatric chest radiographic and CT findings of electronic cigarette or vaping product use–associated lung injury (EVALI). Radiology 295:430–438
Thakrar PD, Boyd KP, Swanson CP et al (2020) E-cigarette, or vaping, product use–associated lung injury in adolescents: a review of imaging features. Pediatr Radiol 50:338–344
Chidambaram AG, Dennis RA, Biko DM et al (2020) Clinical and radiological characteristics of e-cigarette or vaping product use associated lung injury. Emerg Radiol 27:495–501
Wang KY, Jadhav SP, Yenduri NJS et al (2020) E-cigarette or vaping product use–associated lung injury in the pediatric population: imaging features at presentation and short-term follow-up. Pediatr Radiol 50:1231–1239
Aberegg SK, Cirulis MM, Maddock SD et al (2020) Clinical, bronchoscopic and imaging findings of e-cigarette or vaping product use–associated lung injury among patients treated at an academic medical center. JAMA Newt Open 3:e2019176
Kligerman SJ, Kay FU, Raptis CA et al (2021) CT findings and patterns of e-cigarette or vaping product use–associated lung injury: a multicenter cohort of 160 cases. Chest 160:1492–1511
Panse PM, Feller FF, Butt YM et al (2020) Radiologic and pathologic correlation in EVALI. AJR Am J Roentgenol 215:1057–1064
Foust AM, Winant AJ, Chu WC et al (2020) Pediatric SARS, H1N1, MERS, EVALI, and now coronavirus disease (COVID-19) pneumonia: what radiologists need to know. AJR Am J Roentgenol 215:736–744
Butt YM, Smith ML, Tazelaar HD et al (2019) Pathology of vaping-associated lung injury. N Engl J Med 381:1780–1781
Mukhopadhyay S, Mehrad M, Dammert P et al (2020) Lung biopsy findings in severe pulmonary illness associated with e-cigarette use (vaping). Am J Clin Pathol 153:30–39
Davidson K, Brancato A, Heetderks P et al (2019) Outbreak of electronic-cigarette-associated acute lipoid pneumonia — North Carolina, July–August 2019. MMWR Morb Mortal Wkly Rep 68:784–786
Maddock SD, Cirulis MM, Callahan SJ et al (2019) Pulmonary lipid-laden macrophages and vaping. N Engl J Med 381:1488–1489
Basset-Léobon C, Lacoste-Collin L, Aziza J et al (2010) Cut-off values and significance of oil red O-positive cells in bronchoalveolar lavage fluid. Cytopathology 21:245–250
Corwin RW, Irwin RS (1985) The lipid-laden alveolar macrophage as a marker of aspiration in parenchymal lung disease. Am Rev Respir Dis 132:576–581
Pambuccian SE (2020) Testing for lipid-laden macrophages in bronchoalveolar lavage fluid to diagnose vaping-associated pulmonary injury. Are we there yet? J Am Soc Cytopathol 9:1–8
Caro-Dominguez P, Shelmerdine SC, Toso S et al (2020) Thoracic imaging of coronavirus disease 2019 (COVID-19) in children: a series of 91 cases. Pediatr Radiol 50:1354–1368
Pina Prata R, Forjaco A, Ruano CA et al (2021) COVID-19 in a pediatric cohort — retrospective review of chest computer tomography findings. Egypt J Radiol Nucl Med 52:83
Palabiyik F, Akcay N, Sevketoglu E et al (2021) Imaging of multisystem inflammatory disease in children (MIS-C) associated with COVID-19. Acad Radiol 28:1200–1208
Rostad BS, Shah JH, Rostad CA et al (2021) Chest radiograph features of multisystem inflammatory syndrome in children (MIS-C) compared to pediatric COVID-19. Pediatr Radiol 51:231–238
Blumfield E, Levin TL, Kurian J et al (2021) Imaging findings in multisystem inflammatory syndrome in children (MIS-C) associated with coronavirus disease (COVID-19). AJR Am J Roentgenol 216:507–517
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
None
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Friedman, J., Schooler, G.R., Kwon, J.K. et al. Pediatric electronic cigarette or vaping product use–associated lung injury (EVALI): updates in the coronavirus disease 2019 (COVID-19) pandemic era. Pediatr Radiol 52, 2009–2016 (2022). https://doi.org/10.1007/s00247-022-05454-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00247-022-05454-z