
Abstract
In Australia, paramedics are obliged to practice ethically. Graduates of baccalaureate degrees in paramedicine should therefore possess a common grounding in ethics to meet the professional capabilities expected of registered paramedics. However, there is a lack of clarity regarding ethics education for paramedicine students, including what is taught, how it is taught, and how it is assessed. This paper explores ethics education for paramedicine students in Australia, how it aligns with current professional expectations, and how it may be enhanced. Point-in-time data regarding ethics education was collected from websites of fifteen Australian universities offering undergraduate baccalaureate degrees in paramedicine. Data collection was supported by consultation with academics from several institutions. Content analysis was utilised to categorise and analyse data to explore similarities and differences in curricula. Similarities included approaches to learning and teaching and the use of case-based learning, with variability found across teaching staff profiles and content areas. Findings suggest it is time for collaboration to develop a model ethics curriculum for paramedicine students in Australia.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Paramedics in Australia play a crucial role in delivering advanced pre- and out-of-hospital care to the community, from acute critical care to palliative support at the end of life. Diversity is not only experienced through their clinical caseload, but also across cultural contexts and in geographically disparate settings, from metropolitan locations through to regional and remote sites (Hartley, 2012; O'Meara & Duthie, 2018). The cases attended by paramedics can present a range of ethical dilemmas, including but not limited to refusal of service, the protection of vulnerable persons, resuscitation decisions, and challenges involving advance care directives (Adams et al., 1992; Heilicser et al., 1996; Moore, 2020; Moritz et al., 2020; Nordby & Nøhr, 2012; Shearer et al., 2021). In the past, paramedics have articulated the need for improved ethics education to assist them in dealing with the ethical problems faced (Heilicser et al., 1996, p. 242). There have been few studies addressing this need; however, recent research has revealed that paramedics rely more on experience than education to resolve ethical dilemmas (Shearer et al., 2021, p. 336). This is problematic as students of paramedicine have limited opportunities to gain clinical experience underscoring the need to rely on education to provide the theoretical knowledge and skills underpinning good ethical decision making for paramedics.
In December 2018, paramedicine became a regulated profession in Australia under the National Registration and Accreditation Scheme, established by Australian governments (Commonwealth of Australia, 2022) and regulated by the Paramedicine Board of Australia. The Board is supported by the administrative arm of the scheme, the Australian Health Practitioner Regulation Agency (‘AHPRA’) (Australian Health Practitioner Regulation Agency, 2018; Paramedicine Board of Australia, 2021a). Among other roles, the Paramedicine Board functions to develop standards, codes, and guidelines for the profession, approve accreditation standards, and subsequently accredit approved programs of study (Paramedicine Board of Australia, 2021a). Three documents published by the Paramedicine Board of Australia guide the expectations of paramedics. Two of these documents, the ‘Code of Conduct’ (2018) and ‘Professional capabilities for registered paramedics’ (2021), focus on the expectations of the individual paramedic; while the ‘Accreditation Standards: Paramedicine’ (2020) outline the expectations on education providers to develop ‘work-ready’ graduates capable of meeting professional requirements (Paramedicine Board of Australia, 2018, 2020, 2021b).
The accreditation standards require courses to have learning outcomes that address all the professional capabilities for paramedics (Paramedicine Board of Australia, 2020, p.16), including Domain 1 of the professional capabilities document: ‘The professional and ethical practitioner’ (Paramedicine Board of Australia, 2021b, p. 3–4). Australian universities offering degrees in paramedicine are currently aligning their courses with the new accreditation standards. This realignment and impending accreditation of undergraduate courses under the new scheme presents a timely opportunity to explore ethics education for paramedic students in Australia, to identify how it could be enhanced to ensure graduates are adequately prepared to practice professionally and in accordance with the requisite standards.
This study, focusing on undergraduate baccalaureate students of paramedicine in Australia, seeks to document the design and delivery of ethics education and consider whether it meets the current and future needs of students seeking to develop practical ethical aptitude. As the teaching of ethics in paramedicine remains a relatively young field, the medical literature will be drawn on to inform an understanding of the findings, as independent practice is a common feature of both disciplines, and the challenges of practice are shared. Teaching ethics within medical education is well-developed and provides insights that may assist in elevating the teaching of ethics to students of paramedicine, ensuring graduates are prepared for professional registration and practice. Of note when discussing ethics education is the often observed overlap between ethics and law. As Olick (2001) comments, it is not infrequent that clinicians are required to consider both the ethical and legal dimensions of challenges presented in patient care. In both medicine (and paramedicine as evidenced below), some institutions teach ethics and law separately, whereas others prefer teaching them together. It is beyond the scope of this paper to explore this aspect in any detail, though it may be an important topic for future research.
Materials and Methods
During the point-in-time data collection period in January/February 2021, a search for university courses offering paramedicine was conducted using the peak paramedic industry group, the Council of Ambulance Authorities (2022) website, and cross-referenced with accredited programs of study information from the Australian Health Practitioner Regulation Agency (AHPRA) Paramedicine Board of Australia website. Fifteen universities offering pre-registration undergraduate baccalaureate degrees in paramedicine were identified and included in this study. This incorporated courses that were dual degrees (for example, Bachelor of Nursing/Bachelor of Paramedicine), conversion courses (for example, Bachelor of Paramedic Practice [Conversion Pathway]), and Honours courses. Pre-registration refers to a comprehensive undergraduate degree with a full complement of units leading to registration as a paramedic. Postgraduate course unit offerings were excluded, as the intent was to focus on foundational ethics education and assess like-for-like courses.
Publicly available course information was obtained from relevant university websites, and the course structure was purposefully searched for subjects/units pertaining to ethics. Where no dedicated ethics subject/unit was easily identified, other subject/units within the course were searched for relevant ethics content.
All subjects/units that contained content related to ethics were then subjected to analysis using a data extraction framework. Core details were recorded according to the data extraction framework, including subject/unit code and title; study mode; the year of study in which the subject/unit was offered (for example, 1st, 2nd or third year); the unit overview or aims; learning outcomes; syllabus; learning and teaching strategies; assessment strategy and rationale and any resource information, such as utilised textbooks (where available).
A qualitative study design employing document analysis using a systematic process for sourcing, selecting, evaluating, and synthesising data from printed and electronic documents was used to analyse data from the fifteen university websites (Bowen, 2009). Data were transferred from each website verbatim into an Excel spreadsheet. Due to the diversity of data format and content available across university websites, the design framework was expanded to ensure data were captured relevant to each category. As a result, there are some gaps in the data where the information was not available on a particular university website.
Some of these gaps were able to be filled via follow-up Zoom discussions with key academic staff involved in course delivery. Each university was contacted with the offer to add detail to the data collected from the websites. Initial contact was via email, with non-responses followed up twice more to ensure maximum opportunity to participate in the discussions. Nine of the fifteen universities engaged in this opportunity. This information was entered into a separate section of the Excel spreadsheet to ensure clarity of the data source. Transcript documents were created from the discussions, and qualitative content analysis, a ‘…systematic and objective means to make valid inferences from verbal, visual, or written data’, was used to analyse data from the transcripts (Downe-Wamboldt, 1992, p. 314; Elo & Kyngäs, 2008).
Data extracted from websites was then triangulated with transcripts from the discussions with academic staff to enable corroboration and validation (Bowen, 2009). Evaluated data were then integrated, categorised, and thematically analysed by the first author to formulate results.
Please note that the first author was appointed as an Accreditation Assessor with the Paramedicine Board of Australia during the data collection phase of this study. This appointment was declared at consultations with academics after the commencement date in January 2021. The first author did not participate in any accreditation assessments during the data collection phase of this study.
Results
Teaching Staff
The data were not available for academics allocated teaching of the units at four of the fifteen universities. For the remaining eleven universities, there was a mix of academic profiles. Some ethics units were taught purely by paramedics, while others involved a combination of paramedics and lawyers (whether the same individual or two (or more) separate academics). Other academic profiles included a lawyer, a registered nurse/lawyer, an epidemiologist, a nurse/philosopher, or a legal practitioner/health professional (clinical counsellor).
Stand-alone Or Embedded Ethics Content?
Nine of the fifteen universities offered discrete units listing ethics and law in the unit title. Three universities offered ethics content in ‘foundations of paramedicine’ units, while the remaining three offered ethics content in combination with professionalism, policy or society and culture.
Teaching Format
There was no consistency as to when the ethics content was taught across university courses, with scheduling occurring across the first, second, and third year of courses. Delivery also varied, however, some of the variations occurred due to the impact of COVID-19 and the need for some universities to move to an online teaching mode where they usually would offer units face-to-face. Of the fifteen universities, seven offered their unit in a mixed-mode, which encompasses ‘blended’ learning, or a combination of face-to-face and online learning. Five universities offered their ethics units face-to-face only, though one of these universities transitioned to online learning due to COVID-19. Three universities offered their units online only.
Textbooks
Eleven of the fifteen universities offered information on prescribed or recommended textbooks via their respective websites or through discussion with academics. No specific data were available from four universities, although an academic from one of these remaining four universities indicated that they use references from various texts, rather than one specifically, with a preference for journal articles to blend the research and best contemporary evidence. Supplementary readings were also used by other universities to support learning.
There are nine specific law and/or ethics textbooks used by universities, listed in Table 1. Of those nine, five covered ethics and law, with four of these five being paramedic specific and at least three of these engaging the expertise of a paramedic ethicist. Of the remaining four texts, two were ethics specific, and two were law specific, though neither of these four were paramedic specific.
Unit Overviews
Unit overviews expanded upon and reflected the subject titles (see Table 2). Again, there was considerable variance between the detail provided within the unit overviews, with some offering a brief synopsis of the unit content while others were more expansive.
Unit overviews identified broad areas covered within units related to ethics, including decision-making (clinical, intuitive, analytical, safe & reasoned); a wide range of paramedic knowledge skills and attributes, for example, approach to patient-centred care, the role of the paramedic, introductory skills, and physical and mental preparedness; and references to context, such as the healthcare system, regulatory structures, registration, and policy. Learning and teaching approaches, both online and face-to-face, were articulated in some unit overviews, with the use of case studies, critical reflection and discussion featuring heavily. There was a strong emphasis on ethics and law across unit overviews, focusing on theories, principles, choices, and challenges. Legal principles, legislation and the legal system were particularly showcased. Topics concerning professionalism were included in some unit overviews, covering areas such as professional practice, communication, conduct, standards, and professional responsibility. Other areas less frequently covered include philosophy, cultural awareness and safety, and caring for vulnerable populations.
Learning Outcomes
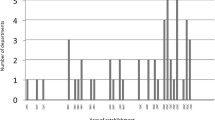
Available data were collated regarding learning outcomes for each identified unit. Learning outcomes were available for all but one of the universities. The data were tabulated with learning outcomes transcribed verbatim, then grouped according to the subject area (refer to Fig. 1).

Learning outcomes
Learning outcomes relating to law only were identified as such. Where there was generalised mention of law and ethics, learning outcomes were placed within that grouping. Any specific mention of legal or ethical principles or ethical decision-making were identified and grouped separately.
Paramedic specific areas included a broad range of paramedic-specific outcomes, including but not limited to emotional/social skills and paramedic wellbeing, patient assessment and history taking, basic procedures and skills in paramedicine, manual handling, and communication, including medical terminology.
Content Areas
For two universities, no unit content or syllabus data were available from their respective websites or via Zoom consults. Only limited data were available from respective university websites at a further four universities, again with no additional context available via Zoom consults. The remaining nine university data sets regarding content offer greater depth, with information from their websites supported by information elicited from Zoom consults with academics (refer to Fig. 2 and Table 3).

Content areas. OHS Occupational health and safety, EEA Emergency Examination Authority, AHPRA Australian Health Practitioner Regulation Agency
There was a broad range of content areas across the data set. Common content included professionalism and related topics and ethics, including applied ethics. Legal and ethical issues related to vulnerable populations, such as Indigenous health, child protection, mandatory reporting, elder abuse, guardianship, sexual assault, developmental disability, women, adolescents and children, were also common. Other popular content included privacy and confidentiality; and consent and refusal. Less commonly covered content included medico-legal issues of restraint, ethics of expert testimony, and biomedical research.
Approaches to Learning and Teaching
Data regarding approaches to learning and teaching was available from twelve of the fifteen universities. Information was extracted from unit overviews and learning and teaching strategies from university websites, supported by data from Zoom consults with academics where available. Analysed results were then tabulated (see Figs. 3 and 4).

Pedagogical tools

Pedagogical approaches
Pedagogical tools were examined and identified. The use of workbooks or modules featured, with several universities utilising these tools as pre-work for either face-to-face or online tutorials. There were consistent themes within pedagogical approaches, including encouraging engaged discussion, group work and collaborative learning, and a strong focus on the practical application of knowledge. Consistent with these approaches was an emphasis on case-based education across universities, with many utilising case scenarios as an applied approach to considering principles, concepts, theories, and legislation. Less common strategies included the analysis of arguments and challenges, problem-solving and communication strategies.
Assessment
The types of assessments utilised across paramedic science ethics curricula are shown in Fig. 5. No data were available for two of the universities. Of the available information, it is evident that a broad range of assessments are conducted at various points throughout the curricula. The most common assessment type was written assessment, followed by online tests or quizzes. Examination was the third most utilised form of assessment. A mix of question types was used in the tests/quizzes and examinations, including multiple-choice and short answer questions. Other methods of assessment included case studies, posters, and group presentations. During a Zoom consult, one university academic articulated that they use a continuous assessment process in the form of written assessments at the end of each module rather than one end of unit examination.

Assessment types used
Discussion
The introduction of professional registration for paramedics in Australia in late 2018, and the publication more recently of documents outlining the obligation for paramedics to practice ethically, suggests that it is timely to critically reflect on the formal ethics education provided in undergraduate paramedic education in Australia.
Teaching Staff
As an initial point of discussion, it is important to explore who should be teaching ethics in paramedicine. This study found heterogeneity among academics engaged in teaching ethics-related units to paramedicine students at Australian universities with respect to their backgrounds and fields of expertise. While further research may elicit academics’ formal qualifications, there is no current consensus about those qualifications. Braunack‐Mayer et al. (2001) identified the lack of standardised qualifications for teaching ethics in medical schools as a challenge in medicine. Stipulating specific qualifications can prove difficult however the literature indicates academics with an appropriate ethics background, such as a higher degree with an emphasis on ethics, was highly desirable (Braunack‐Mayer et al., 2001). At the very least, academics engaged in teaching ethics should possess a good understanding of moral philosophy and familiarity with and confidence in the clinical environment (Braunack‐Mayer et al., 2001; Giubilini et al., 2016), emanating from professional experience.
A range of teaching profiles were endorsed by the academics consulted in this study. As an example, one academic voiced that the combination of an expert in law and ethics and a paramedic for contextualisation was the perfect combination of teaching team for such subjects. This academic noted that while paramedics have a good working knowledge, we are not experts in the law. As such, we should engage people to teach it that are, although a paramedic should be present to contextualise learning from praxis, which would meet the accreditation requirement for academics to hold the relevant qualifications and experience (Paramedicine Board of Australia, 2020). Previous research in the medical field, for example, by Lehmann et al. (2004), found that Deans of U.S. and Canadian medical schools expressed that being a physician was insufficient to be an effective teacher of professional ethics. Similarly, Giubilini et al. (2016) asserted that an ethics expert and a clinical expert would be a more effective way to deliver ethics education sessions. While it is acknowledged teachers of ethics require specialist training (Lehmann et al., 2004) to meet the need for vertical and horizontal integration of ethics throughout the paramedicine curriculum, Stirrat (2010) argues that teaching should be a shared obligation, not only the responsibility of dedicated academics. As such, Stirrat (2010) advocates support for improving the knowledge of all academics regarding ethics and law. Therefore, key stakeholders ought to be engaged to explore best practice regarding academic staff involved in teaching ethics.
Stand-alone or Embedded Content/Teaching Format
While most (n = 9) of the fifteen universities offering paramedicine have discrete units addressing ethics and law within the curriculum, others have elected to integrate the study of ethics with other subject areas such as professionalism or culture. Accompanying this variance was a disparity in views expressed by academics as to when ethics should be taught. Some felt students needed at least some foundational knowledge prior to any clinical placement, while others felt it important for students to develop an understanding of the profession gained through clinical exposure to support their learning of ethics in paramedicine. Perhaps the answer lies in the overall program design.
‘The Accreditation Standards: Paramedicine’ specifically articulate the need for ‘vertical and horizontal integration of theoretical concepts and practical application throughout the program’ (Paramedicine Board of Australia, 2020, p. 16). The integration of ethics education within current paramedicine curricula was not obvious to the authors of this study. How best to integrate ethics education vertically and horizontally to reflect ethics being intrinsic to paramedic practice is one area that needs further consideration and was raised in discussions with academics as a point of reflection and future action.
Paramedicine can learn about improved integration of ethics education from the experience gained in medicine. Teachers of medical ethics and law in U.K. medical schools published a consensus statement, which asserts that: ‘ethics and law teaching should be features of the whole curriculum, should begin early and be reinforced throughout the course’ (Ashcroft et al., 1998, p. 191). Similarly, a 2004 survey of U.S. and Canadian medical schools found that many of their respondents articulated the need for ‘horizontal and longitudinal integration’ of ethics curricula across each year of a medical degree (Lehmann et al., 2004). In 2001 a working group on behalf of teachers of ethics and law in Australian and New Zealand medical schools followed the U.K.’s lead and published a position statement on an integrated ethics curriculum (Braunack‐Mayer et al., 2001). Findings from a recent study by Torda and Mangos (2020) suggests that ethics education is now integrated and interspersed with other content in Australasian medical schools.
The medical research demonstrates that a more integrated approach better endows students with core foundational knowledge and experience as they enter the profession and gain further insights from praxis. Paramedic practice involves the integration of clinical and non-clinical skills (including law and ethics). As such, an approach to enhancing ethics education in paramedicine may be to introduce a foundational unit on ethics and law early in the curriculum. This unit would introduce key concepts taught by subject matter (law and ethics) experts who would work alongside a paramedic to provide context. Ethical and legal principles and concepts could then be better incorporated throughout other subjects over the remaining curriculum, and thus more accurately reflect practice which integrates both clinical and non-clinical considerations and decision-making. It must be noted, however, that one of the risks of integrated ethics content is that it becomes diminished if not reinforced as a key aspect of the curriculum (Ashcroft et al., 1998; DuBois & Burkemper, 2002). As a profession, paramedicine could gain from medicine’s experience by engaging key stakeholders to develop a consensus statement on vertical and horizontal integration of ethics within paramedicine curricula.
Textbooks
The utilisation of paramedic specific textbooks across universities teaching undergraduate paramedicine in Australia is fairly homogenous, with strong engagement with ethics and law texts written by subject matter experts. This differs substantially to international findings, such as those articulated by DuBois and Burkemper (2002, p. 434) of 58 syllabi explored in US medical schools consisting of 1,191 distinct readings, with only eight of these homogenous across six schools. Similarly, a broad and generic list of ethics curriculum resources for emergency medicine graduate medical education was put forth by Marco et al. (2011).
Paramedic specific textbooks are particularly important when reflecting on the heterogeneity of academics involved in teaching ethics. Paramedic academics lacking expertise in ethics are likely to be dependent on textbooks to help inform their teaching and serve as a particularly helpful reference given the unique challenges faced in praxis.
Content Areas
The breadth of content areas found in this study reflects the various approaches taken by universities to fit ethics-related content into a crowded paramedicine curriculum. The problem with the varied approach is that graduates from different universities potentially possess vastly different underpinning knowledge and understanding of how to resolve ethical challenges in practice.
Australian and international medical schools addressed this consistency issue by developing position statements on ethics core curriculum (Ashcroft et al., 1998; Braunack‐Mayer et al., 2001). These statements outline the core content, including knowledge, skills, and attitudes, as well as recommended teaching methods and assessment for ethics education in medical schools (Ashcroft et al., 1998; Braunack‐Mayer et al., 2001). Similarly, in Australia, the law discipline has 11 compulsory core units as the minimum academic study requirement for admission to legal practice in Australia, of which legal ethics is one (Victorian Legal Admissions Board, 2021). Paramedicine could consider a similar solution.
A national consensus for ethics curricula could consist of agreed core content areas and a range of electives. Electives would be an essential consideration as elements of the ethics curriculum must remain dynamic to accommodate changes in contemporary practice and to ensure students can develop skills in addressing novel questions raised by current events, such as the impact of the COVID-19 pandemic, as one example (Maguire et al., 2020).
Approaches to Learning and Teaching (Pedagogical Tools/Approaches)
A broad range of pedagogical tools and approaches were found to be used by academics involved in this study. These included the use of modules and workbooks, engaged discussion, group work and collaborative learning. Irrespective of the delivery platform, the use of case studies was common and justified by participants as a way to enable students to practically engage in cases and discussion. The early utilisation of case studies in ethics education in paramedicine is a positive, given the evidence that they are an effective form of teaching (Brooks & Bell, 2017; Lehmann et al., 2004).
Medical students struggled with applying knowledge of ethics to clinical cases as much ethics education focused on knowledge acquisition rather than the process of ethical analysis and reasoning (Myser et al., 1995). It was argued that programs should reorient themselves more towards questions that challenge students to extend their current ethical thinking and apply it to the situations faced in ordinary clinical practice (Scher & Kozlowska, 2018, p. 114). Later studies of undergraduate medical programs, such as a scoping review by Souza and Vaswani (2020), found simulation using problem-based learning and case studies featured heavily as teaching methods. Engaging students in small groups utilising these approaches was also effective (Torda & Mangos, 2020).
Approaches to learning and teaching ethics and law should be “attuned to the students’ needs appropriate both to their particular stage of training and to relevant specialty-specific ethical issues”(Stirrat, 2010, p.156). This suggests that learning should be scaffolded to become more complex and challenging as students’ progress in their studies, further emphasising the need for vertical and horizontal integration of ethics in the curriculum. Within paramedicine, the current use of case-based scenarios could be used as a foundation for a greater focus on ethics learning outcomes in scaffolded clinical placements to provide students with a practical opportunity to experience, observe, and reflect upon ethical challenges handled in praxis (Brooks & Bell, 2017). This would allow students to develop transferable skills to enable real-world decision-making.
Assessment
Within this study cohort, written assessment, online tests or quizzes, and examinations were the most utilised assessment approaches. Other methods of assessment included case studies, posters, and group presentations. While written assessment, online quizzes and examinations certainly have their place in assessment strategies, this could be balanced with more applied methods assessing ethical and legal competencies, demonstrated in practical assessments such as OSCEs and simulated case studies.
In their study of 125 U.S. and 16 Canadian medical schools, Lehmann et al. (2004) reported that just over half of the medical schools assessed students’ ability to reason morally; in addition, one third formally evaluated students’ performance in ethically difficult simulated situations, such as delivering bad news or discussing do not resuscitate orders. It seems remiss in practically orientated professions such as medicine and paramedicine that more applied strategies are not well utilised. Other suggestions include student reflections after the course, simulated patient interactions, and patient evaluation of the students (Souza & Vaswani, 2020). Students are more likely to integrate clinical ethical reasoning skills into their learning when they understand the practical application of those skills in the management of cases will be assessed (Myser et al., 1995). Furthermore, the assessment of competence in ethics reinforces the importance of ethical analysis and reasoning relative to other discipline areas within the curriculum (Myser et al., 1995; Savulescu et al., 1999).
The authors suggest that the assessment strategy should be scaffolded, increasing experiential complexity as students’ progress with their studies. Hence high-fidelity case scenarios using trained actors followed by real-time feedback and student reflection on the case may be a good approach (Marco et al., 2011), particularly if feedback is offered from the situational perspective of both the patient and professional, which Higgs (1987) considers essential. Approaches to scenarios could be adapted for both face-to-face and online learning environments.
Limitations
All available data from university websites were collected during a short period and taken at face value, supported by consultation with academics where available. As not all universities participated in the discussion activity, there is an inevitable difference in the range and depth of information collected across the fifteen institutions providing undergraduate baccalaureate degrees in paramedicine. This was particularly the case when unit titles did not explicitly mention ethics. Where unit titles were overt, no further exploration of other units occurred – alternate sources of ethics education were only sought where specific units of study were not self-evident. As a result, there may well be introductory sources of ethics education in addition to overt units of study.
As previously noted, compared to medicine, the teaching of ethics is still a relatively young field in paramedicine. As such, the medical literature regarding ethics education has been referenced in this paper due to a paucity of relevant literature in the paramedic discipline. It must be noted that a full comparison of the two professions has not been explored in this paper. Perhaps associated with endeavours to achieve consensus on what should be delivered in paramedic ethics education, should be an accompanying consideration of how medicine and paramedicine differ, and how paramedicine could engage in further research to build a stronger foundation of literature from which our own profession can draw.
Conclusion
Graduates of baccalaureate degrees in paramedicine should possess a common grounding in ethics to meet the professional capabilities expected of registered paramedics in Australia. Findings in this study reveal differences across university courses, with a wide variety of content, methods of delivery, and assessment resulting in a diverse overall design of ethics curricula suggesting that this common ground is not yet present.
To date, there has been limited opportunity to engage academics to discuss and achieve consensus about the elements spoken of in this study. However, the evolution of paramedicine as a profession, the new regulatory environment, and the current focus on educational adjustment to meet accreditation requirements serves as the perfect juncture to explore ethics education in the paramedicine curriculum in Australia.
Ideally, an ethics curriculum should be integrated horizontally and vertically across the years of the paramedicine program to reflect the experience of praxis and the inherent nature of ethical challenges, experiences and dilemmas encountered by paramedics. Future endeavours should identify barriers to integrated ethics curriculum and seek to address the need for consensus on a responsive model curriculum that prepares graduates to engage holistically in the profession they are about to enter.
Data Availability
The datasets generated and analysed during the current study are available from the corresponding author on reasonable request.
References
Adams, J., Arnold, R., Siminoff, L., & Wolfson, A. (1992). Ethical conflicts in the prehospital setting. Annals of Emergency Medicine, 21(10), 1259–1265. https://doi.org/10.1016/S0196-0644(05)81759-7
Ashcroft, R., Baron, D., Benatar, S., Bewley, S., Boyd, K., Caddick, J., Campbell, A., Cattan, A., Clayden, G., Day, A., Dlugolecka, M., Dickenson, D., Doyal, L., Draper, H., Farsides, B., von Fragstein, M., Fulford, K., Gillon, R., Goodman, D., & de Zulueta, P. (1998). Teaching medical ethics and law within medical education: A model for the UK core curriculum. Journal of Medical Ethics, 24(3), 188–192. https://doi.org/10.1136/jme.24.3.188
Australian Health Practitioner Regulation Agency. (2018). Paramedics: Welcome to the profession. Retrieved November 29, 2021, from https://www.ahpra.gov.au/News/2018-11-30-Paramedics-Welcome-to-the-National-Scheme.aspx
Bowen, G. A. (2009). Document analysis as a qualitative research method. Qualitative Research Journal, 9(2), 27–40. https://doi.org/10.3316/QRJ0902027
Braunack-Mayer, A. J., Gillam, L. H., Vance, E. F., Gillett, G. R., Kerridge, I. H., McPhee, J., Saul, P., Smith, D. E., Wellsmore, H. M., Koczwara, B., Rogers, W. A., Stoffell, B. F., McNeill, P. M., Newell, C. J., Parker, M. H., Walton, M., & Whitehall, J. S. (2001). An ethics core curriculum for Australasian medical schools. Medical Journal of Australia, 175(4), 205–210. https://doi.org/10.5694/j.1326-5377.2001.tb143097.x
Brooks, L., & Bell, D. (2017). Teaching, learning and assessment of medical ethics at the UK medical schools. Journal of Medical Ethics, 43(9), 606–612. https://doi.org/10.1136/medethics-2015-103189
Commonwealth of Australia. (2022). National Registration and Accreditation Scheme. Retrieved January 25, 2022, from https://www.health.gov.au/initiatives-and-programs/national-registration-and-accreditation-scheme
Council of Ambulance Authorities. (2022). Where can I study to become a paramedic? Retrieved January 25, 2022, from https://www.caa.net.au/
Downe-Wamboldt, B. (1992). Content analysis: Method, applications, and issues. Health Care for Women International, 13(3), 313–321. https://doi.org/10.1080/07399339209516006
DuBois, J., & Burkemper, J. (2002). Ethics education in U.S. medical schools: A study of syllabi. Academic Medicine, 77(5), 432–437. Retrieved February 17, 2022, from https://journals.lww.com/academicmedicine/Fulltext/2002/05000/Ethics_Education_in_U_S__Medical_Schools__A_Study.19.aspx
Elo, S., & Kyngäs, H. (2008). The qualitative content analysis process. Journal of Advanced Nursing, 62(1), 107–115. https://doi.org/10.1111/j.1365-2648.2007.04569.x
Giubilini, A., Milnes, S., & Savulescu, J. (2016). The medical ethics curriculum in medical schools: Present and future. Journal of Clinical Ethics, 27(2), 129–145.
Hartley, P. R. (2012). Paramedic practice and the cultural and religious needs of pre-hospital patients in Victoria. Victoria University.
Heilicser, B., Stocking, C., & Siegler, M. (1996). Ethical dilemmas in emergency medical services: The perspective of the emergency medical technician. Annals of Emergency Medicine, 27(2), 239–243. https://doi.org/10.1016/S0196-0644(96)70330-X
Higgs, R. (1987). CABGs and KINGS: Relevance and realism in the teaching of clinical ethics in Camberwell. Journal of Medical Ethics, 13(3), 157–159. https://doi.org/10.1136/jme.13.3.157
Lehmann, L. S., Kasoff, W. S., Koch, P., & Federman, D. D. (2004). A survey of medical ethics education at U.S. and Canadian medical schools. Academic Medicine, 79(7), 682–689. https://doi.org/10.1097/00001888-200407000-00015
Maguire, B., O’Neill, B., Shearer, K., McKeown, J., Phelps, S., Gerard, D., Handal, K., & Maniscalco, P. (2020). The ethics of PPE and EMS in the COVID-19 era. Journal of Emergency Medical Services. Retrieved December 15, 2021, from https://www.jems.com/exclusives/ethics-of-ppe-and-ems-in-the-covid-19-era/
Marco, C. A., Lu, D. W., Stettner, E., Sokolove, P. E., Ufberg, J. W., & Noeller, T. P. (2011). Ethics curriculum for emergency medicine graduate medical education. Journal of Emergency Medicine, 40(5), 550–556. https://doi.org/10.1016/j.jemermed.2010.05.076
Moore, E. (2020). Respecting an autonomous decision to refuse life-saving treatment: a case study. Journal of Paramedic Practice, 12(8), 304–309. https://doi.org/10.12968/jpar.2020.12.8.304
Moritz, D., Ebbs, P., & Carver, H. (2020). Paramedic ethics, capacity and the treatment of vulnerable patients. Journal of Paramedic Practice, 12(12), 1–7. https://doi.org/10.12968/jpar.2020.12.12.CPD1
Myser, C., Kerridge, I. H., & Mitchell, K. R. (1995). Teaching clinical ethics as a professional skill: Bridging the gap between knowledge about ethics and its use in clinical practice. Journal of Medical Ethics, 21(2), 97–103. https://doi.org/10.1136/jme.21.2.97
Nordby, H., & Nøhr, Ø. (2012). The ethics of resuscitation: How do paramedics experience ethical dilemmas when faced with cancer patients with cardiac arrest? Prehospital and Disaster Medicine, 27(1), 64–70. https://doi.org/10.1017/S1049023X1200026X
O’Meara, P., & Duthie, S. (2018). Paramedicine in Australia and New Zealand: A comparative overview. The Australian Journal of Rural Health, 26(5), 363–368. https://doi.org/10.1111/ajr.12464
Olick, R. S. (2001). It’s ethical, but is it legal? Teaching ethics and law in the medical school curriculum. The Anatomical Record, 265(1), 5–9. https://doi.org/10.1002/ar.1035
Paramedicine Board of Australia. (2018). Code of Conduct for registered health practitioners (interim), June 2018. Retrieved November 30, 2021, from https://www.paramedicineboard.gov.au/Professional-standards/Codes-guidelines-and-policies.aspx
Paramedicine Board of Australia. (2020). Accreditation Standards: Paramedicine. Retrieved November 30, 2021, from https://www.paramedicineboard.gov.au/Accreditation/Accreditation-publications-and-resources.aspx
Paramedicine Board of Australia. (2021a). About. Retrieved November 29, 2021, from https://www.paramedicineboard.gov.au/About.aspx
Paramedicine Board of Australia. (2021b). Professional capabilities for registered paramedics. Retrieved November 30, 2021, from https://www.paramedicineboard.gov.au/Professional-standards/Professional-capabilities-for-registered-paramedics.aspx
Savulescu, J., Crisp, R., Fulford, K. W., & Hope, T. (1999). Evaluating ethics competence in medical education. Journal of Medical Ethics, 25(5), 367–374. https://doi.org/10.1136/jme.25.5.367
Scher, S., & Kozlowska, K. (2018). Rethinking Health Care Ethics. Palgrave Macmillan. https://doi.org/10.1007/978-981-13-0830-7#toc
Shearer, K., Thomas, M., & Signal, T. (2021). Perceptions of ethical dilemmas in Australian paramedicine. Journal of Paramedic Practice, 13(8), 332–342. https://doi.org/10.12968/jpar.2021.13.8.332
Souza, A., & Vaswani, V. (2020). Diversity in approach to teaching and assessing ethics education for medical undergraduates: A scoping review. Annals of Medicine and Surgery, 56, 178–185. https://doi.org/10.1016/j.amsu.2020.06.028
Stirrat, G. (2010). Teaching and learning medical ethics and law in UK medical schools. Clinical Ethics, 5(3), 156–158. https://doi.org/10.1258/ce.2010.010029
Torda, A., & Mangos, J. (2020). Medical ethics education in Australian and New Zealand (ANZ) medical schools: a mixed methods study to review how medical ethics is taught in ANZ medical programs. International Journal of Ethics Education, 5(2), 211–224.
Victorian Legal Admissions Board. (2021). Academic Qualifications and Training. Retrieved December 1, 2021, from https://www.lawadmissions.vic.gov.au/qualifications-and-training/academic
Acknowledgements
The first author would like to acknowledge the Australian Government Research Training Program, which has provided a tuition offset.
Author information
Authors and Affiliations
Contributions
Kirsty Shearer, Matthew Thomas, Tania Signal, and Nikola Stepanov contributed to the study conception and design. Material preparation, data collection and analysis were performed by Kirsty Shearer. The first draft was written by Kirsty Shearer and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics Approval
The study was approved by the HREC of CQUniversity Australia (0000022092). Academics participating in discussions were emailed an information sheet and consent form, with consent to participate verbally confirmed prior to any discussion.
Competing Interests
Kirsty Shearer was appointed as a paid Accreditation Assessor with the Paramedicine Board of Australia during the data collection phase of this study. Matthew Thomas, Tania Signal, Ruth Townsend and Nikola Stepanov have no competing interests to declare.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Shearer, K., Thomas, M., Signal, T. et al. Undergraduate Ethics Education in Paramedicine in Australia. J Acad Ethics 21, 377–392 (2023). https://doi.org/10.1007/s10805-022-09463-3
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10805-022-09463-3