
Abstract
The present study tracked the city-wide dynamics of severe acute respiratory syndrome-corona virus 2 ribonucleic acids (SARS-CoV-2 RNA) in the wastewater from nine different wastewater treatment plants (WWTPs) in Jaipur during the second wave of COVID-19 out-break in India. A total of 164 samples were collected weekly between February 19th and June 8th, 2021. SARS-CoV-2 was detected in 47.2% (52/110) influent samples and 37% (20/54) effluent samples. The increasing percentage of positive influent samples correlated with the city’s increasing active clinical cases during the second wave of COVID-19 in Jaipur. Furthermore, wastewater-based epidemiology (WBE) evidence clearly showed early detection of about 20 days (9/9 samples reported positive on April 20th, 2021) before the maximum cases and maximum deaths reported in the city on May 8th, 2021. The present study further observed the presence of SARS-CoV-2 RNA in treated effluents at the time window of maximum active cases in the city even after tertiary disinfection treatments of ultraviolet (UV) and chlorine (Cl2) disinfection. The average genome concentration in the effluents and removal efficacy of six commonly used treatments, activated sludge process + chlorine disinfection (ASP + Cl2), moving bed biofilm reactor (MBBR) with ultraviolet radiations disinfection (MBBR + UV), MBBR + chlorine (Cl2), sequencing batch reactor (SBR), and SBR + Cl2, were compared with removal efficacy of SBR + Cl2 (81.2%) > MBBR + UV (68.8%) > SBR (57.1%) > ASP (50%) > MBBR + Cl2 (36.4%). The study observed the trends and prevalence of four genes (E, RdRp, N, and ORF1ab gene) based on two different kits and found that prevalence of N > ORF1ab > RdRp > E gene suggested that the effective genome concentration should be calculated based on the presence/absence of multiple genes. Hence, it is imperative to say that using a combination of different detection genes (E, N, RdRp, & ORF1ab genes) increases the sensitivity in WBE.
Graphical abstract

Similar content being viewed by others

Introduction
An outbreak of pneumonia of unknown etiology was first reported in Wuhan (Hubei province, China) in late 2019, and the metagenomics sequencing shed light on the association of this outbreak with a novel coronavirus (nCoV) (Mehta et al., 2020). The “novel coronavirus-infected pneumonia” was officially designated as COVID-19 caused by severe acute respiratory syndrome-corona virus 2 (SARS-CoV-2) (Zhu et al., 2020; Gorbalenya et al., 2020). A total of 222,895,613 confirmed cases, including 4,602,961 deaths, were officially announced all over the world, by September 8th, 2021 (https://www.worldometers.info/coronavirus/), with distressing consequences on human health and economy, particularly in the USA, India, and Russia, among others (Johns Hopkins University and Medicine, 2021). The available epidemiological evidence strongly suggests that COVID-19 is primarily transmitted through respiratory droplets and contact routes (Rothan & Byrareddy, 2020). Tracing SARS-CoV-2 genetic material–viral RNA–in stool and urine of COVID-19 patients (Chen et al., 2020; Peng et al., 2020; Young et al., 2020) shed light on the pattern of spread of virus dissemination by aqueous matrices. The circulation of the virus was speculated to have occurred from malfunctioning sewage works (sewer networks and wastewater treatment plants (WWTPs)) in the community (Zaneti et al., 2021; Ahmed et al., 2020).
Recently, there grew a huge interest in the scientific community in shedding of virus into feces as well as the presence and persistence of SARS-CoV-2 in municipal effluents, although the potential of sewage to spread COVID-19 is extremely low and has not been reported to date (Ahmed et al., 2020; Medema et al., 2020). Both the World Health Organization (WHO) and the US Centers for Disease Control and Prevention (CDC) do not consider COVID-19 as water-borne and finding clues to support this claim throughout literature has not reached a clear conclusion (CDC, 2021). The presence of SARS-CoV-2 in wastewater indeed raises the potential for sewage analysis to inform epidemiological monitoring of COVID-19 as wastewater-based epidemiology (WBE). WBE is regarded as a complementary approach for current clinical surveillance which includes providing information on the prevalence and spread of disease in a population (Bivins et al., 2020). WBE based on raw wastewater fingerprinting to obtain qualitative and quantitative data within a given wastewater catchment not only provides an early warning sign for disease outbreaks but also acts as a smart way of imposing pre-emptive quarantine (Sims & Kasprzyk-Hordern, 2020).
For the last 1.5 years, several groups of researchers have been conducting different studies into sewage monitoring of SARS-CoV-2 with primarily two objectives. One is to detect the presence/surveillance of virus in a population for early epidemic prediction (SWEEP), and secondly, to assess infection risk to the public and sewage workers/operators from untreated/partially treated contaminated sewage and effluent as well as the air surrounding wastewater treatment facilities (Tiwari et al., 2021). WBE is a potential tool to complement the current clinical surveillance as an affordable, convenient, and practical program as it gives a time period of at least 7–28 days in advance for early preparedness by providing information on the prevalence and spread of disease in a population which helps decision and policymakers for proper allocation of resources (Sims et al., 2021).
Considerable efforts have been devoted to detecting SARS-CoV-2 in sewage in several countries, particularly in high- and upper-middle-income communities such as the Netherlands, Italy, and Spain where the sewerage systems are properly connected (Medema et al., 2020; La Rosa et al., 2020; Randazzo et al., 2020). However, the imbalance between the number of studies in developed countries and those on the broad spectrum of developing and resource-limited communities, especially India, indicates that much work has yet to be accomplished. Over 80% of wastewater is not connected to proper sewage networks and is discharged without treatment in India. The problem with India’s sewerage system is that it is fragmented and poorly connected. There is still a large percentage of the population that is not connected to any sewage treatment plants and sewerage infrastructure. The coverage of the sewerage system in Jaipur is less than that of the drainage system as it covers only 60–70% of the Jaipur municipal corporation area and caters to about 80% of the population.
There are very few case studies that have been reported from India, across the nation, including, i.e., Uttarakhand and Rajasthan from Northern India (Arora et al., 2020, 2021), Hyderabad (Hemalatha et al., 2021; Kopperi et al., 2021), and Chennai from Southern India (Chakraborty et al., 2021); and Gujarat (Kumar et al., 2020, 2021a, b, c) and Maharashtra from Central India (Sharma et al., 2021); most of which have successfully demonstrated the usefulness of WBE but on a limited scale. The awareness of WBE has been increasing during the COVID-19 pandemic; however, WBE is still not an established practice in low- and middle-income countries (LMICs) such as India. There are some challenges for an effective WBE implementation in India including a lack of awareness among the public health officials and government authorities, leaders of corporations, and the public. The implementation of a nationwide WBE program in countries like India with dissimilar sanitary coverage is an extremely complicated issue. The use of distinct sanitation systems, such as centralized sewer systems and on-site sanitation systems–pit latrines, bucket latrines, and septic tanks–imposes a challenge for WBE implementation in low- and middle-income countries. Viral RNA detection in dysfunctional sewer systems needs to be further explored (Gwenzi et al., 2021; Street et al., 2020). Therefore, it becomes even more imperative to validate this research in such systems to prove WBE as an efficient monitoring tool for early prediction.
Considering these limitations and challenges due to the fragmented sewerage system and the huge gap between generated versus treated sewage, this study aims to delineate how efficient can WBE be for predicting the upcoming surge of COVID-19 in Jaipur and whether such systems become a barrier in the successful application of WBE? To answer these pertinent questions, the present research study was planned from Indian perspectives to bridge the knowledge gap between researchers, the scientific community and government officials, and policymakers and to successfully implement WBE at a city scale that could possibly help in controlling the pandemic. Thus, the objectives of the present study were to (1) evaluate the implementation of WBE for Jaipur city, for prediction of the second wave of COVID-19; (2) determine the efficacy of different treatment systems in nine WWTPs in the removal of SARS-CoV-2 loads; (3) determine and validate the prevalence of different genes involved using the combination of two kits; and (4) standardizing the methodology including sample collection, transportation, and pre-processing in a cost-effective manner to establish WBE as an overall economical approach. Furthermore, the study will substantiate the potential of WBE for the city-wide surveillance in Jaipur city to incorporate WBE into the regular monitoring programs and policy framework to manage the future COVID-19 wave efficiently.
Experimental methodology
Wastewater sampling
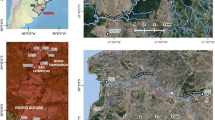
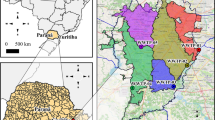
Influent and effluent samples were collected from nine municipal wastewater treatment plants (WWTPs) located across Jaipur city for the monitoring of the second wave of COVID-19. The influent samples have been analyzed for the prediction of the second wave while the analysis of effluent samples was done for evaluating the efficiency of the WWTPs for the removal of viral loads. This is a longitudinal study wherein the samples were taken between February 19th and June 8th, 2021. All the samples were collected as 1-L grab samples in sterile bottles and transported to the Environmental Biotechnology Laboratory at Dr. B. Lal Institute of Biotechnology, Jaipur, for further investigation and analysis. Appropriate precautions including ambient temperatures were taken into consideration for sample collection. Concerned personnel wore standard personal protective equipment (PPE) during the entire sampling process. The collected samples were transported to the laboratory at ambient temperatures of the city during the collection months, as adopted by (Arora et al., 2020, 2021). Figure 1 shows the geographical locations of the sampling sites used in the study.

Sampling sites of Jaipur for the study
Sample preparation
Figure 2 describes the methodology involved during the study. The samples for RNA isolation were prepared with slight modifications from the protocol described previously (Arora et al., 2020, 2021). The wastewater samples were surface sterilized using UV treatment for 30 min followed by manual mixing. Furthermore, 1-mL sample was aliquoted and centrifuged at 7000 rpm for 30 min (for removal of debris & unwanted materials) and the supernatant was then processed for RNA extraction as described in (Arora et al., 2021).

Methodology followed for processing the samples during the study
Viral RNA extraction
Viral RNA was extracted from the processed wastewater samples via the MagMAX Viral/Pathogen Nucleic Acid Isolation Kit (Applied Biosystems) following the manufacturer’s instructions using the automated KingFisher™ Flex machine. The protocol involves “three wash” steps for the extraction of the RNA. Samples were vortexed for 10 s and then mixed with the extraction buffer consisting of a binding solution, binding beads, and proteinase K (referred to as extraction master mix), vortexed for 30 s, and then processed using the automated system. This is followed by three washing steps using wash plate 1 consisting of wash buffer, wash plate 2, and 3 each consisting of varying amounts of 80% PCR grade ethanol. The RNA is finally eluted out and the process takes about 24 min each time. The eluted RNA in the plates is then sealed and stored at −20 °C till further use.
Qualitative and quantitative detection of SARS-CoV-2
The qualitative and quantitative presence of SARS-CoV-2 RNA was detected in the total RNA extracted from the wastewater samples using CFX 96 Thermal Cycler (Bio-Rad) RT-PCR machine using two separate commercially available kits. Kit 1 was Allplex™ 2019-nCoV Assay RT-PCR, used for the qualitative detection of SARS-CoV-2, consisted of 2019-nCoV MOM (prepared master mix), 5X Real-time One-step Buffer, Real-time One-step Enzyme, and exogenous Internal Control (IC). Kit 1 targeted the E gene, N gene, and RdRp gene with FAM and HEX as internal controls to be read on Cal Red 610 and Quasar 670 fluorophore channels, respectively. The PCR reaction was set up by mixing 11 μL of the isolated RNA with 14 μL of RT-PCR master mix. The reaction protocol consisted of 1 cycle at 50 °C for 20 min, 1 cycle at 95 °C for 15 min, followed by 45 cycles of denaturation at 94 °C for 15 s and combined annealing and extension for 30 s at 58 °C followed by plate read and detection. The PCR run was analyzed with Bio-Rad CFX Manager software version 3.1 (Bio-Rad Laboratories). As per the manufacturer’s instructions, the detection of a minimum of any two genes (out of three) in a sample was considered positive based on Ct values.
To further quantify the presence of SARS-CoV-2 viral genome in the wastewater samples, InnoDetect One Step COVID-19 (Kit 2) was used wherein two different plasmid DNA consisting of N gene and ORF1ab gene separately were used to prepare a standard curve (a range of 10 pg/μL to 0.01 fg/μL) as per the protocol in the manufacturer’s instructions. These standard curves were then used for the quantification of the respective genes in the samples. RNase-free water was used to make the main stock of concentration of 40 ng/μL. Kit 2 consists of a master mix, primer–probe (N gene, ORF1ab & RNaseP), and uses three fluorophore channels (HEX/VIC, FAM, & ROX/Texas Red, respectively) for individual identification. Viral RNA of SARS-CoV-2 was used as a positive control and DNase RNase-free water as a negative control provided with the kit. The reaction cycle consists of a reverse transcription step at 42 °C for 15 min 1 cycle, cDNA initial denaturation at 95 °C for 3 min 1 cycle, denaturation at 95 °C for 15 s, and combined annealing and extension at 60 °C for 40 s followed by plate read and detection. The samples with quantitative presence of any of the two genes (N or ORF1ab) or both the genes were considered positive.
Sensitivity of SARS-CoV-2 detection in wastewater
To determine the lower limit of detection of the assay kit used in this study, we established a standard curve with tenfold serial dilutions of 2019-nCoV DNA control from the RT-qPCR Kit, ranging from 1 × 106−1 copies/µL. An inverse linear relationship was generated against both of the target genes–N and ORF1ab. It was also interesting to note that even though the sensitivity of two quantitative probes seemed to be different, i.e., the limit of detection for N gene being log10 3 genome concentration/liter (GC/L) while that of ORF1ab being log10 4 GC/L.
Statistical analysis
The co-detection of genes using different kits and the removal efficiency due to different treatment approaches were visualized using R (ver. 3.31, http://www.R-project.org/). To evaluate the temporal effect, the viral concentration data (viral loads/positive detection rate) were paired with 7-day averaged new cases for Jaipur and India. A paired-sample T-test was carried out in order to evaluate the efficacy of ASP, MBBR, and SBR treatment processes while a comparison was made between influent and effluent wastewater samples of the treatment process. Pearson co-correlation coefficient tests were also carried out to understand the co-relations between active cases and influent loads/concentration.
Results
Characteristics of selected sampling sites for prediction and monitoring of the second wave of COVID-19
Similar to other tier-2 cities of India, Jaipur also has a fragmented sewerage network system with different centralized and decentralized wastewater treatment plants (WWTPs). The main objective of the present study was to determine whether a WBE-based early warning system can be established in such a fragmented system. Seven different sampling sites (site 1, 2, 3, 4, 5, 6, and 8) were selected across the whole length and two sites (site 7 and 9) were selected across the cross-section of the city; the details of which are described in Table 1. This ensured coverage of about 60–70% of the city population connected to the main sewerage trunk. Of the nine sites, one (site 4) was a system connected to an academic institution (Malaviya National Institute of Technology Jaipur (MNIT Jaipur)) connected with a residential capacity of 2000 inhabitants. Site 2, 3, 5, and 8 are small-sized decentralized systems that receive wastewater from multiple catchment areas and inhabit a population size of about 5000 individuals. Site 1 and 9 are medium-sized decentralized systems with a population size of greater than 50,000 individuals while sites 6 and 7 are large centralized systems with a population size of about 5 Lakhs (official data obtained from Jaipur Development Authority (JDA), & National Institute of Urban Affairs (NIUA) report 2021). For an efficient WBE application in lower- and middle-income countries (LMICs) such as India, surveillance and selection of sampling sites were done to best represent the maximum coverage of the city’s sewer system connected to the catchment area and covers the maximum population of the city. Also, the selection of WWTPs was also done to have variable factors for research in the study such as different sizes/capacity of WWTPs and different treatment types.
Grab composite samples were collected every week during the entire duration of the study. Samples were collected from the sites located at the center towards the sites upstream or downstream across the sewage trunk line. As a result, samples of the sites closer to the center were collected around 11 AM while those of the sites at the terminal were collected around late afternoon at 1 PM. Wastewater sample collection from WWTPs, its transportation to the experimental laboratory, and pre-processing before RNA extraction is a challenge in terms of both logistic feasibility and for the applicability of WBE at a city scale. Our previous studies (Arora et al., 2021) have already reported that direct RNA extraction (without pre-processing) from 1-mL centrifuged supernatant of the properly mixed 1 L collected wastewater sample is sufficient enough for the detection of SARS-CoV-2. As a result, a similar protocol was used in this study.
Qualitative and quantitative detection of SARS-CoV-2 in the influent samples of WWTPs with monthly variations and correlation with the active cases in the city
In the present study, we reported weekly data of wastewater samples collected from nine different locations for sixteen weeks from February to June 2021, and the results are mapped in the heat map as shown in Fig. 3. The average Ct values for E, RdRp, N, and ORF 1ab genes were 32.3, 35.1, 33.4, and 34.7, respectively. Likewise, the average Ct value of internal control (MS2 bacteriophage) was 27.3, and no SARS-CoV-2 genes were detected in the negative control samples. We detected and quantified monthly variations in SARS-CoV-2 RNA from wastewater samples to understand the pandemic situation during the second wave in Jaipur, Rajasthan (India). The longitudinal analysis of the wastewater samples collected from the nine sites showed the first detection of SARS-CoV-2 as early as 27th February 2021 as evident from Fig. 3. The percentage prevalence of positive influent samples to the total samples collected showed 44.4% positivity on 19th March 2021 when the new active case number per day was only 61. The percentage positivity then increased to almost 100% from 26th March 2021 and continued till 15th May 2021 before declining. This is also in agreement with the fact that the increasing prevalence of percentage positive influent wastewater samples correlated well with the increasing cases and deaths reported during the second wave of COVID-19 in Jaipur. The noticeable increase in the case number, viz., 528 per day appeared on 5th April 2021 which is 2 weeks post the significant number of positive wastewater samples (on 26th March 2021). So, this time period of 2 weeks could be sufficiently utilized to control the ever-increasing cases and deaths, in the city. This can also be correlated with the number of deaths due to COVID-19 in this duration wherein the 7-day moving death average was around 1 on 1st April which increased to 55.57 on 8th May 2021 (peak of COVID-19). The restricted movement was imposed in the city on 17th April 2021 when the new active case number had already reached 1484 per day, which rose to a maximum of 4202 on 7th May 2021 (as per official data from www.covid-19india.org). Additionally, lag correlation analysis was performed for three different time intervals, viz., 7 days, 14 days, and 21 days. Both the new active cases on the day as well as 7th-day average were analyzed for the same. The Pearson correlation coefficient values for the three-time intervals v’s daily new cases and the 7-day average are depicted in Table 2. The results for all the three-time intervals clearly showed that the 7-day average proves to be a better measure than the daily new active cases. The Pearson correlation coefficient for the three-time intervals suggested a 21-day lag to be the best predictor of the spread of COVID-19 infections. The current study of the WBE or wastewater surveillance provides population-scale information for the detection of the hotspot, measure the scope of the outbreak, provide stakeholders with a decision platform, understand the impact of the demand in the health sector, track infection and measures, and provide an early warning for re-emergence of the pandemic outbreak, thus helps in better pandemic management of COVID-19.

Heat map showing temporal variation in the positive prevalence of the SARS-CoV-2-targeted genes in influent samples at various locations in Jaipur city with increasing active cases and deaths reported (green N negative, pink P positive, NA not applicable)
The quantitative analysis of all the influent samples was also carried out wherein the genome copy number of the N gene and ORF1ab gene was calculated. As observed in Fig. 4, during the months of February, the average genome concentration was log10 4.40 GC/liter which increased to log10 4.58 in March and to log10 5.43 and 5.47 in April and May, respectively. The increasing genome concentration correlated well with the increasing number of active cases and mortality rate. Figure 4 also shows the detection of the N gene as early as 27th February 2021 coinciding with the qualitative analysis while the ORF1ab gene was first detected on 26th March 2021. Thus, the N gene could be detected 20 days prior to the significant rise in the new active patients per day while ORF1ab was detected 10 days prior. It is worth noting that the genome copies of both the genes were quantifiable in the wastewater samples throughout the second wave. Another interesting observation to note here is that although the N gene could be detected earlier during the rise of the cases, it was the ORF1ab gene that could be detected and quantified when the patient case numbers declined while the detection of the N gene had already reached below the limit of detection (LOD). The SARS-CoV2 RNA concentrations in the wastewater influent samples calculated from the N gene ranged from 4.4 to 6.04 log10 GC/L and ORF1ab ranged from 4.5–5.60 log10 GC/L (n = 110). Normalized viral loads of quantifiable wastewater influent samples from WWTPs were plotted and compared with new cases from Jaipur city and India (Fig. 4).

Analysis of SARS-CoV-2 concentration week wise with daily COVID-19 cases and deaths reported in Jaipur and India (LOD limit of detection)
Prevalence of genes targeted for SARS-CoV-2 detection
Owing to the low sensitivity of the RT-PCR kits towards wastewater samples, two different kits consisting of five different probes were used for the study to ensure accurate detection. As already described in the “Experimental methodology” section, four different genes (N, RdRp, E, and ORF1ab) were analyzed where RdRp and E genes were detected qualitatively, ORF1ab was detected quantitatively, and N gene was detected both qualitatively and quantitatively using two different probes. Figure 5 describes the prevalence and co-prevalence of four genes in both the samples (influent and effluent). Out of the 164 total wastewater samples tested, all the four target genes could be detected in only 15 wastewater samples whereas, in other samples, genes were detected in different combinations. N gene was the most commonly detected gene in the samples wherein 33 samples tested positive for only one of the N gene targets (N detected by either or both probes from Kits 1 and 2) followed by 5, 8, and 12 samples in combination with E, RdRp, and ORF1ab genes, respectively. Furthermore, one sample each consists of positive targets of only ORF1ab or only RdRp genes. However, interestingly, the E gene showed the highest number of false positives and was never detected alone. Similarly, 16 and 7 samples were found positive for a combination of N, RdRp, and E gene, or of ORF1ab, N, and E genes, respectively.

Positive detections using two kits with different genes (i.e., E, N, RdRp, ORF1ab) of all samples (both influent and effluent). The red triangle indicates positive samples identified based on the criteria. The blue and green bars indicate the false-negative identified by Kit 1, and Kit 2, respectively
Among the 164 wastewater samples analyzed in the study, only 52 samples (30.5%) could be confirmed by both kits. However, the total number of wastewater samples that could be ruled positive by either of the kit target criteria was 72. The difference of 69.5% positive prevalence in samples was reported using a combination of 2 kits. It is also observed that six samples were detected positive qualitatively, i.e., showed any two out of three genes positive using Kit 1 (including N gene) but could not be quantified by Kit 2. This could be attributed to the variation in the probe used for detection, sensitivity, and the detection limits of the two kits. In addition, 16 samples which were considered negative during the qualitative detection by Kit 1 (as per manufacturer’s criteria) were detected positive by Kit 2 (either N gene or ORF1ab gene or both present). These observations thus support the use of a combination of kits to achieve a finer distinction and broader detection of the SARS-CoV-2 genome when compared to detection by a single kit. Hence, it is imperative to say that wastewater surveillance-based data must not be validated based on a single particular gene of SARS-CoV-2 but its effective gene concentration including multiple genes.
Efficacy of WWTPs in the removal of SARS-CoV-2
The efficacy of the WWTPs in the removal of SARS-CoV-2 from the wastewater samples was observed in our earlier study during the first wave of COVID-19 (Arora et al., 2020, 2021). However, in the present study, it was observed that the efficacy of the WWTPs was compromised wherein the virus load could be detected in the effluent samples as well. Due to limitations (mainly permissions or breakdown of WWTP), in sample collection, the effluent samples from site 9 were not considered for analysis. Figure 5 summarizes the positive prevalence and the efficacy of different treatment technologies in the removal of SARS-CoV-2 in the samples. It was observed that during March, an average of only 20% of effluents samples were positive, which increased to 43.2% in April, and 55% in May. It was observed that this percentage can be correlated with the high active case-loads in the city, (between 9th April 2021 and 24th May 2021 as per www.COVID-19.org) which makes it difficult for WWTPS to remove SARS-CoV-2. The removal efficacy of different treatment technologies was also compared in terms of qualitative detection. Paired t-tests between the influent and effluent wastewater samples, taken on the same days, were performed to understand the significance of the SARS-CoV-2 gene removal efficacy of each treatment process, i.e., activated sludge treatment ASP + Cl2, moving bed biofilm reactor (MBBR) with ultraviolet radiations (UV), MBBR + chlorine (Cl2), sequencing batch reactor (SBR), and SBR + Cl2 (Fig. 6). Overall comparison of SARS-CoV-2 genome removal efficacy of different treatments is expressed on the total positive prevalence obtained throughout the monitoring. The significance of SARS-CoV-2 genes removal efficacy in different treatment technologies includes the order of SBR + Cl2 (81.2%) > MBBR + UV (68.8%) > SBR (57.1%) > ASP (50%) > MBBR + Cl2 (36.4%). We examined the efficiency of MBBR, SBR, and ASP wastewater treatment processes before and after the treatment wastewater samples (i.e., influent and effluent). A paired-sample T-test was carried out in order to evaluate the efficacy of treatment processes, while a comparison was made between influent and effluent wastewater samples of the treatment process. The results showed significant removal of all three targeted SARS-CoV-2 genes from the MBBR plant (p < 0.05), while a substantial decrease (p < 0.05) in E and N genes was noticed in the SBR treatment process depicted by a post-treatment increase in Ct values of genes. Likewise, all three genes were successfully removed from the ASP treatment process. In addition to this, the paired T-test between the inlet and outlet wastewater samples, taken on the same date during the study, displayed a significant reduction/removal of SARS-CoV-2 genes. Contrary to this, the reduction of SARS-CoV-2 genes in wastewater samples was insignificant in the SBR treatment process. The results suggest that all three treatment processes successfully reduced/removed the virus genetic load in wastewater samples; however, the performance of MBBR was found to be higher than that of the SBR and ASP treatment processes.

Temporal variation in gene copies of the SARS-CoV-2 targeted genes and effective gene concentration in Effluent samples at various locations in Jaipur city with removal efficacy of different treatments (P positive result, N negative result, NA not applicable)
The removal efficacy of the WWTPs was also analyzed by comparing the viral genome load in terms of quantitative analysis of N gene and ORF1ab gene, respectively, in the influent and the effluent samples. Figure 7 shows the box plots of different treatment types using the N gene and ORF1ab gene, respectively. These results suggested that in the case of the sites like sites 4 and 5 once the genome load in the influent samples exceeded the log of five, effluent loads were in the median range of 5 logs for both genes irrespective of the loads observed in corresponding effluent grabs which fluctuated between logs of 4 to 6.

Box plot indicating removal efficiency of SARS-CoV-2 RNA in wastewater in 5 different treatments systems at WWTPs using (a) N gene and (b) ORF1ab gene. Only the WWTP with no less than 2 data points for the removal efficiency is included in the figure
Discussions
Sampling from fragmented and selected areas of a city can successfully be harnessed into a prediction model
WBE has been evaluated as a potential tool for the prediction of the COVID-19 pandemic across various sections of the world (Fongaro et al., 2021; Ahmed et al., 2020). However, those studies have been carried out either based on a small scale in developing countries (such as in studies of Kumar et al., 2020, 2021a, b, c) or within a city with a highly connected sewer network in developed countries. The wastewater systems in the majority of Indian urban cities are fragmented and composed of various decentralized treatment plants scattered throughout the city confines. The rural and slum areas and outskirts of these urban areas have practically a non-existent WWTP and thus most of the wastewater is dumped either in surface water bodies like rivers or in the community-wide septic tanks. Given the fragmented state of the sanitation network, a mere ability to detect pathogens or biomarkers in wastewater is not sufficient. This detection needs to be carried out in a systematic, regular, and planned manner to monitor the community uniformly and warn the same well in advance about any potential threats. There is an urgent need for time-series data of SARS-CoV-2 RNA concentration in the wastewater that can be matched with the actual clinical survey data to confirm the utility and predictability of wastewater surveillance in India. This is also imperative for the adaptation of the Surveillance of Wastewater for Early Epidemic Prediction (SWEEP) on the policy level. This becomes more important in India since the development of a proper and integrated wastewater treatment system is far-fetched even in the urban areas considering the overall limitations. Therefore, the present study aimed to investigate the applicability of WBE in the prediction and monitoring of COVID-19 waves in a city-level paradigm with a limited interconnected sewerage system. Despite the presence of disconnected and fragmented WWTPs, undergoing the treatment of only 60–70% of the total wastewater generated, the collection sites were selected such that they covered most of the total WWTPs installed in the city. A combination of small and medium decentralized WWTPs and large centralized treatment plants was selected to investigate in detail the ability and feasibility of WBE to detect the upcoming COVID-19 active caseload rise in advance. As mentioned in results the “Characteristics of selected sampling sites for prediction and monitoring of the second wave of COVID-19” section, it was observed that even with such a restricted coverage, the increase in positivity from various sites could be observed at least 14–20 days (at a total active case count of less than 50 per day) before a visible rise in newly detected active cases. Another important observation to be made in this case study is that in contrast to Kumar et al. (2021a), this study shows that if the sites are selected carefully, it is possible to directly correlate the positivity rate of the sites to the upcoming wave in advance. As is the case in point where this study was able to predict the upcoming wave of COVID-19 in Jaipur city, well in advance of 14–20 days (on 5th April 2020) while the cases started increasing exponentially after 20th April, with peak maximum cases load on 8th May 2021. Overall, it can be highlighted that even in Indian sewage system networks rudimentary as they might be, WBE can be either directly (as observed here) or at least indirectly can be applied for early predictions (Kumar et al., 2021a). Similar to the temporal variations in copy number reported in a previous study by Kumar et al. (2021a), an exact trend of copy number could not be established; however, it was observed that the general positivity rates observed in this study could be correlated with the rise of caseloads in the city. Thus, it may seem that in a carefully monitored city, just qualitative detection might be enough in raising a rudimentary alarm for the city officials.
Another interesting observation was in contrast to the previously published reports which suggest that WBE detection of SARS-CoV-2 genomes outlasts the clinical detection and falls slowly (Nemudryi et al., 2020); this study reported a sharp decline in positive prevalence rate (Figs. 2 and 3) in the wastewater samples with the fall in cases. Within 2–3 weeks of COVID-19 s wave peak, the positive prevalence rate dropped to 50% (4/8) and 8% (1/9) in samples collected after 20th May 2020. This contrast is interesting and needs to be further investigated. One of the possible explanations for this observation may be the limited sampling from selected collection points. Another explanation of this observation may be the symptoms present in the passing wave where coughing subsides contributing to a decreased ratio of sputum to fecal viral load. However, more investigation is needed in this direction, and in absence of a certain load-to-case number conversion metric, this observation might not be completely explained.
A combination of kits with multiple target probes has a large coverage and detection sensitivity
The premise of using WBE successfully in community-wide surveillance of a disease or a biomarker is the shedding of respective pathogens or certain specific molecules into the wastewater (Weidhaas et al., 2021). SARS-CoV-2 is known to be shed in wastewater through the body excreta of an infected individual regardless of the manifested symptoms. Although several targets for detection of such diseases are available, several factors contribute to the efficiency of the method such as the sensitivity of a detection primer–probe combination or any inhibiting factor present in each test sample. Therefore, it can be argued that relying on only one type of target or probe may lead to false-negative or positive detection. Since timely detection of the target is essential for the management of the disease in the community, the percentage efficacy of two different kits was compared. To surveil and continuously monitor the presence of the viral particles, already available and Indian Council of Medical Research (ICMR) approved kits were used as a part of investigating the uniform up-scalement of the city-wide surveillance. As described previously, Kit 1 was Allplex™ 2019-nCoV Assay RT-PCR kit, used for the qualitative detection of SARS-CoV-2 (for E, N, and RdRP genes) and Kit 2 was InnoDetect One Step COVID-19 kit used for quantitative detection (for N and ORF1ab gene). The set of targets consisted of both structural (N, E) and non-structural (RdRp and ORF1ab) genes ((Naqvi et al., 2020). Out of the total collected 164 samples, 148 samples were confirmed positive by kit 1 which could also be quantified by kit 2. However, 16 samples were confirmed positive only based on the 2 kits used. Interestingly, only 30.48% (50 out of 164) of the positive samples could be detected by both the kits while 12.8% (21 out of 164) of the samples were additionally identified by either Kit 1 or Kit 2 alone.
It was also observed that most of the samples uniquely detected by Kit 1 were collected from a site connecting to centralized wastewater treatment plants (sites 7 and 8) while all the samples which could only be detected by Kit 2 were from decentralized systems (sites 1, 3, and 5). The sites which show sample variability between the detection by Kit 1 versus Kit 2 operate at a different scale and collect over different sizes of the catchment area. Thus, the variability in detection could be because of the differential sensitivity of the primer–probe set used in Kit 1 and 2. Or it could be due to the difference in silt or contaminant levels accumulated during the collection of wastewaters in larger catchments between the origin and the centralized treatment plants. Furthermore, the sites which could be ruled positive only by Kit 2 were tested positive for at least one of the three target genes of Kit 1 but were ruled negative as per the Kit 1 criteria. Therefore, it can be inferred that using additional detection probes might be required to determine any false-negative results obtained with a single kit. While such factors will always be a consideration in the WBE approach and can only be resolved by upgrading the detection infrastructure, using more than one kit seems to increase the coverage of detection by 13% approximately which becomes more relevant as the increase in the number of samples becomes larger. It is worth highlighting that gene N, while could be detected by the Kit 1 probe very efficiently, did have a couple of instances of only being detected by the probe from Kit 2 only indicating the benefits of the multiple target approach.
It is interesting to note that not all the target genes could be detected uniformly or independently in all the samples analyzed. This observation further highlights the need for the analysis of multiple targets while surveilling pathogen presence in a given community. In addition to the use of multiple targets for detection, the criteria for considering a sample positive in terms of wastewater also need to be revisited owing to the dilution of the virus particle and/or genes in the wastewater samples or the presence of various inhibitors. The current study for instance has followed the ICMR approved criteria of detecting two out of three targets for a sample to be positive by Kit 1. However, it is worth noting that these criteria were first approved for testing in patients directly and might not be as applicable to the wastewater sample where the presence of a single gene (with Ct values below the detection cut-off of 40) might indicate a very low presence of circulating pathogens in the community. Such observations should be worth a second look as even though it is possible that they are false positives, an alternative scenario where the detection of a spread is inhibited by some community-specific factors which might be present in the wastewater samples. Standardizing a way therefore where the validity of the presence of one single target out of many may provide a more sensitive application of WBE in containing a large-scale spread.
Quantification by two different target probes could cover the complete second wave in the city
It was also interesting to note that even though the sensitivity of two quantitative probes seemed to be different (limit of detection for N gene being log103 genome concentration/liter (GC/L) while that of ORF1ab being log 104 GC/L) (Fig. 4), both the genes could be quantified throughout the study period. Although a more sensitive detection method like droplet PCRs in combination with integrated wastewater-based monitoring is ideal for monitoring at the city level, this study has tried to investigate the success of WBE monitoring on the existing current wastewater treatment facilities in the city using simple qPCR-based detection. It was observed that with weekly monitoring across the selected few sites in the city of Jaipur (9 sites spread across the city 7 longitudinally and 2 cross-sectionally), the data of sites’ sample positivity could be correlated with a rise in active case rate approximately 14–20 days in advance. This observation has great implications in the context of countries like India where dense population per unit area and minimal individual testing facilities are real limitations. Indeed, the lack of applications like wastewater-based epidemiology predictions in city-wide pandemic management was painfully apparent during the second wave of COVID-19 in Jaipur. The study clearly hypothesizes that with the appropriate individual testing and smart lockdown strategy including micro-containment zone formation based on WBE prediction observations, unnecessary loss of many lives could have been saved along with reduced burden on the healthcare sector by proper management of the resources leading to reduced mortality and morbidity rate.
High SARS-CoV-2 loading led to incomplete removal in WWTPs
It is well known that these WWTPs are designed as per certain design parameters and criteria and work on the specified limited capacity. During the first wave of COVID-19 in Jaipur, it was observed that the treatment technologies available at different WWTPs in the city were sufficient in the removal of the SARS-CoV-2 genome from the effluents and none of the effluent samples in the 14 WWTPs was detected positive by qualitative assays (Arora et al., 2021). However, during the second wave, it was observed that 37% (20/54) of effluent samples were tested positive for the target genes both by qualitative and quantitative assays. This observation can be explained by several factors. Firstly, during the early phase of COVID-19 infections in 2020, the samples were collected during the months of May–July when the number of daily confirmed cases was in the range of 40–45 cases per day, while during the second wave in the city, the daily confirmed case numbers were as high as 4202 (on May 8, 2021) which is approximately 100 times higher. Thus, it can be extrapolated that the shear load of viral particles shed in the wastewater has increased significantly and possibly even higher than the working capacities of the treatment plants. This suggests a clear correlation between increased load in influent and RNA decay efficiency. The duration of the effluent sample collection corresponds to the months (April & May 2021) of the maximum patient caseload in the city. Secondly, it was also observed that upon exceeding a load of log10 5 log genome copies (GC)/liter in the influent, quantification of either of the genes was irrespective of the influent loads. This is an interesting observation in terms of RNA decay efficiency as well as retention. Thus, (a) it is possible that during the peak phase of the second wave, the wastewater treatment systems were exceedingly overloaded with the viral genome that they simply failed in complete removal of the viral RNA fragments; (b) the uniform quantities of gene loads within their median load indicate that there is steady retention of the genomic fragments in the treatment system reaching saturation under high viral load; or (c) the difference in two of the tertiary-treated samples in case of the existence of the second mechanism is that it would be interesting to find out which component of treatment might promote this retention and is there any possibility that viral particles can be viable for a prolonged duration in these pretended fractions. Furthermore, it is important to understand that the size of the treatment plant and operational and management consistencies, along with the quality of influent water, will play a critical role in understanding in-depth the entire research scenario of COVID-19 transmission and monitoring.
Furthermore, it is imperative to understand that sample collection was done from three different secondary treatment technologies, viz., ASP, MBBR, and SBR and followed by two tertiary disinfection processes (UV and chlorine) and still found the genetic fragments of SARS-CoV-2 in the effluent. This observation may imply that owing to the nano-sized colloidal nature of genetic fragments, disinfection processes like chlorination/UV are likely to be less effective than the process of coagulation as reported in Kumar et al. (2021a). In our study, all the different treatment processes are found to effectively remove SARS-CoV-2 RNA with varying efficacy. To the best of our knowledge, this is the first report assessing the effectiveness of five different treatment schemes for SARS-CoV-2 RNA reduction. As far as treatment type is concerned, the SBR + chlorine showed better efficacy of 81.2%, followed by MBBR + UV with 68.8%, followed by SBR, MBBR + chlorine, and ASP. These findings indicate that secondary wastewater treatment may contribute to reducing the virus concentration in wastewater owing to the adverse environmental conditions that the virus encounters, such as temperature, pH, solids, micropollutants, and because of virus sorption to organic particles and further elimination by settling in ASP. Further virus removal can be achieved by MBBR & SBR due to (i) natural decay under unfavorable conditions (solids, microorganisms, temperature) for relatively long hydraulic retention times and (ii) processes of sedimentation, filtration, predation, and adsorption, but removal is largely variable and thus disinfection has an important role to enhance the level of virus inactivation in WWTPs. There is a general agreement that tertiary treatments are effective in the elimination of SARS-CoV-2 from the water lines (Randazzo et al., 2020). Specifically, chlorination and UV have been previously determined as an effective treatment for the elimination of SARS-CoV-2 (Abu Ali et al., 2020).
However, the detection and quantification of SARS-CoV-2RNA in wastewater do not imply viable viruses; it is highly recommended to validate on the infectivity/viability of SARS-CoV-2 after the treatment. However, it is worth considering here that effective aerobic WWTPs may not be sufficient to completely remove the genetic fragments of SARS-CoV-2.
Relevance of standardizing the WBE protocols and guidelines for pandemic management in a city like Jaipur
As mentioned above, the application of WBE in the surveillance and monitoring of physiological and pathogenic trace markers has attained a lot of attention in countries with fully developed and integrated wastewater treatment systems during the COVID-19 pandemic. However, more research is required before this model can be adopted at a city-wide or national level, beyond the pandemic era, particularly in developing countries. In India, these applications are even further from application owing to the limitations faced by underdeveloped wastewater treatment systems.
First, despite being a cost-effective measure to complement the individual testing, the state of the current sanitation network is thought of as a major challenge. In this context, establishing sophisticated sewerage systems will become an expensive step. This glaring gap, along with the consequent lack of awareness in policymakers of India has led to a nationwide reluctance in developing WBE methods in India. This study thus provides the example of the successful application of WBE in Jaipur, a city with a fragmented sewerage system. Even if it is possible to detect an upcoming wave as early as 14–20 days, various requirements as per the internationally established protocols previously reported by other groups, e.g., size of sample collected, cold chain transportation, facilities of ultrafiltration setups, ultracentrifugation, and sophisticated detection instruments like droplet PCR, still need to be established.
The focus of this study was to apply the procedure developed in the lab-scale to the city surveillance. Therefore, the feasibility of using these steps over a full wave of SARS-CoV-2 surge in the city was analyzed. The advantages of the method used here include less time consuming, lesser number of steps, and very less equipment requirements. For example, the prediction could be done successfully with randomly taking just 1 mL volume from 1-L grab samples indicating that there is no need for large collection volume saving the transportation cost. Also, these samples were collected and transported to the laboratory at the ambient city temperatures (non-refrigerated vehicles, duration between collection and storage at 4 degrees was a maximum of 3.5 h) for same-day RNA isolation and qualitative detection suggesting cheaper sample collection and storage on a city level. Along with the observations of (Arora et al., 2021), this collection model can be extended to remote locations where facilities of RNA extraction and detection might not be established. Therefore, instead of establishing and maintaining testing centers in every small village, gated community, or town, the collected sample can simply be transported to a centralized testing center under cold chain transport for detection and monitoring on a regular basis. The protocol for sample pre-processing is simple and can be completed by using even low-speed centrifuges. Thus, the procedure reported in this study has been shown to be working perfectly on city-scale weekly monitoring and can be applied to scale up even harnessing in the moderately equipped cities with centrally equipped detection centers. Thus, WBE has been successfully proven for early hotspot prediction which will help public health authorities and the government to take suitable measures, and optimize the resource efficiently for better pandemic management of COVID-19.
Conclusions
Wastewater surveillance is a promising tool that detects real-time and early disease signals and determines emerging hotspots in the surveillance of COVID-19 prevalence at the community level. Yet, in India, the city-scale surveillance of SARS-CoV-2 RNA in wastewater remains poorly understood and needs to be explored, especially in cities with fragmented sewerage systems. A temporal variation of SARS-CoV-2 RNA presence in wastewater was studied for a period of five months in Jaipur, India. This study reported the first successful SARS-CoV-2 WBE application in 9 wastewater systems in Jaipur (n = 164) with varying sizes, which serve 60–70% of Jaipur’s sewerage network. Interestingly, the positive detection rates of SARS-CoV-2 RNA in the wastewater from all the WWTPs increased along with the clinical cases over time. A total of 72 samples (43.9%) of the total 164 samples tested in the study were found to be positive, with at least two positive RT-PCR results targeting four SARS-CoV-2 genes such as E, RdRp, N, and ORF1ab gene. This system of wastewater-based epidemiology is extremely essential in practice in an Indian context where the resources are lacking in terms of both disease management and diagnosis. As demonstrated by this study, a gap of 14–20 days warning could be sufficient to take necessary actions to stop the spread of the next COVID-19 wave. This finding was further supported by the relation between the percentage change in effective gene concentration level and confirmed cases, which followed a similar trend on the temporal scale with a ~ 1 to 2 weeks’ time distance. The study has successfully proven the global implications of WBE for India, highlighting the role of WBE through the application of scalable and cost-effective protocol reported in the study for societal benefit and third wave improved management.
Data availability statement
All data generated or analyzed during this study are included in this published article and additional dataset generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Abu Ali, H., Yaniv, K., Bar-Zeev, E., Chaudhury, S., Shaga, M., Ronen, Z., Kushmaro, A., & Nir, O. (2020). Tracking SARS-CoV-2 RNA through the wastewater 1 treatment process. medRxiv. 2020.10.14.20212837.
Ahmed, W., Angel, N., Edson, J., Bibby, K., Bivins, A., O’Brien, J. W., Choi, P. M., Kitajima, M., Simpson, S. L., Li, J., & Tscharke, B. (2020). First confirmed detection of SARS-CoV-2 in untreated wastewater in Australia: A proof of concept for the wastewater surveillance of COVID-19 in the community. Science of the Total Environment, 728, 138764.
Arora, S., Nag, A., Sethi, J., Rajvanshi, J., Saxena, S., Shrivastava, S. K., & Gupta, A. B. (2020). Sewage surveillance for the presence of SARS-CoV-2 genome as a useful wastewater-based epidemiology (WBE) tracking tool in India. Water Science and Technology, 82(12), 2823–2836.
Arora, S., Nag, A., Rajpal, A., Tyagi, V. K., Tiwari, S. B., Sethi, J., Sutaria, D., Rajvanshi, J., Saxena, S., Shrivastava, S. K., & Srivastava, V. (2021). Imprints of lockdown and treatment processes on the wastewater surveillance of SARS-CoV-2: A curious case of fourteen plants in Northern India. Water, 13(16), 2265.
Bivins, A., Greaves, J., Fischer, R., Yinda, K. C., Ahmed, W., Kitajima, M., Munster, V. J., & Bibby, K. (2020). Persistence of SARS-CoV-2 in water and wastewater. Environmental Science & Technology Letters, 7(12), 937–942.
Chakraborty, P., Pasupuleti, M., Shankar, M. J., Bharat, G. K., Krishnasamy, S., Dasgupta, S. C., Sarkar, S. K., & Jones, K. C. (2021). First surveillance of SARS-CoV-2 and organic tracers in community wastewater during post lockdown in Chennai, South India: Methods, occurrence and concurrence. Science of the Total Environment, 778, 146252.
Chen, Y., Chen, L., Deng, Q., Zhang, G., Wu, K., Ni, L., Yang, Y., Liu, B., Wang, W., Wei, C., & Yang, J. (2020). The presence of SARS-CoV-2 RNA in the feces of COVID-19 patients. Journal of Medical Virology, 92(7), 833–840.
Fongaro, G., Stoco, P. H., Souza, D. S. M., Grisard, E. C., Magri, M. E., Rogovski, P., Schörner, M. A., Barazzetti, F. H., Christoff, A. P., de Oliveira, L. F. V., & Bazzo, M. L. (2021). The presence of SARS-CoV-2 RNA in human sewage in Santa Catarina, Brazil, November 2019. Science of the Total Environment, 778, 146198.
Gorbalenya, A. E., Baker, S. C., Baric, R., Groot, R. J. D., Drosten, C., Gulyaeva, A. A., Haagmans, B. L., Lauber, C., Leontovich, A. M., Neuman, B. W., & Penzar, D. (2020). Severe acute respiratory syndrome-related coronavirus: The species and its viruses–a statement of the Coronavirus Study Group.
Gwenzi, W. (2021). Leaving no stone unturned in light of the COVID-19 fecal-oral hypothesis? A water, sanitation and hygiene (WASH) perspective targeting low-income countries. Science of the Total Environment, 753, 141751.
Hemalatha, M., Kiran, U., Kuncha, S. K., Kopperi, H., Gokulan, C. G., Mohan, S. V., & Mishra, R. K. (2021). Surveillance of SARS-CoV-2 spread using wastewater-based epidemiology: Comprehensive study. Science of the Total Environment, 768, 144704.
https://www.cdc.gov/ (Accessed on 31 Dec 2021)
Johns Hopkins University and Medicine. Available online: https://coronavirus.jhu.edu/map.html (Last accessed on 9 Sept 2021).
Kopperi, H., Tharak, A., Hemalatha, M., Kiran, U., Gokulan, C. G., Mishra, R. K., & Mohan, S. V. (2021). Defining the methodological approach for wastewater based epidemiological studies–Surveillance of SARS-CoV-2. Environmental Technology & Innovation, 101696.
Kumar, M., Patel, A. K., Shah, A. V., Raval, J., Rajpara, N., Joshi, M., & Joshi, C. G. (2020). First proof of the capability of wastewater surveillance for COVID-19 in India through detection of genetic material of SARS-CoV-2. Science of the Total Environment, 746, 141326.
Kumar, M., Joshi, M., Shah, A. V., Srivastava, V., & Dave, S. (2021a). Wastewater surveillance-based city zonation for effective COVID-19 pandemic preparedness powered by early warning: A perspectives of temporal variations in SARS-CoV-2-RNA in Ahmedabad (p. 148367). Science of The Total Environment.
Kumar, M., Kuroda, K., Patel, A. K., Patel, N., Bhattacharya, P., Joshi, M., & Joshi, C. G. (2021b). Decay of SARS-CoV-2 RNA along the wastewater treatment outfitted with Upflow Anaerobic Sludge Blanket (UASB) system evaluated through two sample concentration techniques. Science of the Total Environment, 754, 142329.
Kumar, M., Joshi, M., Patel, A. K., & Joshi, C. G. (2021c). Unravelling the early warning capability of wastewater surveillance for COVID-19: A temporal study on SARS-CoV-2 RNA detection and need for the escalation. Environmental Research, 196, 110946.
La Rosa, G., Iaconelli, M., Mancini, P., Ferraro, G. B., Veneri, C., Bonadonna, L., Lucentini, L., & Suffredini, E. (2020). First detection of SARS-CoV-2 in untreated wastewaters in Italy. Science of the Total Environment, 736, 139652.
Medema, G., Heijnen, L., Elsinga, G., Italiaander, R., & Brouwer, A. (2020). Presence of SARS-Coronavirus-2 RNA in sewage and correlation with reported COVID-19 prevalence in the early stage of the epidemic in the Netherlands. Environmental Science & Technology Letters, 7(7), 511–516.
Mehta, P., McAuley, D. F., Brown, M., Sanchez, E., Tattersall, R. S., & Manson, J. J. (2020). COVID-19: Consider cytokine storm syndromes and immunosuppression. The Lancet, 395(10229), 1033–1034.
Naqvi, A. A. T., Fatima, K., Mohammad, T., Fatima, U., Singh, I. K., Singh, A., Atif, S. M., Hariprasad, G., Hasan, G. M., & Hassan, M. I. (2020). Insights into SARS-CoV-2 genome, structure, evolution, pathogenesis and therapies: Structural genomics approach. Biochimica et Biophysica Acta (BBA)-Molecular Basis of Disease, 1866(10), 165878.
Nemudryi, A., Nemudraia, A., Wiegand, T., Surya, K., Buyukyoruk, M., Cicha, C., Vanderwood, K. K., Wilkinson, R., & Wiedenheft, B. (2020). Temporal detection and phylogenetic assessment of SARS-CoV-2 in municipal wastewater. Cell Reports Medicine, 1(6), 100098.
Peng, L., Liu, J., Xu, W., Luo, Q., Chen, D., Lei, Z., Huang, Z., Li, X., Deng, K., Lin, B., & Gao, Z. (2020). SARS-CoV-2 can be detected in urine, blood, anal swabs, and oropharyngeal swabs specimens. Journal of Medical Virology, 92(9), 1676–1680.
Randazzo, W., Truchado, P., Cuevas-Ferrando, E., Simón, P., Allende, A., & Sánchez, G. (2020). SARS-CoV-2 RNA in wastewater anticipated COVID-19 occurrence in a low prevalence area. Water Research, 181, 115942.
Rothan, H. A., & Byrareddy, S. N. (2020). The epidemiology and pathogenesis of coronavirus disease (COVID-19) outbreak. Journal of Autoimmunity, 109, 102433.
Sharma, D. K., Nalavade, U. P., Kalgutkar, K., Gupta, N., & Deshpande, J. M. (2021). SARS-CoV-2 detection in sewage samples: Standardization of method & preliminary observations. The Indian Journal of Medical Research, 153(1–2), 159.
Sims, N., & Kasprzyk-Hordern, B. (2020). Future perspectives of wastewater-based epidemiology: Monitoring infectious disease spread and resistance to the community level. Environment International, 139, 105689.
Sims, J. T., Krishnan, V., Chang, C. Y., Engle, S. M., Casalini, G., Rodgers, G. H., Bivi, N., Nickoloff, B. J., Konrad, R. J., de Bono, S., & Higgs, R. E. (2021). Characterization of the cytokine storm reflects hyperinflammatory endothelial dysfunction in COVID-19. Journal of Allergy and Clinical Immunology, 147(1), 107–111.
Street, R., Malema, S., Mahlangeni, N., & Mathee, A. (2020). Wastewater surveillance for Covid-19: An African perspective. Science of the Total Environment, 743, 140719.
Tiwari, S. B., Gahlot, P., Tyagi, V. K., Zhang, L., Zhou, Y., Kazmi, A. A., & Kumar, M. (2021). Surveillance of wastewater for early epidemic prediction (SWEEP): Environmental and health security perspectives in the post-COVID-19post-COVID-19post-COVID-19 Anthropocene. Environmental Research, 195, 110831.
Weidhaas, J., Aanderud, Z. T., Roper, D. K., VanDerslice, J., Gaddis, E. B., Ostermiller, J., Hoffman, K., Jamal, R., Heck, P., Zhang, Y., & Torgersen, K. (2021). Correlation of SARS-CoV-2 RNA in wastewater with COVID-19 disease burden in sewer sheds. Science of the Total Environment, 775, 145790.
Young, B. E., Ong, S. W. X., Kalimuddin, S., Low, J. G., Tan, S. Y., Loh, J., Ng, O. T., Marimuthu, K., Ang, L. W., Mak, T. M., & Lau, S. K. (2020). Epidemiologic features and clinical course of patients infected with SARS-CoV-2 in Singapore. JAMA, 323(15), 1488–1494.
Zaneti, R. N., Girardi, V., Spilki, F. R., Mena, K., Westphalen, A. P. C., da Costa Colares, E. R., Pozzebon, A. G., & Etchepare, R. G. (2021). Quantitative microbial risk assessment of SARS-CoV-2 for workers in wastewater treatment plants. Science of the Total Environment, 754, 142163.
Zhu, N., Zhang, D., Wang, W., Li, X., Yang, B., Song, J., Zhao, X., Huang, B., Shi, W., Lu, R., & Niu, P. (2020). A novel coronavirus from patients with pneumonia in China, 2019. New England journal of medicine.
Acknowledgements
The study group would like to acknowledge the constant support received from Dr. B. Lal Gupta (Director) and Dr. Aparna Datta (Principal). The support received from the Centre for Innovation, Research, and Development (CIRD, Dr. B. Lal Clinical Laboratory Pvt. Ltd.) for analysis and the Jaipur development authority (JDA) officials and plant operators at WWTPs is sincerely acknowledged.
Funding
This work was financially supported by the Internal Mural Grants (IMG) Fund (BIBT/IRSC/IMG/2020–21/036), supported by IRSC, Dr. B. Lal Institute of Biotechnology, Jaipur, and Dr. Xuan Li was also supported by the Australian Research Council Discovery Project (DP190100385).
Author information
Authors and Affiliations
Contributions
Sudipti Arora: conceptualization, methodology, validation, formal analysis, investigation, resources, writing – original draft, writing – review and editing, project administration, funding acquisition. Aditi Nag: conceptualization, formal analysis, investigation, writing – original draft, writing – review and editing, visualization. Aakanksha Kalra: formal analysis, visualization. Vikky Sinha: Investigation. Ekta Meena: investigation. Samvida Saxena: investigation. Devanshi Sutaria: investigation, writing – review and editing. Manpreet Kaur: investigation. Tamanna Pamnani: investigation. Komal Sharma: investigation. Sonika Saxena: resources, supervision, project administration. Sandeep K Shrivastava: resources, methodology, validation. AB. Gupta: conceptualization, formal analysis, writing – review and editing. Xuan Li: formal analysis, writing – review and editing. Guangming Jiang: formal analysis, writing – review and editing.
Corresponding author
Ethics declarations
Ethics approval
The work has been reviewed and approved by the Institutional ethics committee under grant no. BIBT/IRSC/IMG-036.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Highlights
• Positive rates and viral loads best correlated with new cases at 20-22 days lag.
• A comparison of SARS-CoV-2 RNA removal efficacy of 9 WWTPs was investigated.
• SBR showed better performance than MBBR with SARS-CoV-2 RNA removal from wastewater.
• Presence of SARS-CoV-2 in effluent reported even after UV and Chlorine disinfection.
• Using a combination of different detection genes increases sensitivity in WBE.
Rights and permissions
About this article

Cite this article
Arora, S., Nag, A., Kalra, A. et al. Successful application of wastewater-based epidemiology in prediction and monitoring of the second wave of COVID-19 with fragmented sewerage systems–a case study of Jaipur (India). Environ Monit Assess 194, 342 (2022). https://doi.org/10.1007/s10661-022-09942-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10661-022-09942-5