
Abstract
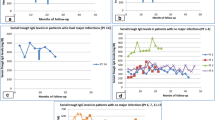
Outcome of patients with X-linked agammaglobulinemia (XLA) has improved with the widespread use of immunoglobulin replacement therapy (IgRT). There are few data on the spectrum of infections experienced by patients undergoing IgRT. We carried out a retrospective cross-sectional analysis of the records of XLA patients seen at Necker-Enfants Malades Hospital, Paris. For each infection, we evaluated infection site, microbial etiology, antibiotic prophylaxis, immunosuppressive treatment, IgRT route, and last known IgG trough level. Sixty patients were included, who cumulated a follow-up of 1470 patient-years. We recorded 188 infections, including 97 after initiation of IgRT. The rate of infection was highest before IgRT (0.66 vs. 0.06 per person-year (ppy), p < 0.001) and was higher after the age of 16 compared to before (0.14 vs. 0.05 ppy, p = 0.048). It was similar for patients receiving intravenous or subcutaneous Ig (0.09 vs 0.05 ppy, p = 0.54). The lungs and gastrointestinal tract accounted for 71% of infection sites. Forty-six (47%) infections occurred in patients receiving antibiotic prophylaxis. Sixteen (16.5%) infections occurred in patients receiving immunosuppressive therapy, which more frequently occurred after age 16 (35% vs. 2.4%, p < 0.001). The median IgG trough level prior to all infections was 8.4 g/L. Almost half (44.3%) of infections occurred with prior IgG trough levels > 8 g/L, and 16/97 (16.7%) in patients with trough levels > 10 g/L. Infection remains a significant issue in patients with XLA undergoing IgRT despite adequate IgG trough levels. Chronic inflammatory manifestations of X-linked agammaglobulinemia and immunosuppressive therapies may be significant drivers of infection during adulthood.


Similar content being viewed by others

Data Availability
Data are available on request
Code Availability
Not applicable
References
Conley ME, Rohrer J, Minegishi Y. X-linked agammaglobulinemia. Clin Rev Allergy Immunol. 2000;19:183–204.
Winkelstein JA, Conley ME, James C, Howard V, Boyle J. Adults with X-linked agammaglobulinemia: impact of disease on daily lives, quality of life, educational and socioeconomic status, knowledge of inheritance, and reproductive attitudes. Medicine (Baltimore). 2008;87:253–8.
Aguilar C, Malphettes M, Donadieu J, et al. Prevention of infections during primary immunodeficiency. Clin Infect Dis. 2014;59:1462–70.
Howard V, Greene JM, Pahwa S, et al. The health status and quality of life of adults with X-linked agammaglobulinemia. Clin Immunol. 2006;118:201–8.
Lougaris V, Soresina A, Baronio M, et al. Long-term follow-up of 168 patients with X-linked agammaglobulinemia reveals increased morbidity and mortality. J Allergy Clin Immunol. 2020;146:429–37.
Seidel MG, Kindle G, Gathmann B, et al. The European Society for Immunodeficiencies (ESID) registry working definitions for the clinical diagnosis of inborn errors of immunity. J Allergy Clin Immunol Pract. 2019;7:1763–70.
Cellier C, Foray S, Hermine O. Regional enteritis associated with enterovirus in a patient with X-linked agammaglobulinemia. N Engl J Med. 2000;342:1611–2.
Frémond M-L, Pérot P, Muth E, et al. Next-generation sequencing for diagnosis and tailored therapy: a case report of astrovirus-associated progressive encephalitis. J Pediatric Infect Dis Soc. 2015;4:e53-57.
Etienne N, Bret L, Le Brun C, et al. Disseminated spiroplasmaapis infection in patient with agammaglobulinemia, France. Emerg Infect Dis. 2018;24:2382–6.
Degand N, Dautremer J, Pilmis B, et al. Helicobacter bilis-associated suppurative cholangitis in a patient with X-linked agammaglobulinemia. J Clin Immunol. 2017;37:727–31.
Martínez-García MÁ, de Gracia J, VendrellRelat M, et al. Multidimensional approach to non-cystic fibrosis bronchiectasis: the FACED score. Eur Respir J. 2014;43:1357–67.
Winkelstein JA, Marino MC, Lederman HM, et al. X-linked agammaglobulinemia: report on a United States registry of 201 patients. Medicine (Baltimore). 2006;85:193–202.
Bearden D, Collett M, Quan PL, Costa-Carvalho BT, Sullivan KE. Enteroviruses in X-linked agammaglobulinemia: update on epidemiology and therapy. J Allergy Clin Immunol Pract. 2016;4:1059–65.
Janssen R, Krogfelt KA, Cawthraw SA, van Pelt W, Wagenaar JA, Owen RJ. Host-pathogen interactions in Campylobacter infections: the host perspective. Clin Microbiol Rev. 2008;21:505–18.
Pac M, Bernatowska EA, Kierkuś J, et al. Gastrointestinal disorders next to respiratory infections as leading symptoms of X-linked agammaglobulinemia in children - 34-year experience of a single center. Arch Med Sci. 2017;13:412–7.
Dion J, Malphettes M, Bénéjat L, et al. Campylobacter infection in adult patients with primary antibody deficiency. J Allergy Clin Immunol Pract. 2019;7(1038–1041):e4.
El-Sayed ZA, Abramova I, Aldave JC, et al. X-linked agammaglobulinemia (XLA): phenotype, diagnosis, and therapeutic challenges around the world. World Allergy Organ J. 2019;12:100018.
Barmettler S, Otani IM, Minhas J, et al. Gastrointestinal manifestations in X-linked agammaglobulinemia. J Clin Immunol. 2017;37:287–94.
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Paccoud, O., Mahlaoui, N., Moshous, D. et al. Current Spectrum of Infections in Patients with X-Linked Agammaglobulinemia. J Clin Immunol 41, 1266–1271 (2021). https://doi.org/10.1007/s10875-021-01043-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10875-021-01043-1