
Abstract
Alcohol consumption is a leading risk factor and increases the risk of liver diseases, cancers, tuberculosis, and injuries. The relationship between alcohol use and cardiovascular risk is complex. While it is well established that heavy alcohol use and binge drinking harm cardiovascular health, the effect of light-to-moderate alcohol consumption remains controversial. Observational studies have repeatedly confirmed the U- or J-shaped relationship between alcohol consumption and cardiovascular disease risk, with the lowest risk observed in the light-to-moderate drinking group. However, the protective effect of low-level alcohol has been challenged by recent genetic epidemiological studies with Mendelian randomization. Such studies have their own limitations, and the application of this methodology in studying alcohol has been questioned. Results from the latest Global Burden of Diseases, Injuries, and Risk Factors Study suggest that the impact of alcohol consumption on health depends on the age structure and the distribution of disease burden and underlying causes in a given population. For young adults, even small amounts of alcohol cause heath loss. For older adults facing a high burden of cardiovascular diseases, light-to-moderate alcohol consumption may improve cardiovascular health outcomes. Mechanistically, all types of alcoholic beverages, including wine, spirits, and beer, have been shown to increase the levels of high-density lipoprotein cholesterol and adiponectin, and reduce the level of fibrinogen. Nonalcoholic components of wine, especially polyphenolic compounds like resveratrol, may additionally enhance endothelial nitric oxide production, and provide antioxidant and anti-inflammatory effects.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The relationship between alcohol and health risk is a highly complex and controversial issue. It is well known that alcohol consumption increases the risk of liver diseases, cancers, tuberculosis, and injuries [1, 18]. For the cardiovascular system, however, the situation is complicated. While heavy alcohol consumption and binge drinking are clearly harmful for cardiovascular health, it remains a debate in the scientific literature whether light-to-moderate alcohol drinking lowers the risk of cardiovascular diseases and type 2 diabetes.
Evidence supporting protective effects of moderate drinking
Evidence from observational studies
Almost 100 years ago, Raymond Perl reported a U-shaped relationship between the amount of alcohol consumption and mortality. He observed in 1926 a longer lifespan in people drinking moderate amounts of alcohol than both non-drinkers and heavy drinkers [9, 62]. The term “French Paradox” was introduced in 1992 to describe the relatively lower incidence of coronary heart disease in some French populations despite a comparatively high intake of saturated fatty acids [30, 48]. The paradox was attributed to moderate red wine consumption [48].
Later observational studies have repeatedly confirmed the U- or J-shaped relationship between alcohol consumption and cardiovascular disease risk. For instance, a 13-year British study has found the lowest overall mortality in men consuming 8–14 glasses of wine or beer weekly [16]. Small amounts of alcohol are associated with a lower risk of death from ischemic heart disease, and from several other causes [16]. Similarly, a 7-year observation involving 15,400 German participants has led to the finding that men consuming up to 20 g of alcohol per day has the lowest risk of death from cardiovascular causes and death from all causes, with a risk reduction by nearly 50% compared with abstainers [24]. An analysis of 245,207 people in a nationally representative sample of US adults between 1987 and 2000 has found that slightly more than one drink daily is associated with lower cardiovascular mortality. Lifelong abstainers, rare-drinkers, and former drinkers have higher risk of dying from cardiovascular disease than moderate drinkers [36]. A meta-analysis of 84 studies has come to a similar conclusion [50] (Table 1).
The above-mentioned results have also been supported by many other studies. Based on such findings, it has been concluded that light and moderate alcohol consumption may reduce the risk of cardiovascular disease. However, the cardioprotective effects of alcohol do not apply to arrhythmia. Alcohol is a risk factor of atrial fibrillation, which is the most common form of arrhythmia [22, 65]. Alcohol consumption increases the rates of paroxysmal and persistent atrial fibrillation.
The effects of alcohol drinking have also been addressed in the Global Burden of Diseases, Injuries, and Risk Factors (GBD) study, which has investigated premature death and disability from over 300 diseases in 195 countries or territories between 1990 and 2016. To generate an improved estimates on deaths and disability-adjusted life-years caused by alcohol, the authors have used 694 alcohol consumption information sources as well as data from 592 prospective and retrospective studies [18]. Also, in this study, the J-shaped relationship has been observed for ischemic heart disease and diabetes mellitus. However, these protective effects are outweighed by the risks of cancers caused by alcohol use. The study concluded that even small amounts of alcohol use contribute to health loss globally; the safest level of drinking is none [18]. Nevertheless, the GBD 2016 study still supports the concept that moderate alcohol consumption protects from ischemic heart disease.
Four years later, results from the GBD 2020 study were published in 2022 [1]. Importantly, the GBD 2020 study applied a novel approach of weighting relative risk according to levels of underlying disease, and took the impact of geography, age, and sex into account. It has found that the threshold level of alcohol on health loss depends on the age structure and the distribution of disease burden and underlying causes in a given population. The health risks associated with low levels of alcohol consumption differ across regions and are larger for younger than for older populations. In young adults with ages of 15 to 39, the risk of cardiovascular disease is low, and injuries are the major cause of health loss. In the population ages 40 to 64, the disease burden shifts to chronic conditions such as cancer. In people older than 65, cardiovascular diseases account for the majority of health loss. The study showed that even small amounts of alcohol are harmful for younger people at age of 15 to 39. For people over age 40, however, health risks caused by alcohol use vary by age and region. Consuming small amounts of alcohol by people in this age group can provide health benefit by reducing the risk of cardiovascular disease, stroke, and diabetes [1]. The authors recommend a modification of existing policy guidelines by recommending alcohol consumption levels by age, no longer by sex [1].
Evidence from randomized controlled trials
The gold standard to test causal relationships are randomized controlled trials (RCTs), in which confounding factors can be better controlled. However, large-scale RCTs of alcohol use are considered unlikely, or even impossible [20]. Smaller intervention studies indicate that alcohol may have direct effects on the vasculature.
A systematic review and meta-analysis of 63 interventional studies has shown that alcohol increases the levels of high-density lipoprotein (HDL) cholesterol, apolipoprotein A1, and adiponectin. Alcohol also decreases the levels of fibrinogen but does not affect triglyceride levels [6].
In a randomized controlled trail, 224 alcohol-abstaining adults with type 2 diabetes mellitus were randomly assigned to 150 ml of mineral water, white wine, or red wine with dinner for 2 years [19]. Compared with the water group, red wine significantly increased the levels of HDL cholesterol and apolipoprotein A1, whereas white wine decreased fasting plasma glucose level and homeostasis model assessment of insulin-resistance (HOMA-IR) score [19]. Interestingly, only slow ethanol metabolizers (alcohol dehydrogenase alleles [ADH1B*1] carriers) significantly benefited from the effect of both wines on glycemic control, indicating that the effect of wine on glycemic control was mainly driven by alcohol. On the other hand, the stronger effect of red wine than white wine on lipid levels suggests that red wine's effects also involve nonalcoholic constituents [19]. The levels of total phenols (including resveratrol and quercetin) in red wine are known to be 10-fold higher than that in white wine [22].
Evidence against protective effects of moderate drinking
The relationship between moderate alcohol consumption and health risk has raised a great deal of controversy. The conclusion that moderate drinking protects the cardiovascular system has been challenged by many researchers.
Lifestyle factors as confounders
Associations in observational studies do not prove causal relationships. An association of moderate alcohol consumption with lower disease risk does not necessarily mean that moderate alcohol drinking reduces disease risk. The study results can be distorted due to confounding [8, 39, 53]. Compared to heavy drinkers and lifetime abstainers, moderate alcohol drinkers are usually well-educated people with healthy lifestyles, higher socioeconomic status, and better physical health [60]. It is supposed that the “health benefits” may be, at least in part, explained by socioeconomic status [60].
Healthier lifestyle behaviors in light-to-moderate drinkers have also been observed in a recent large-scale cohort study [5]. Compared to non-drinkers and heavy drinkers, this group of alcohol consumers shows lower rates of smoking, lower body-mass index, lower red meat consumption, higher physical activity, and higher vegetable intake [5]. Adjustment for these lifestyle factors leads to a reduction of the cardioprotective associations between modest alcohol intake and cardiovascular risk, confirming the contribution of lifestyle factors to the protective effects observed in moderate alcohol drinkers [5]. The authors supposed that adjustments for further confounding factors may even eliminate the residual, cardioprotective associations observed among light/moderate drinkers. This, however, remains debatable. The residual protective effects after adjustment for the known lifestyle factors are still relatively large and statistically significant [5]. Thus, it is rather unlikely that the protective effects of light-to-moderate drinking are completely attributable to lifestyle factors. A recent study has shown that the protective effects of light-to-moderate drinking are independent of demographic measures and health-related behaviors [32]. The association is evident even after further adjustment for a variety of potential explanatory factors, including physical health status, mental health status, socioeconomic status, social support, childhood factors, and earlier life history of alcohol misuse [32].
The “sick quitter” hypothesis
Another issue is the control group [8]. Current non-drinkers, consisting of never-drinkers and former drinkers, serve as the control group in many studies. It is argued that former drinkers might have stopped drinking because of bad health status or illness. Poorer health, lower socioeconomic status, and less social support have been observed in former drinkers, compared to current drinkers [32]. Thus, the aggregated non-drinking group may be at higher risk, rendering the results artificially to be more favorable for the drinking group. Indeed, a recent large-scale study involving 1.93 million adults has provided evidence for the “sick quitter” hypothesis [4]. Former drinkers have higher risk than never-drinkers in some outcomes including all-cause mortality [4]. Nevertheless, the study results showed that consuming moderate amount of alcohol is associated with a lower cardiovascular risk, even after separation of groups of current non-drinkers, supporting the protective effects of moderate alcohol drinking on the cardiovascular system [4].
Evidence from Mendelian randomization studies
Recent studies attempt to evaluate cause and effect by using Mendelian randomization by treating genetic background as “quasi-experiments” [20]. Ethanol is converted by alcohol dehydrogenase (ADH) to acetaldehyde, which is detoxified by aldehyde dehydrogenase (ALDH). A genetic variant of the ADH1B gene on chromosome 4 (rs1229984) accelerates the conversion of alcohol to acetaldehyde, causing discomfort after drinking alcohol. Even more relevant is the common loss-of-function variant of the ALDH2 gene on chromosome 12 (rs671). A single copy of rs671 is sufficient to decrease acetaldehyde breakdown enough to produce symptoms [33].
In populations of European descent, only the less important variant (rs1229984) of the two is found and the average carriage rate of rs1229984 A-alleles is about 7% [25]. As expected, carriers of the A-allele of ADH1B rs1229984 consume fewer units of alcohol per week and Rs1229984 A-allele carriage is associated with reduced odds of coronary heart disease [25]. However, this association only exists in alcohol drinkers but not in non-drinkers, indicating that associations (reduced risk) ascribed to the ADH1B variant are mainly due to a reduced alcohol consumption [25]. Further subdivision of the drinker category into light, moderate, and heavy shows the same protective effect of the variant across all alcohol categories. These results lead to the conclusion that reduction of alcohol consumption, even for light-to-moderate drinkers, is beneficial for cardiovascular health [25].
In a prospective study involving 512,715 adults in China with 10 years of follow-up, conventional epidemiological analyses have been compared with genetic epidemiological analyses. The later uses Mendelian randomization to study the effects of the two genetic variants that influence alcohol intake [33]. The conventional analyses have resulted in U-shaped associations between the amount of self-reported alcohol intake with stroke and myocardial infarction in male participants. In consistency with previous observations, moderate alcohol intake is found to be associated with the lowest disease risks. On the other hand, genetic epidemiological analyses have found that genotype-predicted alcohol intake amount throughout its range is strongly associated with blood pressure, ischemic stroke, and hemorrhagic stroke, without a U-shaped curve. These results suggest that moderate alcohol intake provides no substantial protective effects [33].
In a recent cohort study including 371,463 individuals from the UK Biobank, genetic instruments for habitual alcohol consumption have been constructed using the single-nucleotide variants identified in genome-wide association studies. The genetic instrument (restricted alcohol use disorder allele score) is strongly associated with alcohol intake in the UK Biobank [5]. Also, in this study, the previously reported J- or U-shaped association between alcohol intake and cardiovascular risk can be recapitulated. However, the study has found that individuals who consumes light and moderate amount of alcohol have healthier lifestyle behaviors compared with people who do not drink, and has attributed the protective effects largely to healthy lifestyle factors [5]. Moreover, the study results support a nonlinear association between alcohol consumption and cardiovascular risk, with light alcohol intake being associated with a minimally increased risk, and heavier alcohol consumption associated with exponentially increased risks of both hypertension and coronary artery disease [5].
Limitations of Mendelian randomization studies
Mendelian randomization represents a breakthrough in epidemiological studies. Despite its scientific value, it has also controversies and problems [20]. Mendelian randomization is in fact a simple observational method and has all the risks of any other non-experimental design [37]. Especially, Mendelian randomization methodology is difficult to apply to alcohol studies, as pointed out by researchers [37]. For example, the ADH1B rs1229984 variant is associated not only with lower reported alcohol consumption but also with more extensive education [25], thus generating a source of confounding [37]. A second form of confounding can occur if parental genotype is associated with outcome [37], which is the case in alcohol studies. Another issue is the problem of pleiotropy. If a genetic locus can affect outcome through multiple different pathways, then the assumption that genotype is a fair proxy for a single exposure of interest is violated [37]. Both the ADH1B rs1229984 variant and the ALDH2 rs671 variant can lead to acetaldehyde accumulation and greater toxicity after alcohol intake. Thus, the effects of these genetic loci can be reasonably interpreted as effect modification of, rather than merely instruments for, the exposure of interest [37]. Furthermore, by changing alcohol metabolism, ADH1B and ALDH2 polymorphisms influence the exposure to both alcohol and its metabolites. If the metabolites have an impact on the outcome (i.e., the risk of cardiovascular disease), one of the core assumptions underlying mendelian randomization is violated [20]. In short, Mendelian randomization studies have their limitations and the results should be interpreted with cautions. A recent a systematic review of 24 Mendelian randomization studies has found substantial heterogeneity [63], with null associations reported for genetically predicted alcohol consumption with the primary outcomes cardiovascular disease and diabetes [63]. The authors have concluded that it is not yet possible to draw conclusions on the causal role of moderate alcohol consumption on cardiometabolic health. With the continuous advancements in the field of Mendelian randomization, its role in triangulation of evidence may become more and more important [63]. However, Mendelian randomization should not be considered a replacement for a long-term RCT.
Potential mechanisms
Vascular function studies in humans
Endothelial function in humans can be assessed non-invasively by the brachial artery flow-mediated dilation (FMD) measurements [13]. Using this technique, it has been shown that heavy alcohol consumption impairs endothelial function with an age-adjusted low %FMD odds ratio of 2.99 [58]. Similarly, binge drinking is associated with impaired vascular function, reducing FMD and enhancing ET-1-induced constriction [21]. Regular moderate-to-heavy intake of alcohol raises blood pressure in humans [35]. On the contrary, the blood pressure falls if moderate-to- heavy drinkers reduce their alcohol intake over periods ranging from 4 weeks to 6 months [47].
In contrast, the effects of low-to-moderate alcohol consumption on FMD are inconsistent. Endothelial function has been reported to be improved [3, 57] or impaired [43, 55] by light-to-moderate alcohol drinking. Other studies have found no changes in FMD [44, 74]. After analyzing 31 published studies, a systematic review article has attributed the inconsistency to multiple reasons including heterogeneity in the pattern and dose of alcohol used as well as subject characteristics [26].
Animal studies
Alcoholic beverages have been shown to reduce atherosclerosis in rabbit [11, 27], mouse [12, 17, 23], and hamster [64] models. Interestingly, protective effects against atherosclerosis have also been observed for low-dose red wine [40], ethanol alone [12, 17, 64], or dealcoholized red wine extracts [11], indicating that both alcohol and non-alcoholic compounds are effective. Some studies show that red wine is more effective than white wine and whiskey in preventing atherosclerosis, while beer is without effects [27].
Potential mechanisms
Vasodilation can be caused by alcoholic beverages and by ethanol itself [3]. Human brachial artery diameter increases after one or two alcoholic drinks, and the extent of vasodilation caused by ethanol or wine is comparable [55]. Also, beer consumption is associated with an improvement of vascular function [56].
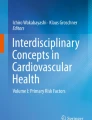
Moderate dose of alcohol (up to 30 g/day) has been shown to increase adiponectin, HDL cholesterol, and apolipoprotein AI, a main protein in HDL cholesterol [6, 49] (Fig. 1). These effects have been consistently observed in all types of alcoholic beverages [6], including wine, spirits, and beer [6, 56].

Disease risk in light-to-moderate alcohol drinkers. Alcohol at any level increases the risk of liver diseases, cancers, tuberculosis, and injuries. On the other hand, light-to-moderate alcohol consumption is associated with cardiovascular protective effects, especially in older adults facing a high burden of cardiovascular diseases. Healthy lifestyles observed among light-to-moderate alcohol drinkers contribute to the health benefits. In addition, alcohol at lower levels can provide direct vasoprotective effects, such as elevation of HDL cholesterol and adiponectin, and reduction of fibrinogen levels. These effects have been shown for wine, beer, and spirits, independent of alcohol type. Polyphenolic compounds (including resveratrol) in wine can provide further benefits by stimulating endothelial nitric oxide (NO) production, inhibiting vascular inflammation, and preventing oxidative stress
Moderate alcohol consumption reduces the circulating levels of fibrinogen [6, 30, 49] (Fig. 1). Red wine and other alcoholic beverages have similar effects so that the beneficial effect on hemostasis is primarily attributable to ethanol [45].
Nevertheless, nonalcoholic components of wine may provide additional benefits, although it is controversial whether the concentration of such compounds is high enough to produce significant effect in vivo [74].
Wine polyphenols are antioxidants and have the potential to prevent low-density lipoprotein (LDL) oxidation, an early step of atherogenesis. Reduced LDL oxidation by wine polyphenols has been shown in human studies [41] and in experimental animals [2, 23]. Moreover, wine polyphenols improve endothelial function and prevent endothelial dysfunction in disease models [42, 52]. Furthermore, polyphenols inhibit angiotensin II-induced upregulation of NADPH oxidase enzymes [51]. At the same time, wine polyphenols increase endothelial NO production [28, 67, 68] (Fig. 1).
Among the wine compounds, resveratrol has received the most attention, both in the scientific community and in the media [54]. Experimental studies have discovered a large range of biological activities of resveratrol in vascular cells [29], including stimulating endothelial NO production [66, 70, 71], inducing mitochondrial biogenesis [10], reducing vascular oxidative stress [29, 61, 72], and inhibiting vascular inflammation [29]. In animal models, resveratrol has been shown to lower blood pressure [46] and suppress atherosclerosis [15, 69].
The results of a number of RCTs with resveratrol are now available. A recent meta-analysis involving 25 RCTs and approximately 600 resveratrol-treated participants has revealed significant effects of resveratrol on glucose and lipid metabolism, decreasing waist circumference, hemoglobin A1c, total cholesterol, LDL cholesterol, and increasing HDL cholesterol [73]. Resveratrol supplementation also improves endothelial function [34]. In patients with cardiovascular disease, resveratrol significantly decreases serum levels of CRP and TNF-α, demonstrating the anti-inflammatory effects of resveratrol [59].
Conclusion
Alcohol use is a leading risk factor for death and disability. The risk of liver disease, cancers, tuberculosis, and injuries is increased by any amount of alcohol. Alcohol intake also reduces global brain volume measures and regional gray matter volumes [14], and is associated with poor mental health, lack of life satisfaction, and psychological distress [31]. Psychological stress and mental health disorders are themselves also risk factors for cardiovascular disease and may thus enhance the alcohol-induced cardiovascular risk. Indeed, many patients with ischemic heart disease do have multiple risk factors; the interaction of these risk factors may result in risk potentiation. For instance, it has been shown that alcohol consumption and smoking have additive adverse effects on endothelial function and arterial stiffness [7, 38].
The relationship between moderate alcohol consumption and cardiovascular health is complex. Observational studies have repeatedly reported the protective effects of light-to-moderate alcohol drinking on cardiovascular disease risk. Although the conclusion has been challenged by recent Mendelian randomization studies, such studies have limitations and the mothodology needs to be further improved and optimized. Latest results from the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) 2020 suggest that impact of alcohol consumption on health loss varies significantly across populations and differs strongly by ages. For young adults, even small amounts of alcohol cause heath loss. For older adults facing a high burden of cardiovascular diseases in many world regions, light-to-moderate alcohol consumption may improve cardiovascular health outcomes.
Data availability
Not applicable.
References
Alcohol Collaborators GBD (2022) Population-level risks of alcohol consumption by amount, geography, age, sex, and year: a systematic analysis for the Global Burden of Disease Study 2020. Lancet 400:185–235. https://doi.org/10.1016/S0140-6736(22)00847-9
Aviram M, Fuhrman B (1998) Polyphenolic flavonoids inhibit macrophage-mediated oxidation of LDL and attenuate atherogenesis. Atherosclerosis 137:S45–S50. https://doi.org/10.1016/s0021-9150(97)00306-7
Bau PF, Bau CH, Naujorks AA, Rosito GA (2005) Early and late effects of alcohol ingestion on blood pressure and endothelial function. Alcohol 37:53–58. https://doi.org/10.1016/j.alcohol.2005.10.034
Bell S, Daskalopoulou M, Rapsomaniki E, George J, Britton A, Bobak M, Casas JP, Dale CE, Denaxas S, Shah AD, Hemingway H (2017) Association between clinically recorded alcohol consumption and initial presentation of 12 cardiovascular diseases: population based cohort study using linked health records. BMJ 356:j909. https://doi.org/10.1136/bmj.j909
Biddinger KJ, Emdin CA, Haas ME, Wang M, Hindy G, Ellinor PT, Kathiresan S, Khera AV, Aragam KG (2022) Association of habitual alcohol intake with risk of cardiovascular disease. JAMA Netw Open 5:e223849. https://doi.org/10.1001/jamanetworkopen.2022.3849
Brien SE, Ronksley PE, Turner BJ, Mukamal KJ, Ghali WA (2011) Effect of alcohol consumption on biological markers associated with risk of coronary heart disease: systematic review and meta-analysis of interventional studies. BMJ 342:d636. https://doi.org/10.1136/bmj.d636
Charakida M, Georgiopoulos G, Dangardt F, Chiesa ST, Hughes AD, Rapala A, Davey Smith G, Lawlor D, Finer N, Deanfield JE (2019) Early vascular damage from smoking and alcohol in teenage years: the ALSPAC study. Eur Heart J 40:345–353. https://doi.org/10.1093/eurheartj/ehy524
Chikritzhs T, Fillmore K, Stockwell T (2009) A healthy dose of scepticism: four good reasons to think again about protective effects of alcohol on coronary heart disease. Drug Alcohol Rev 28:441–444. https://doi.org/10.1111/j.1465-3362.2009.00052.x
Chudzinska M, Wolowiec L, Banach J, Rogowicz D, Grzesk G (2022) Alcohol and cardiovascular diseases—do the consumption pattern and dose make the difference? J Cardiovasc Dev Dis 9. https://doi.org/10.3390/jcdd9100317
Csiszar A, Labinskyy N, Pinto JT, Ballabh P, Zhang H, Losonczy G, Pearson K, de Cabo R, Pacher P, Zhang C, Ungvari Z (2009) Resveratrol induces mitochondrial biogenesis in endothelial cells. Am J Physiol Heart Circ Physiol 297:H13–H20. https://doi.org/10.1152/ajpheart.00368.2009
da Luz PL, Serrano Junior CV, Chacra AP, Monteiro HP, Yoshida VM, Furtado M, Ferreira S, Gutierrez P, Pileggi F (1999) The effect of red wine on experimental atherosclerosis: lipid-independent protection. Exp Mol Pathol 65:150–159. https://doi.org/10.1016/s0014-4800(99)80004-5
Dai J, Miller BA, Lin RC (1997) Alcohol feeding impedes early atherosclerosis in low-density lipoprotein receptor knockout mice: factors in addition to high-density lipoprotein-apolipoprotein A1 are involved. Alcohol Clin Exp Res 21:11–18
Daiber A, Steven S, Weber A, Shuvaev VV, Muzykantov VR, Laher I, Li H, Lamas S, Munzel T (2017) Targeting vascular (endothelial) dysfunction. Br J Pharmacol 174:1591–1619. https://doi.org/10.1111/bph.13517
Daviet R, Aydogan G, Jagannathan K, Spilka N, Koellinger PD, Kranzler HR, Nave G, Wetherill RR (2022) Associations between alcohol consumption and gray and white matter volumes in the UK Biobank. Nat Commun 13:1175. https://doi.org/10.1038/s41467-022-28735-5
Do GM, Kwon EY, Kim HJ, Jeon SM, Ha TY, Park T, Choi MS (2008) Long-term effects of resveratrol supplementation on suppression of atherogenic lesion formation and cholesterol synthesis in apo E-deficient mice. Biochem Biophys Res Commun 374:55–59. https://doi.org/10.1016/j.bbrc.2008.06.113
Doll R, Peto R, Hall E, Wheatley K, Gray R (1994) Mortality in relation to consumption of alcohol: 13 years’ observations on male British doctors. BMJ 309:911–918. https://doi.org/10.1136/bmj.309.6959.911
Emeson EE, Manaves V, Singer T, Tabesh M (1995) Chronic alcohol feeding inhibits atherogenesis in C57BL/6 hyperlipidemic mice. Am J Pathol 147:1749–1758
GBD (2016) Alcohol Collaborators (2018) Alcohol use and burden for 195 countries and territories, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet 392:1015–1035. https://doi.org/10.1016/S0140-6736(18)31310-2
Gepner Y, Golan R, Harman-Boehm I, Henkin Y, Schwarzfuchs D, Shelef I, Durst R, Kovsan J, Bolotin A, Leitersdorf E, Shpitzen S, Balag S, Shemesh E, Witkow S, Tangi-Rosental O, Chassidim Y, Liberty IF, Sarusi B, Ben-Avraham S et al (2015) Effects of initiating moderate alcohol intake on cardiometabolic risk in adults with type 2 diabetes: a 2-year randomized, controlled trial. Ann Intern Med 163:569–579. https://doi.org/10.7326/M14-1650
Glymour MM (2014) Alcohol and cardiovascular disease. BMJ 349:g4334. https://doi.org/10.1136/bmj.g4334
Goslawski M, Piano MR, Bian JT, Church EC, Szczurek M, Phillips SA (2013) Binge drinking impairs vascular function in young adults. J Am Coll Cardiol 62:201–207. https://doi.org/10.1016/j.jacc.2013.03.049
Haseeb S, Alexander B, Baranchuk A (2017) Wine and cardiovascular health: a comprehensive review. Circulation 136:1434–1448. https://doi.org/10.1161/CIRCULATIONAHA.117.030387
Hayek T, Fuhrman B, Vaya J, Rosenblat M, Belinky P, Coleman R, Elis A, Aviram M (1997) Reduced progression of atherosclerosis in apolipoprotein E-deficient mice following consumption of red wine, or its polyphenols quercetin or catechin, is associated with reduced susceptibility of LDL to oxidation and aggregation. Arterioscler Thromb Vasc Biol 17:2744–2752. https://doi.org/10.1161/01.atv.17.11.2744
Hoffmeister H, Schelp FP, Mensink GB, Dietz E, Bohning D (1999) The relationship between alcohol consumption, health indicators and mortality in the German population. Int J Epidemiol 28:1066–1072. https://doi.org/10.1093/ije/28.6.1066
Holmes MV, Dale CE, Zuccolo L, Silverwood RJ, Guo Y, Ye Z, Prieto-Merino D, Dehghan A, Trompet S, Wong A, Cavadino A, Drogan D, Padmanabhan S, Li S, Yesupriya A, Leusink M, Sundstrom J, Hubacek JA, Pikhart H et al (2014) Association between alcohol and cardiovascular disease: Mendelian randomisation analysis based on individual participant data. BMJ 349:g4164. https://doi.org/10.1136/bmj.g4164
Hwang CL, Piano MR, Phillips SA (2021) The effects of alcohol consumption on flow-mediated dilation in humans: a systematic review. Physiol Rep 9:e14872. https://doi.org/10.14814/phy2.14872
Klurfeld DM, Kritchevsky D (1981) Differential effects of alcoholic beverages on experimental atherosclerosis in rabbits. Exp Mol Pathol 34:62–71. https://doi.org/10.1016/0014-4800(81)90036-8
Li H, Forstermann U (2012) Red wine and cardiovascular health. Circ Res 111:959–961. https://doi.org/10.1161/CIRCRESAHA.112.278705
Li H, Xia N, Forstermann U (2012) Cardiovascular effects and molecular targets of resveratrol. Nitric Oxide 26:102–110. https://doi.org/10.1016/j.niox.2011.12.006
Lippi G, Franchini M, Favaloro EJ, Targher G (2010) Moderate red wine consumption and cardiovascular disease risk: beyond the “French paradox”. Semin Thromb Hemost 36:59–70. https://doi.org/10.1055/s-0030-1248725
Makela P, Raitasalo K, Wahlbeck K (2015) Mental health and alcohol use: a cross-sectional study of the Finnish general population. Eur J Public Health 25:225–231. https://doi.org/10.1093/eurpub/cku133
McEvoy LK, Bergstrom J, Tu X, Garduno AC, Cummins KM, Franz CE, Lyons MJ, Reynolds CA, Kremen WS, Panizzon MS, Laughlin GA (2022) Moderate alcohol use is associated with reduced cardiovascular risk in middle-aged men independent of health, behavior, psychosocial, and earlier life factors. Nutrients 14. https://doi.org/10.3390/nu14112183
Millwood IY, Walters RG, Mei XW, Guo Y, Yang L, Bian Z, Bennett DA, Chen Y, Dong C, Hu R, Zhou G, Yu B, Jia W, Parish S, Clarke R, Davey Smith G, Collins R, Holmes MV, Li L et al (2019) Conventional and genetic evidence on alcohol and vascular disease aetiology: a prospective study of 500 000 men and women in China. Lancet 393:1831–1842. https://doi.org/10.1016/S0140-6736(18)31772-0
Mohammadipoor N, Shafiee F, Rostami A, Kahrizi MS, Soleimanpour H, Ghodsi M, Ansari MJ, Bokov DO, Jannat B, Mosharkesh E, Pour Abbasi MS (2022) Resveratrol supplementation efficiently improves endothelial health: a systematic review and meta-analysis of randomized controlled trials. Phytother Res 36:3529–3539. https://doi.org/10.1002/ptr.7562
Mori TA, Burke V, Beilin LJ, Puddey IB (2015) Randomized controlled intervention of the effects of alcohol on blood pressure in premenopausal women. Hypertension 66:517–523. https://doi.org/10.1161/HYPERTENSIONAHA.115.05773
Mukamal KJ, Chen CM, Rao SR, Breslow RA (2010) Alcohol consumption and cardiovascular mortality among U.S. adults, 1987 to 2002. J Am Coll Cardiol 55:1328–1335. https://doi.org/10.1016/j.jacc.2009.10.056
Mukamal KJ, Stampfer MJ, Rimm EB (2020) Genetic instrumental variable analysis: time to call mendelian randomization what it is. The example of alcohol and cardiovascular disease. Eur J Epidemiol 35:93–97. https://doi.org/10.1007/s10654-019-00578-3
Munzel T, Hahad O, Daiber A (2019) Double hazard of smoking and alcohol on vascular function in adolescents. Eur Heart J 40:354–356. https://doi.org/10.1093/eurheartj/ehy430
Naimi TS, Stockwell T, Zhao J, Xuan Z, Dangardt F, Saitz R, Liang W, Chikritzhs T (2017) Selection biases in observational studies affect associations between 'moderate' alcohol consumption and mortality. Addiction 112:207–214. https://doi.org/10.1111/add.13451
Napoli C, Balestrieri ML, Sica V, Lerman LO, Crimi E, De Rosa G, Schiano C, Servillo L, D'Armiento FP (2008) Beneficial effects of low doses of red wine consumption on perturbed shear stress-induced atherogenesis. Heart Vessels 23:124–133. https://doi.org/10.1007/s00380-007-1015-8
Nigdikar SV, Williams NR, Griffin BA, Howard AN (1998) Consumption of red wine polyphenols reduces the susceptibility of low-density lipoproteins to oxidation in vivo. Am J Clin Nutr 68:258–265. https://doi.org/10.1093/ajcn/68.2.258
Oak MH, Auger C, Belcastro E, Park SH, Lee HH, Schini-Kerth VB (2018) Potential mechanisms underlying cardiovascular protection by polyphenols: Role of the endothelium. Free Radic Biol Med 122:161–170. https://doi.org/10.1016/j.freeradbiomed.2018.03.018
Oda N, Kajikawa M, Maruhashi T, Iwamoto Y, Kishimoto S, Matsui S, Hidaka T, Kihara Y, Chayama K, Goto C, Aibara Y, Nakashima A, Noma K, Tomiyama H, Takase B, Yamashina A, Higashi Y (2017) Endothelial function is impaired in relation to alcohol intake even in the case of light alcohol consumption in Asian men; Flow-mediated Dilation Japan (FMD-J) Study. Int J Cardiol 230:523–528. https://doi.org/10.1016/j.ijcard.2016.12.065
Oda N, Kajikawa M, Maruhashi T, Kishimoto S, Yusoff FM, Goto C, Nakashima A, Tomiyama H, Takase B, Yamashina A, Higashi Y (2020) Endothelial function is preserved in light to moderate alcohol drinkers but is impaired in heavy drinkers in women: flow-mediated Dilation Japan (FMD-J) study. PLoS One 15:e0243216. https://doi.org/10.1371/journal.pone.0243216
Pellegrini N, Pareti FI, Stabile F, Brusamolino A, Simonetti P (1996) Effects of moderate consumption of red wine on platelet aggregation and haemostatic variables in healthy volunteers. Eur J Clin Nutr 50:209–213
Prysyazhna O, Wolhuter K, Switzer C, Santos C, Yang X, Lynham S, Shah AM, Eaton P, Burgoyne JR (2019) Blood pressure-lowering by the antioxidant resveratrol is counterintuitively mediated by oxidation of cGMP-dependent protein kinase. Circulation 140:126–137. https://doi.org/10.1161/CIRCULATIONAHA.118.037398
Puddey IB, Zilkens RR, Croft KD, Beilin LJ (2001) Alcohol and endothelial function: a brief review. Clin Exp Pharmacol Physiol 28:1020–1024. https://doi.org/10.1046/j.1440-1681.2001.03572.x
Renaud S, de Lorgeril M (1992) Wine, alcohol, platelets, and the French paradox for coronary heart disease. Lancet 339:1523–1526. https://doi.org/10.1016/0140-6736(92)91277-f
Rimm EB, Williams P, Fosher K, Criqui M, Stampfer MJ (1999) Moderate alcohol intake and lower risk of coronary heart disease: meta-analysis of effects on lipids and haemostatic factors. BMJ 319:1523–1528. https://doi.org/10.1136/bmj.319.7224.1523
Ronksley PE, Brien SE, Turner BJ, Mukamal KJ, Ghali WA (2011) Association of alcohol consumption with selected cardiovascular disease outcomes: a systematic review and meta-analysis. BMJ 342:d671. https://doi.org/10.1136/bmj.d671
Sarr M, Chataigneau M, Martins S, Schott C, El Bedoui J, Oak MH, Muller B, Chataigneau T, Schini-Kerth VB (2006) Red wine polyphenols prevent angiotensin II-induced hypertension and endothelial dysfunction in rats: role of NADPH oxidase. Cardiovasc Res 71:794–802. https://doi.org/10.1016/j.cardiores.2006.05.022
Schini-Kerth VB, Auger C, Kim JH, Etienne-Selloum N, Chataigneau T (2010) Nutritional improvement of the endothelial control of vascular tone by polyphenols: role of NO and EDHF. Pflugers Arch 459:853–862. https://doi.org/10.1007/s00424-010-0806-4
Schooling CM, Leung GM (2022) Alcohol and health. Lancet 400:1765. https://doi.org/10.1016/S0140-6736(22)02124-9
Silva P, Portillo MP, Fernandez-Quintela A (2022) Resveratrol and wine: an overview of thirty years in the digital news. Int J Environ Res Public Health 19. https://doi.org/10.3390/ijerph192315815
Spaak J, Merlocco AC, Soleas GJ, Tomlinson G, Morris BL, Picton P, Notarius CF, Chan CT, Floras JS (2008) Dose-related effects of red wine and alcohol on hemodynamics, sympathetic nerve activity, and arterial diameter. Am J Physiol Heart Circ Physiol 294:H605–H612. https://doi.org/10.1152/ajpheart.01162.2007
Spaggiari G, Cignarelli A, Sansone A, Baldi M, Santi D (2020) To beer or not to beer: a meta-analysis of the effects of beer consumption on cardiovascular health. PLoS One 15:e0233619. https://doi.org/10.1371/journal.pone.0233619
Suzuki K, Elkind MS, Boden-Albala B, Jin Z, Berry G, Di Tullio MR, Sacco RL, Homma S (2009) Moderate alcohol consumption is associated with better endothelial function: a cross sectional study. BMC Cardiovasc Disord 9:8. https://doi.org/10.1186/1471-2261-9-8
Tanaka A, Cui R, Kitamura A, Liu K, Imano H, Yamagishi K, Kiyama M, Okada T, Iso H, Investigators C (2016) Heavy alcohol consumption is associated with impaired endothelial function. J Atheroscler Thromb 23:1047–1054. https://doi.org/10.5551/jat.31641
Teimouri M, Homayouni-Tabrizi M, Rajabian A, Amiri H, Hosseini H (2022) Anti-inflammatory effects of resveratrol in patients with cardiovascular disease: a systematic review and meta-analysis of randomized controlled trials. Complement Ther Med 70:102863. https://doi.org/10.1016/j.ctim.2022.102863
Towers A, Philipp M, Dulin P, Allen J (2018) The “health benefits” of moderate drinking in older adults may be better explained by socioeconomic status. J Gerontol B Psychol Sci Soc Sci 73:649–654. https://doi.org/10.1093/geronb/gbw152
Ungvari Z, Orosz Z, Rivera A, Labinskyy N, Xiangmin Z, Olson S, Podlutsky A, Csiszar A (2007) Resveratrol increases vascular oxidative stress resistance. Am J Physiol Heart Circ Physiol 292:H2417–H2424. https://doi.org/10.1152/ajpheart.01258.2006
University of Minnesota Raymond Pearl on alcohol and longevity. http://www.epi.umn.edu/cvdepi/essay/raymond-pearl-on-alcohol-and-longevity/
van de Luitgaarden IAT, van Oort S, Bouman EJ, Schoonmade LJ, Schrieks IC, Grobbee DE, van der Schouw YT, Larsson SC, Burgess S, van Ballegooijen AJ, Onland-Moret NC, Beulens JWJ (2022) Alcohol consumption in relation to cardiovascular diseases and mortality: a systematic review of Mendelian randomization studies. Eur J Epidemiol 37:655–669. https://doi.org/10.1007/s10654-021-00799-5
Vinson JA, Teufel K, Wu N (2001) Red wine, dealcoholized red wine, and especially grape juice, inhibit atherosclerosis in a hamster model. Atherosclerosis 156:67–72. https://doi.org/10.1016/s0021-9150(00)00625-0
Voskoboinik A, Prabhu S, Ling LH, Kalman JM, Kistler PM (2016) Alcohol and atrial fibrillation: a sobering review. J Am Coll Cardiol 68:2567–2576. https://doi.org/10.1016/j.jacc.2016.08.074
Wallerath T, Deckert G, Ternes T, Anderson H, Li H, Witte K, Forstermann U (2002) Resveratrol, a polyphenolic phytoalexin present in red wine, enhances expression and activity of endothelial nitric oxide synthase. Circulation 106:1652–1658
Wallerath T, Poleo D, Li H, Forstermann U (2003) Red wine increases the expression of human endothelial nitric oxide synthase: a mechanism that may contribute to its beneficial cardiovascular effects. J Am Coll Cardiol 41:471–478
Wallerath T, Li H, Godtel-Ambrust U, Schwarz PM, Forstermann U (2005) A blend of polyphenolic compounds explains the stimulatory effect of red wine on human endothelial NO synthase. Nitric Oxide 12:97–104. https://doi.org/10.1016/j.niox.2004.12.004
Wang Z, Zou J, Cao K, Hsieh TC, Huang Y, Wu JM (2005) Dealcoholized red wine containing known amounts of resveratrol suppresses atherosclerosis in hypercholesterolemic rabbits without affecting plasma lipid levels. Int J Mol Med 16:533–540
Xia N, Daiber A, Habermeier A, Closs EI, Thum T, Spanier G, Lu Q, Oelze M, Torzewski M, Lackner KJ, Munzel T, Forstermann U, Li H (2010) Resveratrol reverses endothelial nitric-oxide synthase uncoupling in apolipoprotein E knockout mice. J Pharmacol Exp Ther 335:149–154. https://doi.org/10.1124/jpet.110.168724
Xia N, Strand S, Schlufter F, Siuda D, Reifenberg G, Kleinert H, Forstermann U, Li H (2013) Role of SIRT1 and FOXO factors in eNOS transcriptional activation by resveratrol. Nitric Oxide 32:29–35. https://doi.org/10.1016/j.niox.2013.04.001
Xia N, Daiber A, Forstermann U, Li H (2017) Antioxidant effects of resveratrol in the cardiovascular system. Br J Pharmacol 174:1633–1646. https://doi.org/10.1111/bph.13492
Zhou Q, Wang Y, Han X, Fu S, Zhu C, Chen Q (2022) Efficacy of resveratrol supplementation on glucose and lipid metabolism: a meta-analysis and systematic review. Front Physiol 13:795980. https://doi.org/10.3389/fphys.2022.795980
Zilkens RR, Burke V, Hodgson JM, Barden A, Beilin LJ, Puddey IB (2005) Red wine and beer elevate blood pressure in normotensive men. Hypertension 45:874–879. https://doi.org/10.1161/01.HYP.0000164639.83623.76
Funding
Open Access funding enabled and organized by Projekt DEAL. The authors were supported by the Deutsche Forschungsgemeinschaft (DFG grants LI-1042/1-1, LI-1042/3-1, LI-1042/5-1, and XI 139/2-1) and by a research grant from the Boehringer Ingelheim Foundation for the collaborative research consortium “Novel and neglected cardiovascular risk factors: molecular mechanisms and therapeutic implications.”
Author information
Authors and Affiliations
Contributions
H. L. wrote the manuscript text. H. L. and N. X. reviewed and edited the manuscript.
Corresponding author
Ethics declarations
Ethics approval
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the special issue on Impact of life style and behavioral risk factors on endothelial function and vascular biology in Pflügers Archiv—European Journal of Physiology
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Li, H., Xia, N. Alcohol and the vasculature: a love-hate relationship?. Pflugers Arch - Eur J Physiol 475, 867–875 (2023). https://doi.org/10.1007/s00424-023-02818-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00424-023-02818-8