
Abstract
Background/purpose
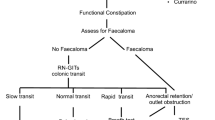
Long-term problems with faecal incontinence occur in up to 50 % of patients after pull-through for Hirschsprung disease (HSCR). The cause often remains unknown, leading to empirical treatments. Using nuclear transit study, we found some patients surprisingly had rapid proximal colonic transit, suspicious of occult diarrhoea. We aimed to assess whether these patients had unrecognized adverse reactions to food.
Methods
Patients (n = 10, all males, 9.6 year; 4.25–15.5 years) with persistent faecal incontinence following pull-through for HSCR referred to the senior author and after exclusion of anatomical defects, underwent nuclear transit studies. Most (8) subsequently underwent breath hydrogen tests for sugar malabsorption and were tested for adverse reactions to food. Exclusion diets for protein allergens, lactose or fructose were then trialed.
Results
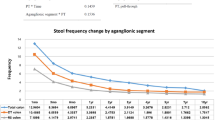
Of the 10 patients with rapid intestinal transit proven on nuclear transit study, breath hydrogen tests for fructose and/or lactose malabsorption were done in 8, and were positive in 7/8 patients. Exclusion diets contributed to either resolution or improvement in faecal incontinence in 9/10 patients.
Conclusions
Rapid transit in the proximal, ganglionated colon may be present in children with faecal incontinence following pull-through for HSCR, possibly secondary to adverse reactions to food. This study suggests that children with post-operative soiling may benefit from a transit study and hydrogen breath tests to diagnose adverse reactions to food caused by sugar malabsorption.

Similar content being viewed by others

References
Rintala RJ, Pakarinen M (2006) Hirschsprung’s disease. In: Oldham K, Stringer M, Mouriquand P (eds) Pediatric surgery and urology: long-term outcomes. Cambridge University Press, Cambridge, pp 385–400
Dasgupta R, Langer JC (2008) Evaluation and management of persistent problems after surgery for Hirschsprung disease in a child. J Pediatr Gastroenterol Nutr 46(1):13–19
Langer JC (2004) Persistent obstructive symptoms after surgery for Hirschsprung’s disease: development of a diagnostic and therapeutic algorithm. J Pediatr Surg 39(10):1458–1462
Levitt MA et al (2009) Hirschsprung disease and fecal incontinence: diagnostic and management strategies. J Pediatr Surg 44(1):271–277
Jarvi K et al (2010) Bowel function and gastrointestinal quality of life among adults operated for Hirschsprung disease during childhood: a population-based study. Ann Surg 252(6):977–981
Zhang SC et al (2007) Long-term outcome, colonic motility, and sphincter performance after Swenson’s procedure for Hirschsprung’s disease: a single-center 2-decade experience with 346 cases. Am J Surg 194(1):40–47
Yik YI et al (2011) Nuclear transit studies of patients with intractable chronic constipation reveal a subgroup with rapid proximal colonic transit. J Pediatr Surg 46(7):1406–1411
Sampson HA et al (2014) Food allergy: a practice parameter update—2014. J Allergy Clin Immunol 134(5):1016–1025
Catto-Smith AG, Trajanovska M, Taylor RG (2007) Long-term continence after surgery for Hirschsprung’s disease. J Gastroenterol Hepatol 22(12):2273–2282
Yik YI et al (2011) Targeting the causes of intractable chronic constipation in children: the Nuclear Transit Study (NTS). In: Singh PN (ed) Radioisotopes—applications in bio-medical science. InTech, pp 305–320
Simren M, Stotzer PO (2006) Use and abuse of hydrogen breath tests. Gut 55(3):297–303
Chumpitazi BP, Nurko S (2011) Defecation disorders in children after surgery for Hirschsprung disease. J Pediatr Gastroenterol Nutr 53(1):75–79
Pastor AC et al (2009) Development of a standardized definition for Hirschsprung’s-associated enterocolitis: a Delphi analysis. J Pediatr Surg 44(1):251–256
Kawai M et al (2005) Cow’s milk allergy presenting Hirschsprung’s disease-mimicking symptoms. Pediatr Surg Int 21(10):850–852
Umeda S et al (2013) Impact of cow’s milk allergy on enterocolitis associated with Hirschsprung’s disease. Pediatr Surg Int 29(11):1159–1163
Di Lorenzo C et al (2000) Colonic motility after surgery for Hirschsprung’s disease. Am J Gastroenterol 95(7):1759–1764
Sutcliffe JR et al (2009) Gastrointestinal transit in children with chronic idiopathic constipation. Pediatr Surg Int 25(6):465–472
Tsampalieros A et al (2008) Dietary fructose intolerance in children and adolescents. Arch Dis Child 93(12):1078
Dabritz J et al (2014) Significance of hydrogen breath tests in children with suspected carbohydrate malabsorption. BMC Pediatr 14:59
Shepherd S, Gibson P (2011) The complete low-FODMAP diet. The Experiment. New York
Bai Y et al (2002) Long-term outcome and quality of life after the Swenson procedure for Hirschsprung’s disease. J Pediatr Surg 37(4):639–642
El Oufir L et al (1996) Relations between transit time, fermentation products, and hydrogen consuming flora in healthy humans. Gut 38(6):870–877
Acknowledgments
L. Stathopoulos was sponsored by Swiss Grants (Fonds du Service de chirurgie pédiatrique et de Perfectionnement du CHUV, the SICPA Foundation, the Société Académique Vaudoise, Lausanne, Switzerland). S. K. King is the recipient of a Career Development Award from the Murdoch Childrens Research Institute. B. S. Southwell was supported by an NHMRC Senior Research Fellowship. Murdoch Childrens Research Institute is supported by the Victorian Government Operational Infrastructure Support Program.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Stathopoulos, L., King, S.K., Southwell, B.R. et al. Nuclear transit study in children with chronic faecal soiling after Hirschsprung disease (HSCR) surgery has revealed a group with rapid proximal colonic treatment and possible adverse reactions to food. Pediatr Surg Int 32, 773–777 (2016). https://doi.org/10.1007/s00383-016-3919-9
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00383-016-3919-9