
Abstract
Purpose
To evaluate the sensitivity and specificity of PET/CT findings in PMR and generate a diagnostic algorithm utilizing a minimum number of musculoskeletal sites.
Methods
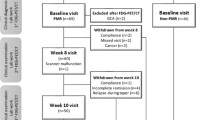
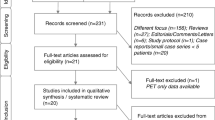
Steroid-naïve patients with newly diagnosed PMR (2012 EULAR/ACR classification criteria) were prospectively recruited to undergo whole-body 18F−FDG PET/CT. Each PMR case was age- and sex-matched to four PET/CT controls. Control scan indication, diagnosis and medical history were extracted from the clinical record. Qualitative and semi-quantitative scoring (maximum standardized uptake value [SUVmax]) of abnormal 18F-FDG uptake at 21 musculoskeletal sites was undertaken for cases and controls. Results informed the development of a novel PET/CT diagnostic algorithm using a classification and regression trees (CART) method.
Results
Thirty-three cases met the inclusion criteria and were matched to 132 controls. Mean age was 68.6 ± 7.4 years for cases compared with 68.2 ± 7.3 for controls, and 54.5% were male. Median CRP was 49 mg/L (32–65) and ESR 41.5 mm/h (24.6–64.4) in the PMR group. The predominant control indication for PET/CT was malignancy (63.6%). Individual musculoskeletal sites proved insufficient for diagnostic purposes. A novel algorithm comprising 18F-FDG uptake ≥ 2 adjacent to the ischial tuberosities in combination with either abnormalities at the peri-articular shoulder or interspinous bursa achieved a sensitivity of 90.9% and specificity of 92.4% for diagnosing PMR.
Conclusions
The presence of abnormal 18F-FDG uptake adjacent to the ischial tuberosities together with findings at the peri-articular shoulder or interspinous bursa on whole-body PET/CT is highly sensitive and specific for a diagnosis of PMR.
Trial registration
Clinical Trial Registration: Australian New Zealand Clinical Trials Registry, http://www.anzctr.org.au, ACTRN1261400696695

Similar content being viewed by others

References
Dasgupta B, Cimmino MA, Kremers HM, Schmidt WA, Schirmer M, Salvarani C, et al. 2012 Provisional classification criteria for polymyalgia rheumatica: a European League Against Rheumatism/American College of Rheumatology collaborative initiative. Arthritis Rheum. 2012;64:943–54.
Owen CE, Poon AMT, Lee ST, Yap LP, Zwar RB, McMenamin CM, et al. Fusion of positron emission tomography/computed tomography with magnetic resonance imaging reveals hamstring peritendonitis in polymyalgia rheumatica. Rheumatology. 2018;57:345–53.
Yamashita H, Kubota K, Takahashi Y, Minamimoto R, Morooka M, Kaneko H, et al. Similarities and differences in fluorodeoxyglucose positron emission tomography/computed tomography findings in spondyloarthropathy, polymyalgia rheumatica and rheumatoid arthritis. Joint Bone Spine: Revue du Rhumatisme. 2013;80:171–7.
Henckaerts L, Gheysens O, Vanderschueren S, Goffin K, Blockmans D. Use of 18F-fluorodeoxyglucose positron emission tomography in the diagnosis of polymyalgia rheumatica-a prospective study of 99 patients. Rheumatology. 2018;57:1908–16.
Fruth M, Buehring B, Baraliakos X, Braun J. Use of contrast-enhanced magnetic resonance imaging of the pelvis to describe changes at different anatomic sites which are potentially specific for polymyalgia rheumatica. Clin Exp Rheumatol. 2018;36(Suppl 114):86–95.
Leeb BF, Bird HA. A disease activity score for polymyalgia rheumatica. Ann Rheum Dis. 2004;63:1279–83.
Meller J, Strutz F, Siefker U, Scheel A, Sahlmann CO, Lehmann K, et al. Early diagnosis and follow-up of aortitis with [(18)F] FDG PET and MRI. Eur J Nucl Med Mol Imaging. 2003;30:730–6. https://doi.org/10.1007/s00259-003-1144-y.
Dasgupta B, Borg FA, Hassan N, Barraclough K, Bourke B, Fulcher J, et al. BSR and BHPR guidelines for the management of polymyalgia rheumatica. Rheumatology. 2010;49:186–90.
Raina SK. Ratio of controls to cases: a design decision. J Postgrad Med. 2014;60:414.
StataCorp. Stata Statistical Software: Release 13. College Station, TX: StataCorp LP; 2013.
Team RC. R: a language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria; 2013.
B TTA. rpart: Recursive Partitioning and Regression Trees. R package version 41–15; 2019.
Gonzalez-Gay MA, Garcia-Porrua C, Salvarani C, Olivieri I, Hunder GG. The spectrum of conditions mimicking polymyalgia rheumatica in Northwestern Spain. J Rheumatol. 2000;27:2179–84.
Pease CT, Haugeberg G, Morgan AW, Montague B, Hensor EM, Bhakta BB. Diagnosing late onset rheumatoid arthritis, polymyalgia rheumatica, and temporal arteritis in patients presenting with polymyalgic symptoms. A prospective longterm evaluation. [Erratum appears in J Rheumatol. 2005 Sep;32(9):1852]. J Rheumatol. 2005;32:1043–6.
McGonagle D, Pease C, Marzo-Ortega H, O’Connor P, Gibbon W, Emery P. Comparison of extracapsular changes by magnetic resonance imaging in patients with rheumatoid arthritis and polymyalgia rheumatica. J Rheumatol. 2001;28:1837–41.
Marzo-Ortega H, Rhodes LA, Tan AL, Tanner SF, Conaghan PG, Hensor EM, et al. Evidence for a different anatomic basis for joint disease localization in polymyalgia rheumatica in comparison with rheumatoid arthritis. Arthritis Rheum. 2007;56:3496–501.
Mackie SL, Pease CT, Fukuba E, Harris E, Emery P, Hodgson R, et al. Whole-body MRI of patients with polymyalgia rheumatica identifies a distinct subset with complete patient-reported response to glucocorticoids. Ann Rheum Dis. 2015;74:2188–92.
Wakura D, Kotani T, Takeuchi T, Komori T, Yoshida S, Makino S, et al. Differentiation between polymyalgia rheumatica (PMR) and elderly-onset rheumatoid arthritis using 18F-fluorodeoxyglucose positron emission tomography/computed tomography: is enthesitis a new pathological lesion in PMR? PLoS One [Electronic Resource]. 2016;11:e0158509.
Geary MB, Elfar JC. Rotator cuff tears in the elderly patients. Geriatr Orthop Surg Rehabil. 2015;6:220–4.
Milgrom C, Schaffler M, Gilbert S, van Holsbeeck M. Rotator-cuff changes in asymptomatic adults. The effect of age, hand dominance and gender. J Bone Joint Surg Br. 1995;77:296–8.
Klontzas ME, Karantanas AH. Greater trochanter pain syndrome: a descriptive MR imaging study. Eur J Radiol. 2014;83:1850–5.
Sondag M, Guillot X, Verhoeven F, Blagosklonov O, Prati C, Boulahdour H, et al. Utility of 18F-fluoro-dexoxyglucose positron emission tomography for the diagnosis of polymyalgia rheumatica: a controlled study. Rheumatology. 2016;55:1452–7.
Funding
This work was funded by an unrestricted educational grant from Abbvie. Author CO has received research grants from Arthritis Australia and Austin Medical Research Foundation. Author AS is supported by an NHMRC Senior Practitioner Fellowship (APP1084178).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Author CO has received speaking honoraria from Roche, Janssen and Pfizer and meeting sponsorship from Roche. Author AP declares no conflict of interest. Author VY declares no conflict of interest. Author CM declares no conflict of interest. Author SL declares no conflict of interest. Author DL declares no conflict of interest. Author JL has received a speaking honorarium from Abbvie and meeting sponsorship from Gilead. Author AS declares no conflict of interest. Author RB declares no conflict of interest.
Ethical approval
All procedures performed in this study were carried out in accordance with the ethical standards of the Austin Health Human Research Ethics Committee (HREC/14/Austin/158).
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Infection and inflammation
Electronic supplementary material
ESM 1
(DOCX 1970 kb)
Rights and permissions
About this article

Cite this article
Owen, C.E., Poon, A.M.T., Yang, V. et al. Abnormalities at three musculoskeletal sites on whole-body positron emission tomography/computed tomography can diagnose polymyalgia rheumatica with high sensitivity and specificity. Eur J Nucl Med Mol Imaging 47, 2461–2468 (2020). https://doi.org/10.1007/s00259-020-04731-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00259-020-04731-z