
Abstract
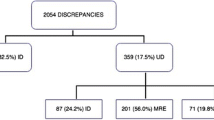
Background Medication reconciliation is a key tool in the prevention of adverse drug events. Objective To assess the impact of an electronic reconciliation tool in decreasing unintended discrepancies between medications prescribed after surgery and the patient’s usual treatment. Setting General Surgery Department of Gregorio Marañón’s University General Hospital, Madrid. Method A pre-post intervention study with no equivalent control group was carried out between June 2009 and December 2010. Patients hospitalized in the General Surgery Department for 24 h or more, and whose prescriptions prior to admission included three or more drugs were included in the study. Patients were interviewed to gather information about their usual treatment drugs. Discrepancies between the latter and the drugs prescribed after surgery were assessed before and after the medication reconciliation electronic tool was implemented. Main outcome measure Proportion of patients with at least one unintended discrepancy. Results A total of 107 patients in the pre-intervention phase and 84 patients in the post-intervention phase were included. We detected 1,678 discrepancies, 167 were found to be unintended. The number of patients with at least one unintended discrepancy was 43 (40.2 %) in the pre-intervention phase, and 38 (38.1 %) in the post-intervention phase, p = 0.885. The percentage of unintended discrepancies over the total amount of drugs reconciled was lower in the post-intervention phase than in the pre-intervention phase (6.6 vs. 10.6 %), p = 0.002. Regarding unintended discrepancies 79.2 % were grade C severity (the error reached the patient but caused no harm), 13.6 % grade D (the error reached the patient and required monitoring or intervention to preclude harm) and 7.1 % grade E (the error may have contributed to or resulted in temporary harm to the patient and required intervention). Conclusion Implementation of an electronic tool facilitated the process of medication reconciliation in a general surgery unit. The proportion of unintended discrepancies over the total amount of drugs reconciled was reduced after the implementation of the reconciliation programme. However, we could not demonstrate a more significant impact due to some methodological limitations.

Similar content being viewed by others


References
Gleason KM, Groszek JM, Sullivan C, Rooney D, Barnard C, Noskin GA. Reconciliation of discrepancies in medication histories and admission orders of newly hospitalized patients. Am J Health Syst Pharm. 2004;61:1689–95.
Joint Commission on Accreditation of Healthcare Organization. National Patient Safety Goals. 2014 (document on the internet). JCAHO; 2012 (cited 2014 Aug 3). http://www.jointcommission.org/assets/1/6/HAP_NPSG_Chapter_2014.pdf.
World Health Organization (WHO) Collaborating Centre for Patient Safety Solutions. Assuring Medication Accuracy at Transitions in Care (document on the internet). Geneve: World Health Organization; 2007 (cited 2014 July 31). http://www.who.int/patientsafety/solutions/patientsafety/PS-Solution6.pdf.
National Institute for Health and Clinical Excellence (NICE) and the National Patient Safety Agency (NSPA). Technical patient safety solutions for medicines reconciliation on admission of adults to hospital (document on the internet). NICE & NSPA; 2007 (cited 2014 July 25). http://www.nice.org.uk/guidance/psg001/resources/full-guidance-pdf2 ISBN: 1-84629-563-7.
Institute for Healthcare Improvement (IHI). Getting started kit: Prevention of adverse drug events. Medication reconciliation. How to guide (document on the internet). IHI; 2007 (cited 2014 July 25). http://www.wapatientsafety.org/downloads/Medication_ReconADEGuideIHI.pdf.
Rozich JD, Resar RK. Medication safety: one organization’s approach to the challenge. J Clin Outcomes Manag. 2001;8:27–34.
Delgado Sánchez O, Jimenez Anoz LA, Fabia AS, Pico JN. Conciliación de la medicación. Med Clin (Barc). 2007;129:343–8.
Lessard S, DeYoung J, Vazzana N. Medication discrepancies affecting senior patients at hospital admission. Am J Health Syst Pharm. 2006;63:740–3.
Delate T, Chester EA, Stubbings TW, Barnes CA. Clinical outcomes of a home based medication reconciliation program after discharge from a skilled nursing facility. Pharmacotherapy. 2008;28:444–52.
Crotty M, Rowett D, Spurling L, Giles LC, Phillips PA. Does the addition of a pharmacist transition coordinator improve evidence-based medication management and health outcomes in older adults moving from the hospital to a long care facility? Results of a randomized, controlled trial. Am J Geriatr Pharmacother. 2004;2:25–64.
Rozich JD, Howard RJ, Justeson JM, Macken PD, Lindsay ME, Resar RK. Standardization as a mechanism to improve safety in health care. Jt Comm J Qual Patient Saf. 2004;30:5–14.
Koehler BE, Richter KM, Youngblood L, Cohen BA, Prengler ID, Cheng D, et al. Reduction of 30-day postdischarge hospital readmission or emergency department (ED) visit rates in high risk elderly medical patients through delivery of a targeted care bundle. J Hosp Med. 2009;4:211–8.
Spinewine A, Claeys C, Foulon V, Chevalier P. Approaches for improving continuity of care in medication management: a systematic review. Int J Qual Health Care. 2013;25:403–17.
Tam VC, Knowles SR, Cornish PL, Fine N, Marchesano R, Etchells EE. Frequency, type and clinical importance of medication history errors at admission to hospital: a systematic review. Can Med Assoc J. 2005;173:510–5.
Anderson HJ. Medication reconciliation: what role will I.T. play? Health Data Manag. 2007; 15: 44, 46, 48.
Juvany R, Jódar R. Importance of medication reconciliation process for ensuring continuity and safety of patient care. Med Clin (Barc). 2012;139:672–3.
Giménez Manzorro Á, Zoni AC, Rodríguez Rieiro C, Durán-García E, Trovato López AN, Pérez Sanz C, et al. Developing a programme for medication reconciliation at the time of admission into hospital. Int J Clin Pharm. 2011;33:603–9.
Delgado Sánchez O, Martínez López I, Crespí Monjo M, Serra Soler G. Conciliación de la medicación: asumamos la responsabilidad compartida. Farm Hosp. 2008;32:63–4.
Giménez Manzorro Á, Trovato López AN, Romero Jiménez RM, Herranz Alonso A, Durán García ME, Planelles López MJ, et al. Herramienta electrónica para la conciliación de la medicación en el ingreso hospitalario. Aten Farm. 2012;14:393–400.
The National Coordinating Council for Medication Error Reporting and Prevention (NCC MERP). NCC MERP index for categorizing medication errors (document on internet). NCC MERP; 2001 (cited 2014 Dec 9). http://www.nccmerp.org/sites/default/files/indexColor2001-06-12.pdf.
Cornish PL, Knowles SR, Marchesano R, Tam V, Shadowitz S, Juurlink DN, et al. Unintended medication discrepancies at the time of hospital admission. Arch Intern Med. 2005;165:424–9.
Michels RD, Meisel SB. Program using pharmacy technicians to obtain medication histories. Am J Health Syst Pharm. 2003;60:1982–6.
Roure Nuez C, González Navarro M, González Valdivieso J, Fuster Barrera M, Broto Sumalla A, Sarlé Rubí J, et al. Efectividad de un programa de conciliación perioperatoria de la medicación crónica en pacientes de cirugía programada. Med Clin (Barc). 2012;139:662–7.
Schnipper JL, Hamann C, Ndumele CD, Liang CL, Carty MG, Karson AS, et al. Effect of an electronic medication reconciliation application and process redesign on potential adverse drug events: a cluster-randomized trial. Arch Intern Med. 2009;169:771–80.
Agrawal A, Wu WY. Reducing medication errors and improving systems reliability using an electronic medication reconciliation system. Jt Comm J Qual Patient Saf. 2009;35:106–14.
Agrawal A, Wu W, Khachewatsky I. Evaluation of an electronic medication reconciliation system in inpatient setting in an acute care hospital. Stud Health Technol Inform. 2007;129:1027–31.
García Ramos SE, Santolaya Perrín R. Conciliación de la medicación que se produce en el ingreso hospitalario. Atem Farm. 2012;14:7–17.
Hellström LM, Bondesson A, Hoglund P, Eriksson T. Errors in medication history at hospital admission: prevalence and predicting factors. BMC Clin Pharmacol. 2012;12:9.
Gleason KM, McDaniel MR, Feinglass J, Baker DW, Lindquist L, Liss D, et al. Results of the Medications at Transitions and Clinical Handoffs (MATCH) study: an analysis of medication reconciliation errors and risk factors at hospital admission. J Gen Intern Med. 2010;25:441–7.
Zoni AC, Durán García ME, Jiménez Muñoz AB, Salomón Pérez R, Martin P, Herranz Alonso A. The impact of medication reconciliation program at admission in an internal medicine department. Eur J Intern Med. 2012;23:696–700.
Orti SM, Company ES, Milla AR, Piqueres RF, Castillo JRD, Tarin IO. Results of a medication reconciliation project in routine medical treatment after surgical discharge. Cir Esp. 2007;82:333–7.
Kwan JL, Lo L, Sampson M, Shojania KG. Medication reconciliation during transitions of care as a patient safety strategy: a systematic review. Ann Intern Med. 2013;158:397–403.
Pippins JR, Gandhi TK, Hamann C, Ndumele CD, Labonville SA, Diedrichsen EK, et al. Classifying and predicting errors of inpatient medication reconciliation. J Gen Intern Med. 2008;23:1414–22.
Cohen V, Jellinek SP, Likourezos A, Nemeth I, Paul T, Murphy D. Variation in medication information for elderly patients during initial interventions by emergency department physicians. Am J Health Syst Pharm. 2008;65:60–4.
Agrawal A. Medication errors: prevention using information technology systems. Br J Clin Pharmacol. 2009;67:681–6.
Tschannen D, Talsma A, Reinemeyer N, Belt C, Schoville R. Nursing medication administration and workflow using computerized physician order entry. Comput Inform Nurs. 2011;29:401–10.
Acknowledgments
We thank every participant team (Preventive Medicine and Quality Assessment, General Surgery and Pharmacy staff) for their cooperation. We are grateful for their interest and help in the development of the programme.
Funding
The project was funded through a collaborative agreement between the Spanish Ministry of Health and Social Policy and the authorities of the Autonomous Region of Madrid, which aims to foster safe practices in the region’s healthcare facilities.
Conflicts of interest
The authors declare that there are no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Appendix
Rights and permissions
About this article

Cite this article
Giménez-Manzorro, Á., Romero-Jiménez, R.M., Calleja-Hernández, M.Á. et al. Effectiveness of an electronic tool for medication reconciliation in a general surgery department. Int J Clin Pharm 37, 159–167 (2015). https://doi.org/10.1007/s11096-014-0057-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11096-014-0057-0