
Abstract
Background
Seroma formation is the most common postoperative complication after laparoscopic inguinal hernia repair. Recurrence and seroma formation may be difficult to distinguish. Many adjunctive techniques with which to reduce the incidence of seroma formation after laparoscopic inguinal repair have been described in the literature; however, the evidence for using intraoperative adjunctive techniques is limited. Therefore, the present systematic review was performed to evaluate the effects and limitations of adjunctive techniques used during laparoscopic inguinal hernia repair.
Methods
Major databases (PubMed, Embase, Springer, and Cochrane Library) were searched using the terms “seroma,” “laparoscopic inguinal hernia”, “TAPP”, “TEP”, “inguinal hernia”, “tack”, “barbed suture”, “drainage”, “Endoloop technique”, and “fibrin sealant”. All studies involving adults undergoing laparoscopic/endoscopic inguinal hernioplasty with at least one intervention designed to reduce seroma formation were included.
Results
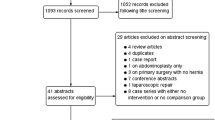
Of the 965 studies identified, 8 met the inclusion criteria. Six adjunctive techniques were described in the literature. Transversalis fascia (TF) inversion with tacking: one prospective non-randomized controlled study revealed a lower incidence of postoperative seroma after TF inversion with tacking for direct inguinal hernias (4.17% vs. 14.29%, P < 0.05). Endoloop technique: one prospective study of 76 cases involving this technique revealed a low incidence of seroma formation (3.9% at 2 weeks) in direct hernias. Barbed suture closure of TF: one prospective study of 36 direct hernias reported only one clinical palpable seroma that resolved 1 month later. Surgical drains: three trials reported the results of drains, and the pooling results demonstrated significantly less seroma formation in patients with surgical drains (2.1 vs. 23.8%; odds ratio 0.12; 95% confidence interval 0.08–0.19; P < 0.0001). Fibrin sealant: one prospective clinical study of 40 patients with indirect inguinal hernias reported a lower volume (P < 0.001) and lower incidence (5% vs. 15%) of seroma formation in the fibrin group. Distal sac fixation technique: in one prospective study of six patients with large inguinoscrotal hernias, one patient developed a seroma on postoperative day 8.
Conclusion
Seroma formation is a natural process that cannot be completely prevented following laparoscopic inguinal hernioplasty, especially in patients with direct and large indirect inguinal hernias. Some intraoperative adjunctive techniques are effective in reducing clinically palpable seroma formation in select patients. More randomized controlled trials are needed for further evaluation.


Similar content being viewed by others


References
Bittner R, Montgomery MA, Arregui E et al (2015) International Endohernia Society update of guidelines on laparoscopic (TAPP) and endoscopic (TEP) treatment of inguinal hernia (International Endohernia Society). Surg Endosc 29(2):289–321
Köckerling F, Bittner R, Adolf D, Fortelny R et al (2017) Seroma following transabdominal preperitoneal patch plasty (TAPP): incidence, risk factors, and preventive measures. Surg Endosc. https://doi.org/10.1007/s00464-017-5912-3 (Epub ahead of print)
Leibl BJ, Schmedt CG, Kraft K et al (2000) Scrotal hernias: a contraindication for an endoscopic procedure? Results of a single-institution experience in transabdominal preperitoneal repair. Surg Endosc 14:289–292
Misra MC, Bhowate PD, Bansal VK et al (2009) Massive scrotal hernias: problems and solutions. J Laparoendosc Adv Surg Tech 19:19–22
Lau H, Lee F (2003) Seroma following endoscopic extraperitoneal inguinal hernioplasty. Surg Endosc 17:1773–1777
Reddy VM, Sutton CD, Bloxham L et al (2007) Laparoscopic repair of direct inguinal hernia: a new technique that reduces the development of postoperative seroma. Hernia 11:393–396
Cihan A, Ozdemir H, Uçan BH et al (2006) Fade or fate. Seroma in laparoscopic inguinal hernia repair. Surg Endosc 20(2):325–328
Azoury SC, Rodriguez-Unda N, Soares KC et al (2015) The effect of TISSEEL fibrin sealant on seroma formation following complex abdominal wall hernia repair: a single institutional review and derived cost analysis. Hernia 19(6):935–942
Morales-Conde S, Suarez-Artacho G, Socas-Macias M, Barranco-Moreno A (2015) Retroprosthetic seroma after laparoscopic ventral hernia repair: incidence, risk factors and clinical significance. Hernia 19(6):943–947
Moher D, Liberati A, Tetzlaff J, Altman DG (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. J Clin Epidemiol 62:1006–1012
Higgins JP, Altman DG, Gotzsche PC et al (2011) The Cochrane collaboration’s tool for assessing risk of bias in randomized trials. BMJ 343:d5928
Slim K, Nini E, Forestier D et al (2003) Methodological index for non-randomized studies (minors): development and validation of a new instrument. ANZ J Surg 73(9):712–716
Ismail M, Garg M, Rajagopal M, Garg P (2009) Impact of closed-suction drain in preperitoneal space on the incidence of seroma formation after laparoscopic total extraperitoneal inguinal hernia repair. Surg Laparosc Endosc Percutan Tech 19(3):263–266
Gao D, Wei S, Zhai C et al (2015) Clinical research of preperitoneal drainage after endoscopic totally extraperitoneal inguinal hernia repair. Hernia 19(5):789–794
Fan JKM, Liu J, Chen K et al (2018) Preperitoneal closed-system suction drainage after totally extraperitoneal hernioplasty in the prevention of early seroma formation: a prospective double-blind randomised controlled trial. Hernia 22(3):455–465
Daes J (2014) Endoscopic repair of large inguinoscrotal hernias: management of the distal sac to avoid seroma formation. Hernia 18(1):119–122
Li J, Zhang W (2018) Closure of a direct inguinal hernia defect in laparoscopic repair with barbed suture: a simple method to prevent seroma formation? Surg Endosc 32(2):1082–1086
Sürgit Ö, Çavuşoğlu NT, Kılıç M et al (2016) Use of fibrin glue in preventing pseudorecurrence after laparoscopic total extraperitoneal repair of large indirect inguinal hernia. Ann Surg Treat Res 91(3):127–132
Berney CR (2012) The Endoloop technique for the primary closure of direct inguinal hernia defect during the endoscopic totally extraperitoneal approach. Hernia 16:301–305
Park A, Birch DW, Lovrics P (1998) Laparoscopic and open incisional hernia repair: a comparison study. Surgery 124:816–821
Fang Z, Ren F, Zhou J, Tian J (2015) Biologic mesh versus synthetic mesh in open inguinal hernia repair: system review and meta-analysis. ANZ J Surg 85(12):910–916
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflict of interest.
Ethical approval
This study design conformed to ethical standards.
Human and animal rights
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed consent
There were no individual participants included in this study.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Li, J., Gong, W. & Liu, Q. Intraoperative adjunctive techniques to reduce seroma formation in laparoscopic inguinal hernioplasty: a systematic review. Hernia 23, 723–731 (2019). https://doi.org/10.1007/s10029-019-01903-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10029-019-01903-1