
Abstract
Aim
The coronavirus disease 2019 (COVID-19) has caused hundreds of thousands of deaths, impacted the flow of life and resulted in an immeasurable amount of socio-economic damage. However, not all of this damage is attributable to the disease itself; much of it has occurred due to the prevailing misinformation around COVID-19. This rapid integrative review will draw on knowledge from the literature about misinformation during previous abrupt large-scale infectious disease outbreaks to enable policymakers, governments and health institutions to proactively mitigate the spread and effect of misinformation.
Subject and methods
For this rapid integrative review, we systematically searched MEDLINE and Google Scholar and extracted the literature on misinformation during abrupt large-scale infectious disease outbreaks since 2000. We screened articles using predetermined inclusion criteria. We followed an updated methodology for integrated reviews and adjusted it for our rapid review approach.
Results
We found widespread misinformation in all aspects of large-scale infectious disease outbreaks since 2000, including prevention, treatment, risk factor, transmission mode, complications and vaccines. Conspiracy theories also prevailed, particularly involving vaccines. Misinformation most frequently has been reported regarding Ebola, and women and youth are particularly vulnerable to misinformation. A lack of scientific knowledge by individuals and a lack of trust in the government increased the consumption of misinformation, which is disseminated quickly by the unregulated media, particularly social media.
Conclusion
This review identified the nature and pattern of misinformation during large-scale infectious disease outbreaks, which could potentially be used to address misinformation during the ongoing COVID-19 or any future pandemic.
Similar content being viewed by others

Background
The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is a novel virus in the coronavirus family causing the coronavirus disease 2019 (COVID-19) (Okan et al. 2020). COVID-19 was first reported in December 2019 and has since evolved into the sixth large-scale worldwide outbreak of the twenty-first century following the Severe Acute Respiratory Syndrome (SARS) outbreak in 2002 (Felter 2020). Estimates suggest that COVID-19 is nearly twice as contagious as the seasonal flu and takes much longer to present symptoms, making transmission of the virus through asymptomatic carriers a substantial public health challenge (Tosta 2020). Given the lack of widespread use of a safe and effective vaccine against COVID-19, public compliance with measures, such as physical distancing, hand hygiene and wearing masks, is essential to intercepting transmission links (Cheng et al. 2020). Dissemination and consumption of clear, consistent and credible information about COVID-19 is a prerequisite to public compliance with these preventative measures (Van den Broucke 2020).
Both the dissemination and consumption of information have spiked since the COVID-19 pandemic (Zarocostas 2020). During the Munich Security Conference in February 2020, the Director-General of the World Health Organization (WHO) urged, ‘we’re not just fighting an epidemic; we’re fighting an infodemic” (World Health Organization 2020). Infodemic is short for “information epidemic’, depicting the rapid spread and amplification of vast amounts of valid and invalid information (Okan et al. 2020). The Internet, social media and other communication platforms have eroded traditional vertical health communication strategies by allowing misinformation to horizontally diffuse faster than ever before (Wang et al. 2019; Cuan-Baltazar et al. 2020). The infodemic makes it difficult for the public to comply with public health measures, as it can debilitate individuals’ ability to distinguish mis- and disinformation from fact and cause false perceptions of true risk, including both a higher perceived risk and a false sense of safety (Van den Broucke 2020; Okan et al. 2020). The spread of misinformation can also incite fear and panic, which has been found to induce mistrust in government and non-government institutions leading the pandemic response and further increase susceptibility to misinformation, conspiracy theories and rumours (Wang et al. 2019). Examining the past spread of misinformation during large-scale disease outbreaks can inform initiatives to tackle the spread of misinformation during the COVID-19 pandemic and ultimately improve public compliance with essential preventative health measures. We conducted a rapid integrative review to quickly synthesize existing literature about misinformation during recent abrupt large-scale infectious disease outbreaks, which we hope will enable policymakers, governments and health institutions to proactively mitigate the spread of misinformation during the current pandemic.
Methods
Rapid integrative review
A rapid review generates knowledge promptly by skipping some of the steps involved in a systematic review by simplifying the overall review process to produce a quick result (Khangura et al. 2012). This approach to knowledge synthesis is useful to explore a new frontier of research, update previous research knowledge, and provide a quick overview of a certain topic where time constraints exist to be able to convey the results to policymakers and/or translate the knowledge into action swiftly. This rapid integrative review primarily followed the integrative rapid review methodology developed by Whittemore and Knafl (2005) with adjustments suggested by other authors for a rapid review (Khangura et al. 2014; Tricco et al. 2015). As integrative reviews synopsise previous scientific literature to obtain a comprehensive concept of a particular research topic (Broome 2000), this approach has been deemed best fitting for this review. The review strategy is described below.
Problem identification
For this rapid review, we identified the following research questions:
-
1.
What research has been undertaken regarding the spread of misinformation during abrupt large-scale infectious disease outbreaks in the past 20 years?
-
2.
What factors determine the spread of misinformation among communities?
-
3.
What sources of information are associated most with the spread of misinformation?
-
4.
What aspects of a disease outbreak were affected by the misinformation (i.e. preventive behaviour, treatment, vaccine, etc.)?
Study selection
To extract the relevant studies on misinformation during recent abrupt large-scale infectious disease outbreaks, we used specific search terms and selected those databases that would best ensure the inclusion of sufficient relevant studies. We included the following disease outbreaks in our study per our search criteria: Severe Acute Respiratory Distress Syndrome (SARS), H1N1 Influenza (swine flu), Ebola, Zika virus, Middle East Respiratory Syndrome (MERS), and COVID-19. We followed the PICOS structure (Table 1) to determine our inclusion criteria for this review. We did not limit studies to a particular country. However, we restricted the time of publication to the past 20 years (2001 to 2020). We included studies published in the English language only.
Literature search
The research team selected the two most appropriate databases from which to mine the information relevant to the research focus of this review. MEDLINE (Ovid) was selected as the richest academic database for infectious disease outbreaks. However, as misinformation during a pandemic/epidemic often involves research articles from multiple disciplines, including social and political sciences and education and geography, and non-peer-reviewed publications, we included a search of the grey literature to capture literature on misinformation during disease outbreaks from those sources. Moreover, grey databases also help extract unpublished or in-progress studies. We selected Google Scholar, which is very commonly used to capture grey literature and can extract studies indexed in other databases as well (Haddaway et al. 2015; Vaska et al. 2019). A complete list of search terms is provided in Table 2. In addition, we also conducted single citation searches and used a pearl growing approach by reviewing the reference lists of all selected publications to ensure all relevant articles were included.
Screening
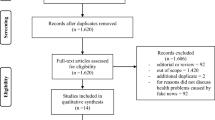
We screened all search outcomes through a two-step process: (i) title-abstract review, and (ii) full-text review (Fig. 1). As suggested in the common rapid review strategies (Tricco et al. 2015), only one reviewer of the research team screened the studies following the two-step process (the title-abstract screening and full-text screening. In the first screening step, the reviewer screened the papers based on the relevance of their titles and abstracts to our research question. After title-abstract screening, relevant abstracts and those from which the reviewer could not draw conclusions alone were included for further review. The full texts of the eligible abstracts were studied thoroughly for inclusion in the rapid review if found relevant to the research questions. Any indecision regarding an article to include or not were resolved by the team consensus.

PRISMA diagram for the selected studies regarding misinformation during large-scale disease outbreaks of the twenty-first century
Data extraction
The research team reviewer extracted relevant information using a limited and predetermined abstraction tool. Firstly, study characteristics were extracted, including citations, study location, study method, study objective and study sample (Table 3). Further data on the specific disease outbreak, the misinformation arising around the disease, how the misinformation or misconceptions were addressed, factors determining the spread of misinformation and sources of mis/information were abstracted following emergent coding (Table 4). EndNote and Microsoft Excel were used in different stages of the study.
Data analysis
The final stage of a rapid review brings together the findings from all eligible articles to deliver an evidence-based response to the original research question. Data were collected, synthesised and presented using summary tables. Extracted data were charted and examined to identify any patterns of information in the articles. The results of this process were further examined to identify key themes. Table 4 details the key findings of each paper regarding misinformation during the outbreaks of interest.
Results
Literature search overview
Our systematic search of MEDLINE identified 533 articles. We found an additional 398 articles in our grey literature search of Google Scholar. After removing duplicates, 853 articles were identified for title and abstract screening. After reviewing the titles and abstracts, 118 articles were chosen for full-text screening. Through full-text screening, 37 articles were considered eligible for the study (Fig. 1).
Content overview
Table 3 illustrates the study contents we extracted from the studies included in this review. Most studies were conducted in the United States (12 of 37) followed by Canada and Nigeria. Thirty-four of 37 studies were published between 2011 and 2020. The study population of the studies were diverse, including physicians, school teachers, youth and students, general community members.
Objectives of the studies
A number of studies analysed content from social and mainstream media and other document sources. The majority of the studies focused on social media and the spread of information and misinformation across different social media platforms. There were also studies that assessed the knowledge, beliefs, practices and behaviour of community people during a widespread disease outbreak (Table 3). The effects of misinformation during a pandemic, the role of different information sources for risk communication, or multiple aspects of the rumour process were evaluated by some of the selected studies.
Data source and collection strategies
Overall, most of the studies collected data directly from individuals through surveys, focus groups and interviews (n = 21). The majority of them collected data from community individuals using surveys (n = 16). Three studies used both surveys and focus groups, one study used both surveys and interviews, and only one undertook only interviews. Eleven studies performed a content analysis of various social media, including Facebook, Twitter, YouTube, Sina Weibo, Reddit, Gab, LinkedIn, Pinterest, GooglePlus, Instagram and Flicker. Most of these studies analysed multiple platforms; however, Twitter was the most common social platform analysed in the studies (n = 11). Five other studies analysed the content of mass media, including online news sites and mainstream newspapers. One study conducted surveys and interviews and content analysis of social media.
Sources of information
In our rapid review, we sought to extract those sources from which people receive information during an outbreak. In studies conducted within the community, participants described receiving a range of information sources. In the case of social media (predominantly content analysis), some studies reported social media as a direct source, whereas others reported the original source of shared content on social media as the information source, usually given as a link/reference on a particular social media post. Overall, the most commonly reported sources of information were mass media (n = 17). Among mass media, the most common source of information was the mainstream news agency (n = 9), followed by TV (n = 4) and radio (n = 4), and unspecified mass media (n = 3). Three studies reported social media in general as the source of information. Twitter was reported in four studies, Facebook in two studies, and YouTube and Instagram in one study each. Official/government health information sites were reported in six studies. Alternative internet-based news media and blogs were reported in four studies and emergency texting was mentioned in only one study. Other sources included friends and family (n = 4), healthcare providers (n = 4), religious leaders (n = 1) and word of mouth (n = 2).
The prevalence of misinformation among individuals and information sources
We also extracted the percentage of people (if the data source was individuals) and percentage of sources (if the data source was social/mass media or other documents) having misinformation and/or a lack of proper knowledge about the diseases. Overall, among individuals, the level of misinformation ranged from approximately 30% to 88%, as reported in the studies. Regarding various online and offline content, 2% to 23.8% of the content was reported as misinformation.
Outbreaks
Ebola was the most commonly studied outbreak that appeared in the literature. Twelve studies were conducted on the Ebola virus disease, which re-emerged extensively in 2014 (first discovered in 1976) and ran a widespread course across West Africa. The second most frequently studied disease was the Zika virus, which is a mosquito-transmitted flavivirus mostly spread from Brazil during 2015–2016. A handful of studies were found pertaining to H1N1 influenza (also known as swine flu), which had an outbreak in 2009 (n = 7). The most recent COVID-19 outbreak was the focus of research in four studies, followed by SARS (n = 2) and MERS (n = 2), whose outbreaks occurred in 2002 and 2017, respectively.
Discourse of misinformation
Various misinformation was reported in the studies eligible for this review. We attempted to catalogue them according to the different levels of outbreak response. This information is presented in Table 4.
Prevention-related misinformation
The most prevalent misinformation was about preventing Ebola by taking a daily hot water bath with salt (Adebimpe et al. 2015). Regarding the prevention of Zika, even some physicians were misinformed that Zika-infected or -exposed persons need to be isolated (Abu-Rish et al. 2019). Regarding SARS, a study in China that explored newspaper databases found ‘blasting firecrackers to keep evil spirits away’ was the most common piece of misinformation reported in 29 of 90 news stories they uncovered (Tai and Sun 2011). Only one prevention-related misinformation was reported about MERS, which was putting Vaseline® (petroleum jelly) under the nose, which was claimed to prevent MERS infection (Song et al. 2017).
Treatment-related misinformation
Saltwater was found as a treatment measure for Ebola across studies (Fung et al. 2016). Sixteen to 17 % of people in one study believed the Zika virus can be treated with antibiotics and/or consuming a certain amount of onions (Adebimpe et al. 2015). A study on H1N1 influenza reported that many people believed since there was no definitive treatment for H1N1 influenza, there was no need for medical consultation, as that could potentially cause panic and fear among the population (Lau et al. 2009).
Risk factor- and disease causation-related misinformation
One study found that 53% of participants believed Ebola came from wild animals from forests, such as monkeys and bats (Kasereka and Hawkes 2019). A rumour claiming that lack of iodine caused SARS lead to panic buying of salt during that pandemic in China (Ding 2009). Some people who usually did not contract seasonal flu asserted they would be safe from H1N1 influenza as well, which may give them a false sense of safety and deter them from getting vaccinated (Boerner et al. 2013).
Mode of transmission-related misinformation
One study found that over two-thirds (68%) of people believed Ebola could be spread via the mere touch of a diseased person (Bali et al. 2016). Other misinformation about mode of transmission of Ebola included consumption of pork, and transmission through air, water and food (Buli et al. 2015; Bali et al. 2016). More than half of the participants in one study among physicians (55.9%) believed the Zika virus could be transmitted via direct contact between individuals (Abu-Rish et al. 2019).
Complication-related misinformation
In terms of misinformation about complications of disease outbreaks, the most commonly observed misinformation about Zika was that a pesticide/larvicide caused microcephaly, a complication that followed Zika virus infection in pregnant women (Miller et al. 2017; Sommariva et al. 2018).
Vaccine-related misinformation
A study in Ghana found news articles and people claming that the vaccine would cause Ebola by either the vaccine itself or the government and researchers would intentionally infect people with Ebola to test the vaccines (Kummervold et al. 2017). Two studies on H1N1 influenza found people who considered the vaccine unsafe were hindered from getting vaccinated (Kanadiya and Sallar 2011; Boerner et al. 2013).
Conspiracy theories
About one-fifth of the US citizens in one American study believed in at least one Zika conspiracy theory (Klofstad et al. 2019). The most widespread conspiracy theory about the Zika virus concerned microcephaly and that it was a complication of the Zika virus infection caused by pesticides/larvicides (Carey et al. 2020; Sharma et al. 2017) and vaccines (Wood 2018). A population-based survey in Congo found 45.9% of people believed at least one of the following three conspiracy theories: Ebola did not exist (25.5% believed), Ebola was a political fabrication (32.6%) and Ebola was fabricated to destabilize the region (36.4%) (Kasereka and Hawkes 2019).
Factors that help spread belief in misinformation
We extracted different factors associated with believing and spreading misinformation during an outbreak (Table 5).
Demographic factors
According to several studies, women and young people were most prone to believing misinformation and passing it on to others (Balami and Meleh 2019). Possessing below secondary level education was also associated with having improper knowledge about Ebola (Gidado et al. 2015). A study reported that being single (65.24%) was related to believing misinformation more than married people (34.76%) (Balami and Meleh 2019).
Intrapersonal factors
One study stated that while misconceptions were associated with increased anxiety, some sort of anxiety also drove people to take preventive action (Kanadiya and Sallar 2011). Similarly, another study found that worried people were more likely to have a positive intention to take the H1N1 influenza vaccine (Naing et al. 2012).
Interpersonal/social factors
A study that conducted focus groups to determine factors that interplay with H1N1 vaccine uptake behaviour found that the ‘bandwagoning’ effect played a role in this context, that is, if everyone else was getting vaccinated, others followed suit; but if everyone was not, others avoided it (Boerner et al. 2013).
Professional/experiential factors
A study on physicians in Jordan found less than five years of experience as a physician was significantly related to having misinformation about the Zika virus (Abu-Rish et al. 2019). Other studies indicated that people having an academic background with a biology major (such as public health, biological sciences, biochemistry, pharmaceutical sciences and nursing) or who were in the scientific field had a lower level of misinformation than individuals from other fields, such as the arts and management sciences (Koralek et al. 2016; Pennycook et al. 2020).
Information source-related factors
Misinformation about Ebola reinforced by the media amplified unjustified fear among people (Seltzer et al. 2015; Bali et al. 2016). Studies that analysed content and responses to misinformation by the different social media platforms found that while some social media such as YouTube and Reddit reduced unreliable posts or remained neutral (Twitter), some rather amplified posts containing misinformation (Gab) (Ghenai and Mejova 2017; Bora et al. 2018; Cinelli et al. 2020).
Risk communication-related factors
One study found that two-thirds of participants (66.5%) either believed (27.5%) that the H1N1 vaccine was not safe or did not have any idea about its safety (39%), which influenced over 63% of people’s refusal to be vaccinated (Kanadiya and Sallar 2011). Lack of accurate public discourse about the diseases from authentic and reliable sources was also reverberated by other studies (Chew and Eysenbach 2010; Stanley et al. 2020).
Government/authority-related factors
During the SARS outbreak in 2002 in China, it was observed that when the Chinese government initially denied and remained silent about the outbreak and restricted the mainstream media from broadcasting accurate news about the SARS outbreak, various misinformation arose and caused panic and fear among people (Ding 2009; Tai and Sun 2011).
Discussion
Our rapid integrative review found that misinformation involves prevention, treatment, risk factor and disease causation, mode of transmission, complications, vaccines and conspiracy theories. Among recent large-scale infectious outbreaks, Ebola was the most commonly studied in the literature for misinformation. Women and young people were reported to be more prone to believing and passing on misinformation. Anxiety, worrying and a lack of experience in the scientific field was associated with the consumption of misinformation. Mass media, particularly social media, was largely found to contribute to the dissemination of misinformation. A lack of government efforts and a lack of trust in government efforts were also found to contribute to the spread of misinformation.
Misinformation is not only an issue during large-scale infectious disease outbreaks; the advent of the Internet and social media have exacerbated the creation and dissemination of misinformation in all areas of health (Chou et al. 2018). Social media feeds are closed networks curated to individual beliefs that amplify misinformation by creating ‘information silos’ and ‘echo chambers’. From dangerous rumours about vaccines (Dubé et al. 2014; Ortiz-Sánchez et al. 2020), tobacco products (Albarracin et al. 2018), alternative therapies (Wilson 2002; Schmidt and Ernst 2004), and weight loss cures (Dedrick et al. 2020) to skepticism about medical guidelines (Fiscella et al. 1998), there is an ever-growing need to curb misinformation.
Most of the misinformation-related studies in this review concerned the Ebola outbreak in West Africa, and most of the articles focused on the role of social media in the spread of misinformation. These findings may indicate two things. First, social media is increasingly playing the prime role in spreading health-related misinformation, as the use of social media has become ubiquitous and the influence of social media has risen to the extreme lately (Laranjo et al. 2015). As Ebola was one of the most recent large-scale, deadly and long-lasting outbreaks before COVID-19, coupled with the growing influence of social media, concern around misinformation regarding Ebola was discussed most often. Second was the relation of health and science literacy and lack of trust in governing bodies with the spread of misinformation (Chou et al. 2018). Ebola was mainly spread in West Africa, where studies showed that the low level of health, science and overall literacy, and a high level of distrust in the government were responsible for the spread of misinformation (Fowler et al. 2014; Gostin and Friedman 2015), factors confirmed by our study.
A proactive, solution-oriented approach that dissects the different levels of misinformation and how each arises is essential to developing feasible steps to overcoming misinformation. Wardle and Derakhshan (2017) discussed the three elements involved in the creation, production, distribution and reproduction of misinformation, namely agent, message and interpreter (Fig. 2). The results of our study can be approached using this model of misinformation to identify areas for intervention. We found that agents and interpreters during both the creation and production phases included family and friends, who are often perceived as a trusted source in the absence of authoritative sources (Balami and Meleh 2019; Bali et al. 2016; Boerner et al. 2013; Koralek et al. 2016; Vinck et al. 2019). During the creation phase, individuals or informal independent online users successfully create misinformation due to the lack of competing accurate information (Wardle and Derakhshan 2017; Kouzy et al. 2020). We found women, young people, and people with low levels of information were more prone to interpreting and passing on the misinformation that had been created (Adebimpe et al. 2015; Balami and Meleh 2019; Gidado et al. 2015; Klofstad et al. 2019). During the production phase, social networks, online forums and social media ascertain misinformation and construct it into a media product (Wardle and Derakhshan 2017), which was also reflected in 14 studies included in this review. A lack of consistent authoritative information contributes to uninformed decision-making, as trust in information becomes tied to personal experience (Wardle and Derakhshan 2017). During the distribution phase, sensationalistic or unclear mass media coverage of misinformation debates can expose the public to false claims (Wardle and Derakhshan 2017). Most of the studies in this review reported mass media as the main sources of information (Alqahtani et al. 2017); this, coupled with a lack of trust in government narratives and the disseminating power of social media, snowballs the distribution and reproduction of misinformation (Fig. 2).

Agents, messages and interpreters identified for the creation, production, distribution and reproduction of misinformation during large-scale infectious disease outbreaks
Conventionally, a single database is searched in a rapid review (Tricco et al. 2015); however, we also employed a grey literature database search to help expand and strengthen our search. Nevertheless, this review also has some limitations we need to acknowledge. The inclusion criteria may have been broad, but we felt this was necessary to capture literature on the different aspects of misinformation in outbreak scenarios adequately. Furthermore, in this review, we were unable to assess the quality of the literature, due to the variability in the type of records identified in the review.
This rapid review synthesizes knowledge about the different types of misinformation that prevail among the population during a large-scale infectious disease outbreak, how it originates and spreads, which individuals are most vulnerable to misinformation, and what factors potentiate the spread and impact of misinformation. This knowledge will help guide public health bodies, governments, researchers, media and other stakeholders to control the insidious effects of misinformation during the current COVID-19 pandemic and future disease outbreaks.
References
Abu-rish EY, Elayeh ER, Browning MJ (2019) Physicians’ knowledge, attitudes and practices towards Zika virus infection in Jordan. J Infect Dev Ctries 13:584–590. https://doi.org/10.3855/jidc.11356
Adebimpe WO, Adeyemi DH, Faremi A, Ojo JO, Efuntoye AE (2015) The relevance of the social networking media in Ebola virus disease prevention and control in southwestern Nigeria. Pan Afr Med J 22:7. https://doi.org/10.11694/pamj.supp.2015.22.1.6165
Albarracin D, Romer D, Jones C, Hall Jamieson K, Jamieson P (2018) Misleading claims about tobacco products in YouTube videos: experimental effects of misinformation on unhealthy attitudes. J Med Internet Res 20:e229. https://doi.org/10.2196/jmir.9959
Alqahtani AS, Rashid H, Basyouni MH, Alhawassi TM, BinDhim NF (2017) Public response to MERS-CoV in the Middle East: iPhone survey in six countries. J Infect Public Health 10:534–540. https://doi.org/10.1016/j.jiph.2016.11.015
Balami AD, Meleh HU (2019) Misinformation on salt water use among Nigerians during 2014 Ebola outbreak and the role of social media. Asian Pac J Trop Med 12:175–180. https://doi.org/10.4103/1995-7645.257118
Bali S, Stewart KA, Pate MA (2016) Long shadow of fear in an epidemic: Fearonomic effects of Ebola on the private sector in Nigeria. BMJ Glob Health 1:e000111. https://doi.org/10.1136/bmjgh-2016-000111
Boerner F, Keelan J, Winton L, Jardine C, Driedger SM (2013) Understanding the interplay of factors informing vaccination behavior in three Canadian provinces. Hum Vaccin Immunother 9:1477–1484. https://doi.org/10.4161/hv.24427
Bora K, Das D, Barman B, Borah P (2018) Are internet videos useful sources of information during global public health emergencies? A case study of YouTube videos during the 2015–16 Zika virus pandemic. Pathog Glob Health 112:320–328. https://doi.org/10.1080/20477724.2018.1507784
Broome ME (2000) Integrative literature reviews for the development of concepts. In concept development in nursing. In: Rogers BL, Knafi KA (eds) Concept development in nursing: foundations, techniques and application 2nd edn. Saunders, Philadelphia, pp 231–250
Buli BG, Mayigane LN, Oketta JF et al (2015) Misconceptions about Ebola seriously affect the prevention efforts: KAP related to Ebola prevention and treatment in Kouroussa prefecture, Guinea. Pan Afr Med J 22:11. https://doi.org/10.11694/pamj.supp.2015.22.1.6269
Carey JM, Chi V, Flynn DJ, Nyhan B, Zeitzoff T (2020) The effects of corrective information about disease epidemics and outbreaks: evidence from Zika and yellow fever in Brazil. Sci Adv 6:eaaw7449–eaaw7449. https://doi.org/10.1126/sciadv.aaw7449
Cheng VC-C, Wong S-C, Chuang VW-M et al (2020) The role of community-wide wearing of face mask for control of coronavirus disease 2019 (COVID-19) epidemic due to SARS-CoV-2. J Inf Secur 81:107–114. https://doi.org/10.1016/j.jinf.2020.04.024
Chew C, Eysenbach G (2010) Pandemics in the age of twitter: content analysis of tweets during the 2009 H1N1 outbreak. PLoS One 5:e14118. https://doi.org/10.1371/journal.pone.0014118
Chou W-YS, Oh A, Klein WMP (2018) Addressing health-related misinformation on social media. JAMA 320:2417. https://doi.org/10.1001/jama.2018.16865
Cinelli M, Quattrociocchi W, Galeazzi A et al (2020) The COVID-19 social media infodemic. Sci Rep 10:16598. https://doi.org/10.1038/s41598-020-73510-5
Cuan-Baltazar JY, Muñoz-Perez MJ, Robledo-Vega C, Pérez-Zepeda MF, Soto-Vega E (2020) Misinformation of COVID-19 on the internet: Infodemiology study. JMIR Public Health Surveill 6:e18444. https://doi.org/10.2196/18444
Dedrick A, Merten JW, Adams T et al (2020) A content analysis of Pinterest belly fat loss exercises: unrealistic expectations and misinformation. Am J Health Educ 51:328–337. https://doi.org/10.1080/19325037.2020.1795754
Ding H (2009) Rhetorics of alternative media in an emerging epidemic: SARS, censorship, and extra-institutional risk communication. Tech Commun Q 18:327–350. https://doi.org/10.1080/10572250903149548
Dubé E, Vivion M, MacDonald NE (2014) Vaccine hesitancy, vaccine refusal and the anti-vaccine movement: influence, impact and implications. Expert Rev Vaccines 14:99–117. https://doi.org/10.1586/14760584.2015.964212
Felter C (2020) Major epidemics of the modern era. Council on Foreign Relations. https://www.cfr.org/timeline/major-epidemics-modern-era. Accessed 13 Sep 2020
Fiscella K, Franks P, Clancy CM (1998) Skepticism toward medical care and health care utilization. Med Care 36:180–189. https://doi.org/10.1097/00005650-199802000-00007
Fowler RA, Fletcher T, Fischer WA et al (2014) Caring for critically ill patients with Ebola virus disease: perspectives from West Africa. Am J Respir Crit Care Med 190:733–737. https://doi.org/10.1164/rccm.201408-1514CP
Fung ICH, Fu KW, Chan CH et al (2016) Social media’s initial reaction to information and misinformation on ebola, august 2014: facts and rumors. Public Health Rep 131:461–473. https://doi.org/10.1177/003335491613100312
Ghenai A, Mejova Y (2017) Catching Zika fever: application of crowdsourcing and machine learning for tracking health misinformation on twitter. In: proceedings - 2017 IEEE international conference on healthcare informatics, ICHI 2017. IEEE, p 518. https://doi.org/10.1109/ICHI.2017.58
Gidado S, Oladimeji AM, Roberts AA et al (2015) Public knowledge, perception and source of information on Ebola virus disease – Lagos, Nigeria; september, 2014. PLoS Curr. https://doi.org/10.1371/currents.outbreaks.0b805cac244d700a47d6a3713ef2d6db
Gostin LO, Friedman EA (2015) A retrospective and prospective analysis of the west African Ebola virus disease epidemic: robust national health systems at the foundation and an empowered WHO at the apex. Lancet 385:1902–1909. https://doi.org/10.1016/S0140-6736(15)60644-4
Haddaway NR, Collins AM, Coughlin D, Kirk S (2015) The role of Google scholar in evidence reviews and its applicability to Grey literature searching. PLoS One 10:e0138237. https://doi.org/10.1371/journal.pone.0138237
Kanadiya MK, Sallar AM (2011) Preventive behaviors, beliefs, and anxieties in relation to the swine flu outbreak among college students aged 18–24 years. Z Gesundh Wiss 19:139–145. https://doi.org/10.1007/s10389-010-0373-3
Kasereka MC, Hawkes MT (2019) The cat that kills people:’ community beliefs about Ebola origins and implications for disease control in eastern Democratic Republic of the Congo. Pathog Glob Health 113:149–157. https://doi.org/10.1080/20477724.2019.1650227
Khangura S, Konnyu K, Cushman R, Grimshaw J, Moher D (2012) Evidence summaries: the evolution of a rapid review approach. Syst Rev 1:10. https://doi.org/10.1186/2046-4053-1-10
Khangura S, Polisena J, Clifford TJ, Farrah K, Kamel C (2014) Rapid review: an emerging approach to evidence synthesis in health technology assessment. Int J Technol Assess Health Care 30:20–27. https://doi.org/10.1017/S0266462313000664
Klofstad CA, Uscinski JE, Connolly JM, West JP (2019) What drives people to believe in Zika conspiracy theories? Palgrave Commun 5:36. https://doi.org/10.1057/s41599-019-0243-8
Koralek T, Runnerstrom MG, Brown BJ, Uchegbu C, Basta TB (2016) Lessons from Ebola: sources of outbreak information and the associated impact on UC Irvine and Ohio University College students. PLoS Curr. https://doi.org/10.1371/currents.outbreaks.f1f5c05c37a5ff8954f38646cfffc6a2
Kouzy R, Abi Jaoude J, Kraitem A, et al (2020) Coronavirus Goes viral: quantifying the COVID-19 misinformation epidemic on twitter. Cureus 12:e7255. https://doi.org/10.7759/cureus.7255
Kummervold PE, Schulz WS, Smout E, Fernandez-Luque L, Larson HJ (2017) Controversial Ebola vaccine trials in Ghana: a thematic analysis of critiques and rebuttals in digital news. BMC Public Health 17:642. https://doi.org/10.1186/s12889-017-4618-8
Laranjo L, Arguel A, Neves AL et al (2015) The influence of social networking sites on health behavior change: a systematic review and meta-analysis. J Am Med Inform Assoc 22:243–256. https://doi.org/10.1136/amiajnl-2014-002841
Lau JTF, Griffiths S, Choi KC, Tsui HY (2009) Widespread public misconception in the early phase of the H1N1 influenza epidemic. J Inf Secur 59:122–127. https://doi.org/10.1016/j.jinf.2009.06.004
Miller M, Banerjee T, Muppalla R, Romine W, Sheth A (2017) What are people tweeting about Zika? An exploratory study concerning its symptoms, treatment, transmission, and prevention. JMIR Public Health Surveill 3:e38. https://doi.org/10.2196/publichealth.7157
Naing C, Tan RYP, Soon WC, Parakh J, Sanggi SS (2012) Preventive behaviours towards influenza a(H1N1)pdm09 and factors associated with the intention to take influenza a(H1N1)pdm09 vaccination. J Infect Public Health 5:412–419. https://doi.org/10.1016/j.jiph.2012.07.005
Okan O, Bollweg TM, Berens EM et al (2020) Coronavirus-related health literacy: a cross-sectional study in adults during the COVID-19 infodemic in Germany. Int J Environ Res Public Health 17:1–20. https://doi.org/10.3390/ijerph17155503
Ortiz-Sánchez E, Velando-Soriano A, Pradas-Hernández L et al (2020) Analysis of the anti-vaccine movement in social networks: a systematic review. Int J Environ Res Public Health 17:1–11. https://doi.org/10.3390/ijerph17155394
Pennycook G, McPhetres J, Zhang Y, Lu JG, Rand DG (2020) Fighting COVID-19 misinformation on social media: experimental evidence for a scalable accuracy-nudge intervention. Psychol Sci 31:770–780. https://doi.org/10.1177/0956797620939054
Schmidt K, Ernst E (2004) Assessing websites on complementary and alternative medicine for cancer. Ann Oncol 15:733–742. https://doi.org/10.1093/annonc/mdh174
Seltzer EK, Jean NS, Kramer-Golinkoff E, Asch DA, Merchant RM (2015) The content of social media’s shared images about Ebola: a retrospective study. Public Health 129:1273–1277. https://doi.org/10.1016/j.puhe.2015.07.025
Sharma M, Yadav K, Yadav N, Ferdinand KC (2017) Zika virus pandemic—analysis of Facebook as a social media health information platform. Am J Infect Control 45:301–302. https://doi.org/10.1016/j.ajic.2016.08.022
Shigemura J, Harada N, Tanichi M et al (2015) Rumor-related and exclusive behavior coverage in internet news reports following the 2009 H1N1 influenza outbreak in Japan. Disaster Med Public Health Prep 9:459–463. https://doi.org/10.1017/dmp.2015.57
Smith TO (2010) A little birdie told me: H1N1 information and misinformation exchange on Twitter. UALR - William H Bowen School of Law Legal Studies Research Paper No. 11:03
Smith PS, Torsiglieri JA, Pasley J, Esch R (2016) Stopping an epidemic of misinformation : How K – 12 Science Teachers Responded to Ebola Technical Report. http://www.horizon-research.com/stopping-an-epidemic-of-misinformation-how-k-12-science-teachers-responded-to-ebola-technicalreport. Accessed 13 Sep 2020
Sommariva S, Vamos C, Mantzarlis A, Đào LU-L, Martinez Tyson D (2018) Spreading the (fake) news: exploring health messages on social media and the implications for health professionals using a case study. Am J Health Educ 49:246–255. https://doi.org/10.1080/19325037.2018.1473178
Song J, Song TM, Seo DC, Jin DL, Kim JS (2017) Social big data analysis of information spread and perceived infection risk during the 2015 Middle East respiratory syndrome outbreak in South Korea. Cyberpsychol Behav Soc Netw 20:22–29. https://doi.org/10.1089/cyber.2016.0126
Stanley ML, Barr N, Peters K, Seli P (2020) Analytic-thinking predicts hoax beliefs and helping behaviors in response to the COVID-19 pandemic. Think Reason. https://doi.org/10.1080/13546783.2020.1813806
Tai Z, Sun T (2011) The rumouring of SARS during the 2003 epidemic in China. Sociol Health Illn 33:677–693. https://doi.org/10.1111/j.1467-9566.2011.01329.x
Tosta E (2020) Transmission of severe acute respiratory syndrome coronavirus 2 through asymptomatic carriers and aerosols: a major public health challenge. Rev Soc Bras Med Trop 53:e20200669. https://doi.org/10.1590/0037-8682-0669-2020
Tricco AC, Antony J, Zarin W et al (2015) A scoping review of rapid review methods. BMC Med 13:224. https://doi.org/10.1186/s12916-015-0465-6
Van den Broucke S (2020) Why health promotion matters to the COVID-19 pandemic, and vice versa. Health Promot Int 35:181–186. https://doi.org/10.1093/heapro/daaa042
Vaska M, Chowdhury M, Naidu J, Baig K, Turin T (2019) Exploring all that is grey in the health sciences: what is grey literature and how to use it for comprehensive knowledge synthesis. J Natl Heart Foundation Bangladesh 8:14–19
Vinck P, Pham PN, Bindu KK, Bedford J, Nilles EJ (2019) Institutional trust and misinformation in the response to the 2018–19 Ebola outbreak in north Kivu, DR Congo: a population-based survey. Lancet Infect Dis 19:529–536. https://doi.org/10.1016/S1473-3099(19)30063-5
Wang Y, McKee M, Torbica A, Stuckler D (2019) Systematic literature review on the spread of health-related misinformation on social media. Soc Sci Med 240:112552. https://doi.org/10.1016/j.socscimed.2019.112552
Wardle C, Derakhshan H (2017) Information disorder: toward an interdisciplinary framework for research and policy making. Council of Europe. https://rm.coe.int/information-disorder-toward-an-interdisciplinary-framework-for-researc/168076277c. Accessed 13 Sep 2020
Whittemore R, Knafl K (2005) The integrative review: updated methodology. J Adv Nurs 52:546–553. https://doi.org/10.1111/j.1365-2648.2005.03621.x
Wilson K (2002) The desktop guide to complementary and alternative medicine: an evidence-based approach. Ann Intern Med 136:A14. https://doi.org/10.7326/acpjc-2002-136-3-a14
Wood MJ (2018) Propagating and debunking conspiracy theories on twitter during the 2015–2016 Zika virus outbreak. Cyberpsychol Behav Soc Netw 21:485–490. https://doi.org/10.1089/cyber.2017.0669
World Health Organization (2020) Munich Security Conference. https://www.who.int/dg/speeches/detail/munich-security-conference. Accessed 13 Sep 2020
Zarocostas J (2020) How to fight an infodemic. Lancet 395:676. https://doi.org/10.1016/S0140-6736(20)30461-X
Funding
No funding was received for conducting this study.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Developing search strategy, conducting literature search, data preparation, and analysis were performed by Nashit Chowdhury, Ayisha Khalid, and Tanvir C. Turin. The first draft of the manuscript was prepared by Nashit Chowdhury and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval
Not applicable.
Conflict of interest
The authors have no relevant conflict of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Chowdhury, N., Khalid, A. & Turin, T.C. Understanding misinformation infodemic during public health emergencies due to large-scale disease outbreaks: a rapid review. J Public Health (Berl.) 31, 553–573 (2023). https://doi.org/10.1007/s10389-021-01565-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10389-021-01565-3