
Abstract
Threatening sporadic outbreaks of avian influenza and the H1N1 pandemic of 2009 highlight the need for rapid and accurate detection and typing of influenza viruses. In this paper, we describe the validation of the VereFlu™ Lab-on-Chip Influenza Assay, which is based on the integration of two technologies: multiplex reverse transcription (RT)-PCR followed by microarray amplicon detection. This assay simultaneously detects five influenza virus subtypes, including the 2009 pandemic influenza A (H1N1), seasonal H1N1, H3N2, H5N1 and influenza B virus. The VereFlu™ assay was clinically validated in Singapore and compared against reference methods of real-time PCR, virus detection by immunofluorescence of cell cultures and sequencing. A sensitivity and specificity of 96.8% and 92.8%, respectively, was demonstrated for pandemic H1N1; 95.7% and 100%, respectively, for seasonal H1N1; 91.2% and 97.6%, respectively, for seasonal H3N2; 95.2% and 100%, respectively, for influenza B. Additional evaluations carried out at the World Health Organization (WHO) Collaborating Centre, Melbourne, Australia, confirmed that the test was able to reliably detect H5N1. This portable, fast time-to-answer (3 hours) device is particularly suited for diagnostic applications of detection, differentiation and identification of human influenza virus subtypes.
Similar content being viewed by others


Background
Influenza type A viruses are classified by the antigenic properties of their surface glycoproteins into 16 hemagglutinin (HA) and 9 neuraminidase (NA) subtypes [1]. Influenza B viruses are not subtyped. Historically, only three HA subtypes, H1, H2 and H3, have been responsible for pandemic outbreaks. This includes the 2009 outbreak caused by a novel influenza A (H1N1) virus of swine origin [2]. In contrast, all virus subtypes and combinatorial possibilities of HA and NA have been detected in wild birds and poultry [3]. Since 1997, highly pathogenic avian influenza (HPAI) viruses, in particular the H5N1 subtype, have jumped the species barrier and caused ongoing sporadic fatal outbreaks in humans [4]. Therefore, the looming threat of pandemics from influenza viruses cannot be overlooked, and assays that enable rapid, accurate identification and subtyping of influenza viruses is pertinent for surveillance and outbreak management.
The increasing popularity of chip-based DNA microarrays reflects their tremendous diagnostic potential and utility for rapid detection and subtyping of influenza viruses [5–11]. Of late, a handful of respiratory virus microarrays have been produced commercially, such as the INFINITI® FLU A-sH1N1 QUAD Assay (AutoGenomics, Inc., Carlsbad, CA), the FluChip (InDevR, Boulder, CO) and the FDA-cleared VRNAT assay (Verigene®, Northbrook, IL). The last of these is designed to detect influenza A and B viruses and respiratory syncytial viruses A and B using a glass slide array. The INFINITI® FLU A-sH1N1 QUAD Assay and the FluChip assays are, however, still for research use only.
In our study, we describe the development and validation of the VereFlu™ assay, which, to our knowledge, is the first commercially available integrated lab-on-chip (LOC) device that combines reverse transcription (RT)-PCR amplification followed by amplicon hybridization to a DNA microarray for the specific detection of clinically important influenza virus subtypes, including the 2009 pandemic influenza (H1N1) and H5N1 viruses.
Materials and methods
VereFlu™ assay – system overview
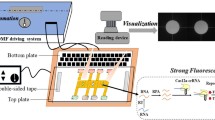
The hardware that is required to run the chips comprises a computer, a thermal control system (TCS), which enables PCR thermal cycling, and a microarray optical reader (Lean s.r.l., Medolla, Italy). The accompanying software controls the instrumentation and also generates the analysis report. The workflow of the system and the processing time of each step is listed below.
-
1.
Extraction of viral RNA (vRNA) from the sample. This can be done either manually using spin-columns or using automated extraction systems (~45 min).
-
2.
vRNA is mixed with RT-PCR master mix and pipetted into the microfluidic channels of the VereFlu™ chip that lead into a rapid, miniaturized PCR reactor
-
3.
The chip is loaded onto a thermal reactor of the TCS, allowing multiplex PCR amplification to be performed on-chip (90 min)
-
4.
Hybridization of amplicons to the microarray (30 min)
-
5.
Spot image analysis (1 min/chip). The total assay time including RNA extraction is approximately 3 h.
Design of VereFlu™ assay probes and primers
Hemagglutinin (HA) and neuraminidase (NA) genes were used as targets for probe and primer design. Gene sequences from human, avian, pandemic influenza A and influenza B viruses were downloaded from GenBank’s Influenza Virus Resource (http://www.ncbi.nlm.nih.gov/genomes/FLU/FLU.html) as well as from Global Initiative on Sharing All Influenza Data (GISAID) (http://platform.gisaid.org/). The sequences were aligned using the BioEdit sequence alignment editor version 7.0.5.3, and highly conserved regions resulting from the alignment were used for probe and primer design. As shown in Table 1, HA-specific primers were designed for pandemic and seasonal H1N1, H3N2, H5N1 and influenza B viruses. Additional primers and probes were designed against the NA segments of pandemic H1N1 and H5N1 to facilitate subtyping. Reverse primers were synthesized with the addition of a 5′-terminal Cy5 label (Sigma Proligo, Singapore). The capture probes were designed using the variable regions of the genes (Table 1). The assay comprised 14 influenza-virus-specific PCR primers and a set of forward and reverse PSII primers for the amplification of a PCR-positive control of plant origin (Table 1). Together, these primers constituted the VereFlu™ primer mix A. There were 23 influenza targeted capture probes, 2 RT-PCR control probes, and positive and negative hybridization control probes (Table 1).
Clinical sample collection and processing
Singapore
A total of 277 respiratory samples (throat and nasal swabs) were collected from patients presenting influenza-like illness with fever ≥38°C, cough, sore throat, headache and muscle ache. The samples were collected from May 2008 to August 2009 by sentinel physicians participating in a local influenza surveillance programme. The specimens were transported from their site of collection to the National Public Health Laboratory (NPHL), Singapore, where sample processing was carried out. All specimens were subjected to influenza virus detection by real-time RT-PCR and shell-vial culture followed by immunofluorescence (IF) assay.
Swabs taken from patients using flocked swabs (Copan Diagnostics, Murrieta, CA) were transported in 3 ml of Copan Universal Transport Medium (UTM). UTM specimens were divided into two aliquots. One aliquot was used for viral culture using standard shell vial technique and the other was subject to nucleic acid extraction using an EZ1 BioRobot (QIAGEN, Hilden, Germany). Extracted RNA was eluted in 60 μl of buffer, and the nucleic acid samples were stored at −80°C until required for PCR analysis.
Real-time RT-PCR detection of influenza A virus has been described by Spackman and colleagues [12]. Samples that were positive for influenza A virus were further subtyped into H1 or H3 using the protocol described by the Public Health Laboratory Services Branch, Centre for Health Protection (CHP), Department of Health, Hong Kong SAR, China (http://www.chp.gov.hk/files/pdf/CHP_Protocols_for_the_Detection_of_Human_Swine_Influenza.pdf). The detection of pandemic influenza A (H1N1) 2009 was based on the nucleoprotein (NP) gene, using primers and probes designed by the NPHL. The detection of influenza B virus has been described by Krafft et al. [13]. All RT-PCRs reactions were set up using QuantiTect Probe PCR kits (QIAGEN) with the amplification performed on a LightCycler 2.0 Real-Time PCR System (Roche, Mannheim, Germany). PCR protocols, primer and probe sequences are available upon request from the authors.
For the isolation of influenza virus, the aliquoted specimen in transport medium was passed through a 0.22-μm Acrodisc syringe filter (Pall Corp., Ann Arbor, MI) and inoculated into a shell vial (Diagnostic Hybrids, Inc., Columbus, OH) containing a monolayer of Madin-Darby canine kidney (MDCK) cells. After two days of incubation at 37°C, the direct IF test using fluorescein-isothiocyanate-conjugated (FITC) monoclonal antibodies (Light Diagnostics, Concord Road, Billerica, MA) specific for influenza A and B viruses was used to detect and differentiate between the viruses. A Zeiss inverted fluorescent microscope was used to examine the samples for positively staining cells. Influenza-virus-positive cultures were stored at −80°C for future use.
WHO Collaborating Centre for Reference and Research on Influenza, Melbourne, Australia
Virus isolates in MDCK cell culture and clinical specimens of influenza A virus, including pandemic influenza A (H1N1) virus, were submitted to the WHO Collaborating Centre for Reference and Research on Influenza at Victorian Infectious Diseases Reference Laboratory (VIDRL) from WHO National Influenza Centres, regional laboratories and hospitals from Australia, New Zealand, and the Asia/Pacific region. Viruses were grown in MDCK cells and/or embryonated chicken eggs [14]. Virus growth was monitored by observing cytopathic effect, and the presence of haemagglutination activity was observed using turkey red blood cells as described previously [14]. The isolates were tested using a standard haemagglutination inhibition assay (HAI) against a panel of reference viruses and their homologous ferret antisera [14]. vRNA was extracted from either clinical specimens or from viruses grown in MDCK cell cultures as described previously [15]. Real-time RT-PCR was also performed to determine the type and subtype of viruses from clinical specimens as described previously [14].
VereFlu™ assay PCR amplification
The multiplex RT-PCR reaction was performed using a QuantiTect Virus+ROX Vial Kit (QIAGEN, Ontario, Canada) in a total volume of 25 μl. The RT-PCR master mix was prepared by adding the following components: 5 μl of 5X QT Virus NR Master Mix, 1 μl of VereFlu™ primer mix A, 3 μl of RNAse-free water, 0.5 μl of RNase inhibitor (20 U/μl), 0.5 μl of QT Virus RT Mix, 10 μl of the RNA template and 5 μl of PSII amplification control. PSII is in vitro-transcribed RNA derived from the chloroplast-encoded gene psbA from a mungbean plant (GenBank: GQ89302). The RT-PCR mix was pipetted into chip inlets leading to the PCR micro-reactor where amplification takes place. The chip was sealed and placed into the TCS. The cycling parameters used were as follows: 15 min at 50°C; 5 min at 95°C; 45 cycles of 15 sec at 95°C, 30 sec at 50°C and 45 sec at 72°C.
Microarray hybridization, detection and data analysis
Upon completion of RT-PCR, the chip was extracted from the TCS and unsealed. For hybridization of amplicons to the microarray, 14.5 μl of hybridization mix was pipetted into the chip inlets such that the final buffer composition was 1 mM phosphate buffer, 2.7 mM KCl, 500 mM NaCl, 1X Denhardt’s solution, 0.05 % Tween 20 and 0.5 nM each of the positive hybridization controls AT730, AT776, AT683 (Table 1). The chip was re-sealed and placed into the TCS. Heat denaturation of amplicons was performed at 2 min at 95°C, followed by a 30-min hybridization at 55°C. After the hybridization, the chips were unsealed and washed for 2 min at room temperature in Falcon tubes filled with 50 ml of 0.3X SSC/0.05% sodium dodecyl sulfate and dried by centrifugation at 3000 rpm for 2 min in a 50-ml Falcon tube. The dried chip was scanned in an optical reader (Lean s.r.l.). Spot segmentation and intensity calculation of the microarray image was performed by overlaying a virtual grid over the microarray image using the corner features as reference points. Spot images detected within the grid were computed for background and signal values [16]. A signal-to-noise ratio of >3.0 was defined as a positive result.
In vitro transcription
Recombinant plasmids bearing synthetic 2009 pandemic influenza A (H1N1) HA and NA genes with T7 promoter sequences at their 5’ ends were obtained from Integrated DNA Technology, Inc. (IDT Inc, Coralville, IA). Recombinant plasmids bearing HA and NA genes from clinical isolates of influenza A H1N1, H3N2 and influenza B (ATCC VR01535) viruses were generated in-house. The plasmids were linearized by restriction digestion using SalI (New England Biolabs Inc, Ipswich, MA) for the NA gene and SacII (Promega, Madison, WI) for the HA gene. In vitro transcripts (IVTs) were generated using Riboprobe® In Vitro Transcription System (Promega) and quantified using an Agilent 2100 Bioanalyzer RNA 6000 Nano Kit (Agilent Technology, Santa Clara, CA).
Analytical sensitivity
IVTs of HA and NA gene segments from clinical isolates of influenza A H1N1 and H3N2 viruses and an ATCC isolate of influenza B virus (VR01535) were used for the determination of analytical sensitivity. The RNA concentration was measured using a Nanodrop ND-1000 spectrophotometer Nanodrop Technologies, Wilmington, DE). The RNA copy number was calculated using the following formula: RNA concentration [X g/μl RNA] / (transcript length [bp] x 340) x 6.022 x 1023, and tenfold serial dilutions of the HA and NA RNA transcripts were made. The LoD and cutoff values were determined in triplicate for the RNA transcripts. The LoD was the lowest concentration of RNA that could give a 95% detection rate for that virus type for all triplicates. The cutoff value for detection was defined as the lowest RNA concentration that would yield a positive assay result 50% of the time.
Analytical specificity
The analytical specificity of the VereFlu™ assay was evaluated using a panel of nine commonly found non-influenza respiratory viruses purchased from the American Type Culture Collection (ATCC), Manassas, VA. Strains included respiratory syncytial virus A2 ATCC VR-1540, respiratory syncytial virus B1 ATCC VR-1400, human coronavirus OC43 ATCC VR-1588, human parainfluenza virus 1 ATCC VR-94, human parainfluenza virus 2 ATCC VR-92, human parainfluenza virus 4b ATCC VR-1377, human rhinovirus 4 ATCC VR-484, human adenovirus type 7 ATCC VR-7, and human adenovirus type 4 ATCC VR-1572. The production of viral stocks was performed by propagating each virus in its appropriate cell line, and the 50% tissue culture infectious dose (TCID50) of each virus was determined. RNA was extracted from each virus sample using a QIAamp Viral Mini Kit (QIAGEN) and tested in triplicate at high RNA concentrations (>105 TCID50/ml). Intra-assay specificity was evaluated by testing three influenza viruses (seasonal influenza A [H1N1], influenza A [H3N2] and influenza B) and IVTs of NA and HA from pandemic influenza A (H1N1) virus against primers and capture probes of the Vereflu™ assay.
Clinical sensitivity and specificity
Clinical samples were subjected to nucleic acid extraction using an EZ1 BioRobot (QIAGEN), and 10 μl of the extracted nucleic acid was used in each VereFlu™ assay reaction. The evaluations were carried out at three local hospitals, and the results were collated and presented as a single table (Table 3).
Assay reproducibility
Quantified viral stocks of influenza A (H3N2) virus, influenza B virus and negative samples were used for assessing intra-assay and inter-assay reproducibility. Low, moderate and strong positives were prepared from influenza A (H3N2) and influenza B virus RNA. The Ct values for H3N2 low, moderate and strong positive samples were 33, 31 and 24, respectively, whilst the Ct values for influenza B low, moderate and strong positive samples were 28, 26, and 20, respectively. LoD and cutoff RNA copy number concentrations provided the basis for low and medium positives. Testing was carried out at each concentration using 30 influenza virus samples in triplicate and 10 negative samples also in triplicate. Studies were conducted with two runs per day, at two local test sites by two operators, over a test period of 5 days. The percentage of agreement with the expected result was calculated.
Statistical analysis
The sensitivity and specificity of the VereFlu™ assay were calculated by comparison to a combination of reference methods, which included RT-PCR, sequencing of the HA segment, virus culture and immunoassays. For sensitivity and specificity results, the 95% confidence interval CI for a proportion was calculated using the Wilson score method without continuity correction [17].
Results
Analytical sensitivity and specificity
The LoD is defined as the RNA concentration that would yield a positive assay result 95% of the time. For all the virus types tested, the LoD was determined to be 102 copies/reaction (Table 2). The cutoff detection was defined as the RNA copy number that could be detected 50% of the time, and this was determined to be 50 copies for both influenza A (H3N2) virus and influenza B virus. For pandemic and seasonal H1N1, the cutoff was determined to be not higher than 2 × 102 copies/reaction.
The VereFlu™ assay was tested with a panel of 9 non-influenza viruses, 3 different influenza A virus subtypes (H1N1, H3N2, H5N1) and influenza B virus. No cross-reaction was observed with the influenza viruses tested. With the non-influenza respiratory viruses, cross-reactions were noted for the 2009 pandemic influenza capture probe with human coronavirus OC43 and influenza B capture probes with human adenovirus type 7. These were considered minor cross-reactions, as their probe signal-to-noise ratios were weakly positive. Also, in both cases, only one of the triplicate samples was positive. Hence, the overall analytical specificity for the VereFlu™ assay was calculated to be 96%.
Clinical evaluation of the VereFlu™ assay, Singapore
The VereFlu™ assay was validated at three sites in Singapore using a total of 277 respiratory samples (Table 3). The assay showed good sensitivity (>91%) and excellent specificity (100%) for all the influenza viruses tested.
Evaluation of the VereFlu™ assay at WHO, Melbourne
The system was evaluated using clinical and cell-cultured virus samples. Additionally, avian influenza A (H5N1) virus testing was also performed. Overall, out of the 44 samples tested, the VereFlu™ assay results for 40 specimens (91%) were concordant with the reference methods. All (n = 4) influenza-negative samples tested negative.
Specifically, the VereFlu™ assay detected the influenza viruses in positive samples as follows: 10/12 (83.3%) for pandemic H1N1, 3/3 (100%) for seasonal H1N1, 2/2 (100%) for H5N1, 7/9 (77.7%) for H3N2 and 18/18 (100%) for influenza B. Observations by the research investigators indicated that the assay was able to detect both lineages of influenza B viruses (Yamagata and Victoria lineages) and influenza A viruses of different clades, including H5N1.
Assay reproducibility
The reproducibility of the VereFlu™ assay is presented in Table 4. When tested at RNA copy numbers that would give moderate and strong positives for H3N2 and influenza B, the assays were highly reproducible (>91%). As expected, when low RNA copy numbers were tested, the reproducibility dropped to almost 50% for H3N2 and 70% for influenza B.
Discussion
Here, we report the development and evaluation of a portable and easy-to-use diagnostic platform, the VereFlu™ assay, for the typing and subtyping of human influenza virus. The test is based on an on-chip multiplex RT-PCR amplification followed by detection using a microarray, and it can be performed fairly rapidly, taking about 3 h to complete. Each TCS or thermal reactor accommodates a maximum of five chips, which can be run either simultaneously or independently using different protocols. The modular nature of the system allows the linkup of more than one TCS unit to the computer, hence enabling the system to be adapted to the throughput needs of either large- or small-scale diagnostic settings. Laboratory reproducibility data from our study suggest that the assay is easy to handle, which is an important consideration during outbreak situations.
The overall clinical sensitivity for all influenza A viruses tested was 94.3%, and the specificity was 96.8%. These values were comparable to those obtained in similar microarray based influenza virus typing assays [18, 19]. It is known that microarray-based detection and typing of influenza viruses is generally less sensitive than performing a real-time PCR [9, 19]. Our analytical sensitivity was determined to be 102 copies/reaction for each influenza type. These figures are similar to those reported by Huang et al. [9], at 102 RNA copies/reaction for seasonal H3N2, H1N1, H5N1 and influenza B virus. The detection limit for a multiplex PCR assay has been reported to be 50 copies for influenza A and influenza B viruses [20], which explains why some of the samples that were typed and confirmed by the reference methods of cell culture and real-time RT PCR were missed by the VereFlu™ assay.
In our laboratory, we use real-time PCR to detect influenza A virus and then follow up with a second subtyping PCR when influenza A positives are detected. We anticipate that the VereFlu™ assay will ease that process, since detection and subtyping is done simultaneously on-chip. Multiplexing capabilities of real-time PCR reactions are typically limited to a fourplex as restricted by the number of fluorescence acquisition channels present in the PCR instrument. In contrast, the detection format in the VereFlu™ assay is low-density-array-based, allowing tens to hundreds of capture probes to be spotted and correspondingly allowing a similar number of amplicons to be detected. Hence, the arrays have a much greater detection capability for robust parallel testing than real-time PCR.
Given the high mutational frequency of influenza virus genomes [21] efforts taken to increase the specificity of the VereFlu™ assay included the use of short capture probes of 21 to 28 nucleotides [22] as well as the incorporation of probe redundancy. The capture probes were designed to detect between 2 and 4 sections of the targeted gene and may be useful in overcoming the problem of misdiagnosis due to capture probes failing to hybridize with the amplicon as a result of gene polymorphisms. In our assay, capture probe cross-reactions were observed for the 2009 pandemic influenza A (H1N1) probe with human coronavirus OC43 and the influenza B capture probe with human adenovirus type 7. During the testing of clinical samples, false positives of this nature will be unlikely, as hybridization to only one capture probe (instead of both probes for influenza B virus or all three probes for 2009 pandemic H1N1) is insufficient to permit the VereFlu™ software to call a positive result. Instead, the operator will be alerted that the particular influenza gene segment has been detected, and a re-test will be advised. We are working on applying a more stringent hybridization wash, which may solve the problem of cross-reactions.
Conclusions
In summary, we have developed a lab-on-chip device that has been clinically evaluated both locally and at WHO, Melbourne. The system was found to be reliable and accurate for the identification of clinically significant influenza viruses and could potentially prove to be a valuable method for routine influenza surveillance as well as outbreak events.
References
Fouchier R, Munster V, Wallensten A, Bestebroer T, Herfst S, Smith D, Rimmelzwaan G, Olsen B, Osterhaus A (2005) Characterization of a novel influenza A virus hemagglutinin subtype (H16) obtained from black-headed gulls. J. Virol. 79:2814–2822
Gatherer D (2009) The 2009 H1N1 influenza outbreak in its historical context. J. Clin. Virol 45:174–178
Olsen B, Munster V, Wallensten A, Waldenström J, Osterhaus A, Fouchier R (2006) Global patterns of influenza a virus in wild birds. Science 312:384–388
Suguitan A, Subbarao K (2006) The Pandemic Threat of Avian Influenza Viruses. Perspectives in Medical Virology 16:97–132
Kessler N, Ferraris O, Palmer K, Marsh W, Steel A (2004) Use of the DNA flow-thru chip, a three-dimensional biochip, for typing and subtyping of influenza viruses. J. Clin. Microbiol. 42:2173–2185
Liu R, Lodes M, Nguyen T, Siuda T, Slota M, Fuji H, McShea A (2006) Validation of a fully integrated microfluidic array device for influenza A subtype identification and sequencing. Anal. Chem. 78:4184–4193
Han X, Lin X, Liu B, Hou Y, Huang J, Wu S, Liu J, Mei L, Jia G, Zhu Q (2008) Simultaneously subtyping of all influenza A viruses using DNA microarrays. J. Virol. Methods 152:117–121
Townsend M, Dawson E, Mehlmann M, Smagala J, Dankbar D, Moore C, Smith C, Cox N, Kuchta R, Rowlen K (2006) Experimental evaluation of the FluChip diagnostic microarray for influenza virus surveillance. J. Clin. Microbiol. 44:2863–2871
Huang Y, Tang H, Duffy S, Hong Y, Norman S, Ghosh M, He J, Bose M, Henrickson K, Fan J, Kraft A, Weisburg W, Mather E (2009) Multiplex assay for simultaneously typing and subtyping influenza viruses by use of an electronic microarray. J. Clin. Microbiol. 47:390–396
Kang X, Li Y, Sun H, Wu W, Liu H, Lin F, Qing C, Chang G, Zhu Q, Chen W, Yang Y (2010) Subtype identification of the novel A H1N1 and other human influenza A viruses using an oligonucleotide microarray. Arch. Virol. 155:55–61
Li X, Qi X, Miao L, Wang Y, Liu F, Gu H, Lu S, Yang Y, Liu F (2009) Detection and subtyping of influenza A virus based on a short oligonucleotide microarray. Diagn. Microbiol. Infect. Dis. 65:261–270
Spackman E, Senne D, Myers T, Bulaga L, Garber L, Perdue M, Lohman K, Daum L, Suarez D (2002) Development of a real-time reverse transcriptase PCR assay for type A influenza virus and the avian H5 and H7 hemagglutinin subtypes. J. Clin. Microbiol. 40:3256–3260
Krafft A, Russell K, Hawksworth A, McCall S, Irvine M, Daum L, Connoly J, Reid A, Gaydos J, Taubenberger J (2005) Evaluation of PCR testing of ethanol-fixed nasal swab specimens as an augmented surveillance strategy for influenza virus and adenovirus identification. J. Clin. Microbiol. 43:1768–1775
Barr I, Komadina N, Hurt AC, Shaw R, Durrant C, Lannello P, Tomasov C, Sjogren H, Hampson A (2003) Reassortants in recent human influenza A and B isolates from South East Asia and Oceania. Virus Res. 98:35–44
Barr I, Deng Y, Lannello P, Hurt A, Komadina N (2008) Adamantane resistance in influenza A(H1) viruses increased in 2007 in South East Asia but decreased in Australia and some other countries. Antivir. Res. 80:200–205
Qin L, Rueda L, Ali A, Ngom A (2005) Spot detection and image segmentation in DNA microarray data. Appl. Bioinformatics 4:1–11
Newcombe RG (1998) Two-sided confidence intervals for the single proportion: Comparison of seven methods. Stats. Med. 17:857–872
Mehlmann M, Bonner A, Williams J, Dankbar D, Moore C, Kuchta R, Podsiad A, Tamerius J, Dawson E, Rowlen K (2007) Comparison of the MChip to viral culture, reverse transcription-PCR, and the QuickVue influenza A + B test for rapid diagnosis of influenza. J. Clin. Microbiol 45:1234–1237
Gall A, Hoffmann B, Harder T, Grund C, Höper D, Beer M (2009) Design and validation of a microarray for detection, hemagglutinin subtyping, and pathotyping of avian influenza viruses. J. Clin. Microbiol 47:327–334
Boivin G, Côté S, Déry P, De Serres G, Bergeron M (2004) Multiplex real-time PCR assay for detection of influenza and human respiratory syncytial viruses. J. Clin. Microbiol. 42:45–51
Ghedin E, Sengamalay N, Shumway M, Zaborsky J, Feldblyum T, Subbu V, Spiro D, Sitz J, Koo H, Bolotov P, Dernovoy D, Tatusova T, Bao Y, St George K, Taylor J, Lipman D, Fraser C, Taubenberger J, Salzberg S (2005) Large-scale sequencing of human influenza reveals the dynamic nature of viral genome evolution. Nature 437:1162–1166
Suzuki S, Ono N, Furusawa C, Kashiwagi A, Yomo T (2007) Experimental optimization of probe length to increase the sequence specificity of high-density oligonucleotide microarrays. BMC Genomics 8:373–386
Acknowledgments
The work that was carried out at the National University Hospital, Singapore, was supported by the Ministry of Health, Singapore (HSDP06/X04).
The Melbourne WHO Collaborating Centre for Reference and Research on Influenza is supported by the Australian Government Department of Health and Ageing.
Conflict of interest
The author(s) declare that they have no competing interests.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Teo, J., Pietro, P.D., Biagio, F.S. et al. VereFlu™: an integrated multiplex RT-PCR and microarray assay for rapid detection and identification of human influenza A and B viruses using lab-on-chip technology. Arch Virol 156, 1371–1378 (2011). https://doi.org/10.1007/s00705-011-0999-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00705-011-0999-7