
Abstract
The coronavirus (COVID-19) pandemic is currently a global health threat attributed to negatively affecting the mental health and well-being of people globally. The purpose of the present study is to examine the mediating role of optimism-pessimism and psychological inflexibility in the relationship of coronavirus stress with psychological problems among Turkish adults. The sample of the study included 451 adults (55% women). Participants mainly consisted of young adults with a mean age of 23.30 years, ranging from 18 to 65 years (SD = 6.97). A mediation model indicated that coronavirus stress had a significant predictive effect on optimism-pessimism, psychological inflexibility, and psychological problems. Further, optimism-pessimism and psychological inflexibility mediated the effect of coronavirus stress on psychological problems in adults. Lastly, optimism-pessimism predicted the psychological problems of adults through psychological inflexibility. These results elucidate our understanding of the role of mediators in coronavirus stress and psychological health problems. The findings are useful in terms of providing evidence for tailoring interventions and implementing preventative approaches to mitigate the psychopathological consequences of COVID-19. Based on the present findings, the potential utility of acceptance and commitment therapy is discussed within the context of COVID-19.
Similar content being viewed by others

According to the World Health Organization (WHO), severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), also known as novel coronavirus, causes coronavirus disease 2019 (COVID-19) (WHO 2020). Fever, cough, and shortness of breath are among the most well-documented symptoms. The COVID-19 outbreak rapidly emerged as a worldwide pandemic and within a short period of time caused economic disruption, job loss, financial hardship, and social isolation. Many people experienced stress as a natural response to the adversity. Across the world, many clinical studies have been conducted to discover a vaccine for COVID-19, yet the impact on mental health and associated interventions and services remains largely understudied. The reported increase in mental health issues due to physical distancing, quarantining processes, and social isolation makes further research in this area critical in order to systematically investigate, understand, and tailor appropriate interventions (Harper et al. 2020; Satici et al. 2020; Tanhan et al. 2020). In Turkey, the first COVID-19 case was diagnosed on March 11, and as of May 6, the confirmed total statistics related to COVID-19 include 131,744 diagnosed cases, 3584 deaths, 78,202 recoveries, and 12,347,024 tests (Turkish Ministry of Health 2020).
COVID-19 is a health threat identified as a significant stressor threatening the mental health and well-being of many individuals around the world (Brooks et al. 2020; Bhuiyan et al. 2020; Satici et al. 2020). It has been suggested that COVID-19 stress can trigger mild to severe levels of psychosocial problems, such as depression, somatization, and anxiety (Arslan and Yıldırım 2020; Bhuiyan et al. 2020; Gunnell et al. 2020; Satici et al. 2020). Recent reports have demonstrated that people have suffered from serious social and mental health problems including depression and anxiety (Bao et al. 2020; Çiçek et al. 2020; Wang et al. 2020), poor psychological health (Yildirim and Arslan 2020), suicide (Gunnell et al. 2020; Bhuiyan et al. 2020; Mamun and Griffiths 2020), posttraumatic stress disorders (Bao et al. 2020), burnout among health care professionals (Chen et al. 2020), psychological inflexibility (Çiçek et al. 2020), physical isolation and loneliness (Tanhan et al. 2020; Zandifar and Badrfam 2020), behavioral problems (Cortese et al. 2020), and negative consequences associated with spending excessive time on the internet (Çiçek et al. 2020). These responses to COVID-19 could lead to chronic psychopathology and affect a large number of people if problems are not identified, acknowledged, and treated effectively. Mental health researchers have called for urgent and rigorous research that can address mental health problems and provide concrete solutions for the prevention of emerging problems associated with COVID-19 (Liu et al. 2020; Tanhan et al. 2020; Wang et al. 2020; Yao et al. 2020). In order to provide appropriate mental health services and develop prevention and intervention strategies for people in response to COVID-19, it is critical to understand the mitigating factors associated with coronavirus stress and psychological problems. Thus, the purpose of the present study is to examine the mediating role of optimism-pessimism and psychological inflexibility on the relationship between coronavirus stress and psychological problems among Turkish adults.
Optimism-Pessimism and Mental Health
Stressful life events, such as those instigated by the coronavirus pandemic, have significant influence on an individual’s psychological functioning and well-being, and can be a catalyst for psychological problems including anxiety, confusion, social withdrawal, and depression (Ingram and Luxton 2005; Yildirim and Arslan 2020). Although the experience of coronavirus stress may have a negative impact on the mental health and well-being of some individuals, this might not be the case for all people. Individual differences in resilience, coping and perceptions may influence how a person responds to adversarial experiences. Optimism and pessimism are conceptualized as important constructs in coping with uncontrollable life events (Nes 2016). Optimism-pessimism is considered to be a generalized version of the confidence-doubt dichotomy pertaining to life in general, rather than to just a specific issue (see Carver et al. 2010). It has received attention in recent years due to the growing field of positive psychology (Woldgabreal et al. 2016). Carver et al. (2010) defined optimism as an individual difference variable that reflects the extent to which people hold generalized favorable expectancies for their future. Optimism and pessimism are stable personality characteristics that have important implications for regulating one’s behaviors. Optimism has been associated with a person’s expectancies of good and bad outcomes (Scheier and Carver 1985).
Previous studies have indicated that optimism is associated with adaptive outcomes and well-being, such as life satisfaction, positive affectivity, self-esteem, and flourishing (Duy and Yildiz 2017; Gallagher and Lopez 2009; Karademas 2006; Peterson and Chang 2003; Sapmaz and Doğan 2012; Scheier et al. 2001), whereas pessimism has been found to correlate with maladaptive outcomes, such as depression and anxiety (Andersson 1996; Chang and Sanna 2001; Kwok and Gu 2017; Scheier and Carver 1992; Vickers and Vogeltanz 2000). For example, Carver et al. (2010) found that higher levels of optimism were related to better subjective well-being in times of adversity. Optimism enhances people’s motivation to pursue goal-oriented behaviors (Scheier and Carver 1985), physical health (Carver et al. 2010), and positive adjustment to college, and also decreases psychological problems (Scheier et al. 1994). Optimistic individuals have also been reported to employ greater problem-focused strategies, which contribute to better adjustment and functioning in the face of negative life events compared with those who are pessimistic (Nes 2016; Taylor and Armor 1996). Nes and Segerstrom (2006) found an association between optimism and adaptive coping strategies contributing to the management, reduction, and elimination of negative effects associated with stress. Similarly, optimism was negatively related to maladaptive coping strategies including withdrawal, avoidance, or ignoring stressors. Optimists are expected to be confident and persistent in the face of diverse life challenges and pessimists are expected to have less confidence in similar situations. Optimists are able to adjust their coping strategies depending on the stressors (Nes and Segerstrom 2006; Reed 2016) and, thereby, they may experience more positive outcomes compared with pessimistic individuals.
Psychological Inflexibility and Mental Health
Understanding one’s own thoughts, feelings, and sensations is necessary to address psychopathology and promote well-being (Hayes et al. 2006; Hayes et al. 2012; Larson 2011; Tanhan 2019). Acceptance and commitment therapy (ACT) is considered to be a third-wave therapy that represents a multidimensional and functional contextual model that considers both well-being and psychopathology (Hayes et al. 2006; Hayes et al. 2012). From the ACT perspective, stress or pain is inevitable for all people and the psychopathology that emerges from psychological inflexibility can be intervened with (Hayes et al. 2006; Hayes et al. 2012; Tanhan 2019). Psychological inflexibility implies “the rigid dominance of psychological reactions, over chosen values and contingencies, in guiding action” (Bond et al. 2011, p. 678). Psychological inflexibility is a process in which a person portrays dysfunctional control efforts related to bodily sensations, feelings, or thoughts to avoid experiencing unpleasant internal or external events. This process may worsen an individual’s internal and external experience of a negative experience (Bond et al. 2011; Levin et al. 2014; Tanhan 2019). Six core psychological inflexibility processes have been described: experiential avoidance, inflexible attention, disrupted values, inaction or impulsivity, conceptualized self, and cognitive fusion (Hayes et al. 2006, 2012; Tanhan 2019). Psychological inflexibility can develop into psychopathology when a person experiences one or more of these six core processes excessively or for a prolonged period of time (Hayes et al. 2006; Hayes et al. 2012). An individual with high psychological inflexibility is thought to approach stressful situations as rigid and reactive rather than meaningful, mindful, and value-driven (Arslan and Allen 2020). Therefore, psychologically inflexibility may contribute to the development of psychological, behavioral, and social problems.
Psychological inflexibility is a construct associated with the development and maintenance of a wide range of psychological problems. Previous studies have indicated the association between the restrictive nature of psychological inflexibility and various psychological problems, including somatization, depression, anxiety, and posttraumatic stress symptoms (Dick et al. 2014; Harris 2009; Masuda and Tully 2012). Levin et al. (2014) reported that psychological inflexibility was significantly associated with a range of current and lifetime psychological and behavioral problems (e.g., depressive symptoms, anxiety, and eating disorders). Similarly, Woodruff et al. (2014) reported the significant predictive effect of psychological inflexibility on positive and negative psychological health indicators, such as depression, unhappiness, positive affect, and life satisfaction. The literature also supports the mediating role of psychological inflexibility between different constructs, such as maladaptive schemas and depression, help-seeking and stigma (e.g., Crosby et al. 2011; Gaudiano et al. 2017; Kurz et al. 2014; Mendoza et al. 2018). For example, Yadavaia et al. (2014) reported that psychological inflexibility was a mediator of change in self-compassion, anxiety, depression, stress, and general psychological distress. Uğur et al. (2020) found that psychological inflexibility mediated the relationship between fear of negative evaluation and psychological vulnerability. Psychological inflexibility has also been found to mediate the relationship between depression severity and stigma toward others with depression (Gaudiano et al. 2017).
Although the importance of examining the relationship between psychological inflexibility and optimism has been highlighted (Woldgabreal et al. 2016), few studies have focused on the association between these variables. Thus, there is need to advance research in this area. Towsyfyan and Hossein Sabet (2017) emphasized the effectiveness of ACT on increased optimism for the people with major depressive disorders as well as the importance of high psychological flexibility for increased optimism (Woldgabreal et al. 2016). High psychological inflexibility is more likely to be related to higher levels of pessimism (Masuda and Latzman 2011). Psychologically flexible individuals are able to manage and adjust their feelings and thoughts in a productive and psychologically adaptive way, and this characteristic can positively influence optimism in the face of stressors. Therefore, psychological inflexibility may be an important mechanism in enhancing optimism and decreasing pessimism by mitigating the negative effects of coronavirus stress on these constructs.
Purpose of the Paper
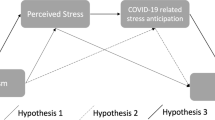
Given the theoretical and empirical evidence presented above, the purpose of the current study was to examine the mediating effects of the optimism-pessimism and psychological inflexibility on the association of coronavirus stress with psychological problems among Turkish adults. Prior to testing the mediation model, we first examined the psychometric properties of the Coronavirus Stress Measure (CSM) to enhance the scale’s usability for both research and practice using the sample of the present study. Subsequently, we addressed the following research hypotheses: (H1) psychological inflexibility would mediate the negative impacts of coronavirus stress on adults’ optimism and pessimism; (H2) optimism and pessimism would mediate the association of psychological inflexibility with psychological problems; and (H3) optimism, pessimism, and psychological inflexibility together would mediate the association between coronavirus stress and psychological problems among adults. Given the literature indicating the impacts of the coronavirus pandemic on individuals’ mental health and functioning, to understand the factors that help explain the association between coronavirus stress and psychological problems is critical to developing prevention and intervention strategies for adults. Findings of this study will therefore provide important implications and directions for current and future approaches to prevention and intervention.
Method
Participants
The sample of the present study comprised 451 adults. Participants mainly included young people with a mean age of 23.30 years, ranging from 18 to 65 years (SD = 6.97). Slightly more than half of the sample consisted of women (55%). The majority of participants were of an average socioeconomic level (75%) and held a university diploma (91%). An online survey was created using demographic items and the measures of the study. Institutional review board approval was obtained prior to the data collection process and the participants were informed that participation in the study was voluntary, the survey was confidential, and they could withdraw from the survey at any time if they did not want to continue. Additionally, an electronic assent form was signed by adults who volunteered to participate in the study.
Measures
Coronavirus Stress
The Coronavirus Stress Measure (CSM) was adapted from the 14-item perceived stress scale (PSS, Cohen et al. 1983) to assess COVID-19 related to stress. The CSM included eight items with scoring based on a 5-point Likert type scale, ranging between 0 = never and 4 = very often (e.g., “In the last month due to coronavirus, how often have you felt that you were unable to control the important things in your life?”). The psychometric properties of the CSM were examined with the present sample to enhance the usability of the scale for use in research and practice, as shown in the “Results” section.
Optimism and Pessimism
The Optimism and Pessimism Measure (OPM) is a 12-item self-report rating scale developed to assess optimism and pessimism among Turkish youths and adults (Arslan and Yıldırım 2020). All items are rated using a 5-point Likert type scale, ranging from 1 = strongly disagree to 5 = strongly agree (e.g., “I can’t be happy with anything, I’m a pessimistic person,” I hope many things will be better in the future”). Previous research indicated that the scales had strong internal reliability estimates (Arslan and Yıldırım 2020).
Psychological Inflexibility
Psychological inflexibility was assessed using the Acceptance and Action Questionnaire–II, which is a 7-item self-report scale developed to assess psychological inflexibility and experiential avoidance (Bond et al. 2011). All items of the scale are scored based on a 7-point Likert type scale, ranging from 1 = never true to 7 = always true (e.g., “My painful experiences and memories make it difficult for me to live a life that I would value”). Yavuz et al. (2016) investigated the psychometrics of the scale with a Turkish sample, indicating a strong internal and test-retest reliability estimate.
Psychological Problems
The Brief Symptom Inventory (BSI-18) was used to assess adults’ psychological problems (Derogatis and Fitzpatrick 2004). The BSI is an 18-item self-report measure, comprising six-item subscales: depression, anxiety, and somatization (e.g., “Feeling no interest in things,” “Pains in heart or chest”). All items are responded to using a 5-point Likert type scale, ranging from not at all (0) to very much (4). The scale and its subscales have had strong internal reliability estimates for a Turkish sample (Arslan and Yıldırım 2020).
Data Analyses
Prior to testing the structural models, preliminary analyses were conducted including descriptive statistics, analysis assumptions, internal reliability (α) estimates, and correlation analysis. First, skewness and kurtosis values fall within |2| range, indicating that the variables of the study were fairly normally distributed (D’Agostino et al. 1990; Field 2009). Subsequently, we established measurement models to examine factor structure of the measures using a series of exploratory factor analysis (EFA) and confirmatory factor analysis (CFA) models. The EFA and CFA models were run via psych (Revelle 2019) and lavaan (Rosseel 2012) R packages. First, the factor structure of CSM (8 items) was explored using the EFA and then confirmed using the CFA. The CFA was conducted to examine the factor structure of psychological inflexibility, optimism-pessimism, and psychological problems. Finally, we examined the hypothesized structural mediation model and obtained estimates and their bootstrap standard errors via lavaan R package (Rosseel 2012) with DWLS estimation option. Findings from the hypothesized structural mediation and measurement model were interpreted using common data-model indices and their cut-points: Tucker-Lewis index (TLI) and comparative fit index (CFI) ≥ .90 = adequate and ≥ .95 = close data-model fit, standardized root mean square residual (SRMR) and root mean square error of approximation (RMSEA) ≤ .10 = acceptable, ≤ .08 = adequate, and ≤ .05 = good data-model fit (Hu and Bentler 1999; Kline 2015).
Results
Preliminary Analysis
Preliminary analysis results showed that the variables of the study had skewness values ranging from − .42 to 1.19, and kurtosis values ranging from − .70 to 1.02, indicating acceptable distributional properties for further analysis (absolute values less than 2). Cronbach alphas (α) reliability estimates were computed, as shown in Table 1. All scales had strong reliability estimate with the present sample, with α values ranging from .83 to .96.
Demographic variables were negatively correlated with maladaptive psychological constructs (MPCs: somatization, anxiety, depression, and overall psychological problems), meaning that being older, coming from higher socioeconomic background, or attaining higher degree were associated with lower values on MPCs.
Coronavirus stress (r range = − .27–.53) and pessimism (r range = .41–.60) were moderately and positively correlated with MPCs, meaning that having high level of stress or being pessimistic was associated with higher scores on MPCs, whereas optimism was moderately (but negatively) correlated with MPCs (r range = − .49–− .30). Psychological inflexibility was moderately and positively correlated with MPCs (r range = .37–.52), meaning that having a high score on psychological inflexibility is associated with higher scores on MPCs. Correlation analysis results are presented in Table 2.
Measurement and Structural Mediation Model
Consisting of eight items provisionally, the CSM was adapted from the 14-item PSS (Cohen et al. 1983), for which psychometric properties should be explored further. Theoretically, these eight items aim to represent a unidimensional construct. A series of EFA models were run on the CSM. Eigenvalues greater than one rule and scree and parallel plots all suggested two factors. One solution was to discard three items falling into one factor and continue with the remaining five, which could be sufficient for a unidimensional construct. The CFA models presented in Table 3 were run to justify the five-item CSM based on the EFA results. In the first model, all adapted items were included which produced relatively low standardized loadings on three suspected items (.15, .11, and .23). In the second model, three suspected items were excluded which leaves us with five items (standardized loadings ranging from .58 to .84). Results indicated that discarding three suspected items improved the model fit without jeopardizing the construct definition. Thus, the second model was retained with five items. Next, a series of the CFA models were conducted to examine the measurement model of optimism-pessimism, psychological inflexibility, and psychological problem constructs. Model fit indices for measurement models and their alternatives are presented in Table 3.
After validating the measurement models, a hypothesized structural model was constructed and is presented in Fig. 1. Despite marginally acceptable fit for some scales individually, combined together, the structural model provided good data-model fit statistics (χ2 (807) = 1862.280, p < .001, CFI = .991, TLI = .991, RMSEA = .055, and SRMS = .061). An RMSEA value between .05 and .10 indicates an acceptable fit (what Kline (2015) refers to as not-close-fit), whereas RMSEA < .05 would have indicated a good fit. This is also supported by combination rule, where TLI and CFI ≥ .95 and SRSR ≤ .08 suggests an acceptable fit (Hu and Bentler 1999).

The structural mediation model depicting relationship between psychological constructs (with standardized coefficients). **p < .01; ***p < .001. PP = psychological problems
Path coefficients were estimated both with the constrained (zero) and unconstrained error variance (negative) to check whether they were sensitive to alternative specifications. Parameters and their standard errors appeared to be robust to these two alternative specifications (they were nearly identical). For all effects in the mediation model, including direct and indirect effects, the bootstrap standard errors were used to test statistical significance (Preacher and Hayes 2008; Preacher and Hayes 2008). Unstandardized path coefficients and their 95% CI are presented in Table 4, and standardized coefficients are embedded in the Fig. 1.
Standardized path coefficients revealed that the effect of coronavirus stress on psychological problems was partially mediated through optimism, pessimism, and psychological inflexibility. Indirect effect estimates and their 95% CI and standardized coefficients are presented in Table 5.
Mediational pathways going through optimism significantly predicted psychological problems (β = .07, p < .01). Mediational pathways going through pessimism also significantly predicted psychological problems (β = .09, p < .001). Relatively stronger indirect effect was found through psychological inflexibility (β = .11, p < .001). Directly or indirectly, in total, experiencing coronavirus stress significantly predicted a moderate to large level of increase in psychological problems (β = .63, p < .001). Altogether, coronavirus stress, optimism, pessimism, and psychological inflexibility explained 59% of the variance in the psychological problems. There were also intermediary mediation effects. Coronavirus stress and psychological inflexibility significantly predicted optimism (β = − .22, p < .01 and β = − .27, p < .001, respectively). Directly and indirectly the variables explained 18% of the variation in optimism together. Coronavirus stress and psychological inflexibility also significantly predicted pessimism (β = − .17, p < .01 and β = .57, p < .001, respectively). Directly and indirectly the variables explained 44% of the variation in pessimism together.
Discussion
Globally, the COVID-19 pandemic has unprecedentedly caused a human health crisis. It has been responsible for a wide array of psychosocial problems, such as fear, anxiety, depression, stress, panic disorders, and social isolation. With regard to the psychometric properties of the newly adopted CSM, the results confirmed that the CSM is a valid and reliable measurement tool assessing COVID-19-related stress, demonstrating satisfactory internal consistency reliability estimate with Cronbach's alpha. The construct validity of the CSM confirms unidimensional structure comprising 5 items. The scale also showed good evidence of convergent validity with theoretically similar constructs such as anxiety and depression and divergent validity with demographic factors such as age. At the time of writing this manuscript, the COVID Stress Scale (CSM) was developed to measure COVID-19-related distress (Taylor et al. 2020). The CSM includes 36 items corresponding to 5 factors. Our scale is undoubtedly advantageous in terms of its brevity, administrability, and cost-effectiveness. These results also expanded the burgeoning literature on the pandemic specific measures such as Coronavirus Perceived Risk Scale (Yıldırım and Güler 2020), Fear of COVID-19 Scale (Ahorsu et al. 2020), and Coronavirus Anxiety Scale (Lee 2020). The CSM can be used in future studies aiming to examine stress-related factors within the context of COVID-19.
The subsequent purpose of this study was to examine the role of optimism-pessimism and inflexibility in elucidating the underlying mechanism between coronavirus stress and psychological problems during the pandemic. Specifically, this study aimed to provide more definitive evidence for tailoring and establishing interventions that contribute to effective coping with the crisis and reduced mental health problems. The results of the study generally support the mediating roles of optimism-pessimism and psychological inflexibility in the association between coronavirus stress and psychological problems. Consistent with previous studies, stress was found to correlate positively with pessimism (Britton et al. 2019), psychological inflexibility (Tavakoli et al. 2019), and psychological problems (Anniko et al. 2019) and correlate negatively with optimism (Britton et al. 2019). Although some prior research has investigated the role of mediators in stress and psychological health problems (e.g., Bargai et al. 2007) and well-being (e.g., Praharso et al. 2017), there is scarcity of research that has examined the mediating role of psychological inflexibility on the association between stress and optimism-pessimism. This study demonstrated that psychological inflexibility significantly mediated the negative impacts of coronavirus stress on adults’ optimism and pessimism. These results have supported the first hypothesis of the study and are congruent with earlier research on the association between inflexibility and optimism-pessimism (Levens and Gotlib 2012).
In support of the second prediction of our study, the results showed that optimism and pessimism significantly mediated the relationship of psychological inflexibility with psychological problems, suggesting that higher optimism and lower pessimism can reduce the negative impact of psychological inflexibility on the experience of psychological problems. Although research in this area is limited, the emerging findings are consistent with earlier studies on the association between optimism-pessimism, flexibility, and mental health. In a study, Reed (2016) investigated the mediating role of optimism between coping flexibility and psychological problems (e.g., stress) and well-being (e.g., life satisfaction). The results indicated that there were strong relationships between coping flexibility, optimism, psychological problems, and well-being. The interaction between coping flexibility and optimism explained a significant amount of the variance in both psychological problems and well-being. Additionally, optimism was found to partially mediate the relationship between coping flexibility and both psychological problems and well-being.
Importantly, optimism, pessimism, and psychological inflexibility together significantly mediated the relationship between coronavirus stress and psychological problems. These results suggest that the reason people with high levels of coronavirus stress report greater psychological problems is that they have high levels of psychological inflexibility and pessimism and lower levels of optimism. The theoretical underpinnings of this prediction are that stress may lead to greater psychological inflexibility and pessimism, and lower optimism which may in turn lead to greater psychological problems (Al Jarrah et al. 2019; Ingram and Luxton 2005; Levin et al. 2014; Yildirim and Alanazi 2018). High levels of optimism and low levels of psychological inflexibility and pessimism may help people to cope with coronavirus stress and foster lower levels of psychological problems.
With regard to the psychometric properties of the newly developed CSM, the results confirmed that the CSM is a valid and reliable measurement tool assessing COVID-19-related stress with as few as five items, demonstrating satisfactory internal consistency reliability estimate with Cronbach's alpha. The construct validity of the CSM confirms unidimensional structure. The scale also showed good evidence of convergent validity with theoretically similar constructs such as anxiety and depression and divergent validity with demographic factors such as age. The CSM can be used in future studies aiming to examine stress-related factors within the context of COVID-19.
Implication and Limitations
The present findings suggest the following recommendations for future studies and interventions. First, researchers, practitioners, health policymakers, and planners need to critically consider the prevention of mental illness by focusing on psychological resources including optimism and psychological flexibility. Second, psychological flexibility and optimism could help to reduce the impacts of coronavirus-related stress on the mental health and well-being of adults. Third, in light of evidence-based psychological therapies such as ACT, nationwide strategic planning and intervention for psychological first aid during the COVID-19 pandemic should be urgently developed and implemented. Such interventions can potentially be delivered online using social networking sites as they are fast, convenient, and cost-effective approaches in delivering planned interventions to the general public. The feasibility of such strategies during the COVID-19 pandemic have been successfully established in China with a high rate of success in addressing mental health problems among the general public and health care professionals (Liu et al. 2020).
This study has some limitations that need to be considered when interpreting the results. First, the data relied completely on self-reported measures which may prone to bias despite high reliability and validity of the selected measures. For example, participants could have given responses which included a tendency to either underreport or overreport socially desirable attitudes. Thus, to address this issue, future research should use multiple assessment techniques for the investigation of the associations among the study variables. Second, the present study had a cross-sectional design which cannot ascertain a causal relationship among the study variables. As such, great caution should be given to the interpretation of the results of mediation analysis on cross-sectional design. Subsequent studies using longitudinal and experimental designs need to be carried out which may have potential to offer additional insights into the associations between coronavirus stress, optimism-pessimism, psychological flexibility, and psychological problems. Finally, further research should be conducted to present more solid evidence and expand psychometric features of the CSM to wider populations such as clinical samples and adolescents. Establishing psychometric features of the CSM in diverse populations and context would contribute to reliability and validity of the scale to be applied in the field of mental health and other relevant fields.
In conclusion, these results add to the burgeoning literature suggesting that positive psychological resources, capabilities, and strengths such as optimism and psychological flexibility are key ingredients in contributing to positive mental health during a health crisis. These preliminary findings can be used to tailor and implement effective and efficient psychological health interventions to cope with challenges of COVID-19.
References
Ahorsu, D. K., Lin, C. Y., Imani, V., Saffari, M., Griffiths, M. D., & Pakpour, A. H. (2020). The Fear of COVID-19 Scale: development and initial validation. International Journal of Mental Health and Addiction. Advance online publication. https://doi.org/10.1007/s11469-020-00270-8.
Al Jarrah, F. N., Hamdan, F. R., Hamdan, M. R., Fraihat, A., & Alazzam, A. A. (2019). The level of optimism and pessimism and its relationship to the quality of life in patients with renal failure in the government and private hospitals in Irbid. International Journal of Psychological Studies, 11(2), 9–23.
Andersson, G. (1996). The benefits of optimism: a meta-analytic review of the Life Orientation Test. Personality and Individual Differences, 21(5), 719–725.
Anniko, M. K., Boersma, K., & Tillfors, M. (2019). Sources of stress and worry in the development of stress-related mental health problems: a longitudinal investigation from early-to mid-adolescence. Anxiety, Stress, & Coping, 32(2), 155–167.
Arslan, G., & Allen, K. (2020). Exploring the association between coronavirus stress, meaning in life, psychological flexibility, and subjective well-being. Submitted for publication.
Arslan, G., & Yıldırım, M. (2020). Coronavirus stress, meaningful living, optimism, and depressive symptoms: A study of moderated mediation model. Submitted for publication.
Bao, Y., Sun, Y., Meng, S., Shi, J., & Lu, L. (2020). 2019-nCoV epidemic: address mental health care to empower society. The Lancet, 395(10224), e37–e38. https://doi.org/10.1016/S0140-6736(20)30309-3.
Bargai, N., Ben-Shakhar, G., & Shalev, A. Y. (2007). Posttraumatic stress disorder and depression in battered women: the mediating role of learned helplessness. Journal of Family Violence, 22(5), 267–275.
Bhuiyan, A. K. M. I., Sakib, N., Pakpour, A. H., Griffiths, M. D., & Mamun, M. A. (2020). COVID-19-related suicides in Bangladesh due to lockdown and economic factors: case study evidence from media reports. International Journal of Mental Health Addiction. https://doi.org/10.1007/s11469-020-00307-y.
Bond, F. W., Hayes, S. C., Baer, R. A., Carpenter, K. C., Guenole, N., Orcutt, H. K., Waltz, T., & Zettle, R. D. (2011). Preliminary psychometric properties of the Acceptance and Action Questionnaire-II: a revised measure of psychological flexibility and acceptance. Behavior Therapy, 42, 676–688.
Britton, M., LaLonde, L., Oshio, A., & Taku, K. (2019). Relationships among optimism, pessimism, and posttraumatic growth in the US and Japan: focusing on varying patterns of perceived stressfulness. Personality and Individual Differences, 151, 109513.
Brooks, S. K., Webster, R. K., Smith, L. E., Woodland, L., Wessely, S., Greenberg, N., & Rubin, G. J. (2020). The psychological impact of quarantine and how to reduce it: rapid review of the evidence. The Lancet, 395(10227), 912–920. https://doi.org/10.1016/S0140-6736(20)30460-8.
Carver, C. S., Scheier, M. F., & Segerstrom, S. C. (2010). Optimism. Clinical Psychology Review, 30(7), 879–889. https://doi.org/10.1016/j.cpr.2010.01.006.
Chang, E. C., & Sanna, L. J. (2001). Optimism, pessimism, and positive and negative affectivity in middle-aged adults: a test of a cognitive-affective model of psychological adjustment. Psychology and Aging, 16(3), 524–531. https://doi.org/10.1037/0882-7974.16.3.524.
Chen, Q., Liang, M., Li, Y., Guo, J., Fei, D., Wang, L., He, L., Sheng, C., Cai, Y., Li, X., Wang, J., & Zhang, Z. (2020). Mental health care for medical staff in China during the COVID-19 outbreak. The Lancet Psychiatry, 7(4), e15–e16. https://doi.org/10.1016/S2215-0366(20)30078-X.
Çiçek, I., Tanhan, A., Bulus, M., & Arslan, G. (2020). Psychological inflexibility predicts depression and anxiety during COVID-19: acceptance and commitment therapy perspective. Submitted for publication.
Cohen, S., Kamarck, T., & Mermelstein, R. (1983). A global measure of perceived stress. Journal of Health and Social Behavior, 24, 386–396.
Cortese, S., Asherson, P., Sonuga-Barke, E., Banaschewski, T., Brandeis, D., Buitelaar, J., Coghill, D., Daley, D., Danckaerts, M., Dittmann, R. W., Doepfner, M., Ferrin, M., Hollis, C., Holtman, M., Konofal, E., Lecendreux, M., Santosh, P., Rothenberger, A., Soutullo, C., Steinhausen, H. C., Taylor, E., Van der Oord, S., & Zuddas, A. (2020). ADHD management during the COVID-19 pandemic: guidance from the European ADHD Guidelines Group. The Lancet Child & Adolescent Health., 4, 412–414. https://doi.org/10.1016/S2352-4642(20)30110-3.
Crosby, J. M., Bates, S. C., & Twohig, M. P. (2011). Examination of the relationship between perfectionism and religiosity as mediated by psychological inflexibility. Current Psychology, 30(2), 117–129. https://doi.org/10.1007/s12144-011-9104-3.
D’Agostino, R. B., Belanger, A., & D’Agostino, R. B. (1990). A suggestion for using powerful and informative tests of normality. The American Statistician, 44(4), 316–321.
Derogatis, L. R., & Fitzpatrick, M. (2004). The SCL-90-R, the Brief Symptom Inventory (BSI), and the BSI-18. In M. E. Maruish (Ed.), The use of psychological testing for treatment planning and outcomes assessment: Instruments for adults, vol 3, 3rd ed. (pp. 1–41). Mahwah: Lawrence Erlbaum Associates Publishers.
Dick, A. M., Niles, B. L., Street, A. E., DiMartino, D. M., & Mitchell, K. S. (2014). Examining mechanisms of change in a yoga intervention for women: the influence of mindfulness, psychological flexibility, and emotion regulation on PTSD symptoms. Journal of Clinical Psychology, 70(12), 1170–1182.
Duy, B., & Yildiz, M. A. (2017). The mediating role of self-esteem in the relationship between optimism and subjective well-being. Current Psychology, 36(3), 410–416. https://doi.org/10.1007/s12144-017-9698-1.
Field, A. (2009). Discovering statistics using SPSS. London: Sage publications.
Gallagher, M. W., & Lopez, S. J. (2009). Positive expectancies and mental health: identifying the unique contributions of hope and optimism. The Journal of Positive Psychology, 4(6), 548–556.
Gaudiano, B. A., Schofield, C. A., Davis, C., & Rifkin, L. S. (2017). Psychological inflexibility as a mediator of the relationship between depressive symptom severity and public stigma in depression. Journal of Contextual Behavioral Science, 6(2), 159–165. https://doi.org/10.1016/j.jcbs.2017.04.010.
Gunnell, D., Appleby, L., Arensman, E., Hawton, K., John, A., Kapur, N., Khan, M., O’Connor, R. C., Pirkis, J., & COVID-19 Suicide Prevention Research Collaboration. (2020). Suicide risk and prevention during the COVID-19 pandemic. The Lancet Psychiatry., 7, 468–471. https://doi.org/10.1016/S2215-0366(20)30171-1.
Harper, C. A., Satchell, L. P., Fido, D., & Latzman, R. D. (2020). Functional fear predicts public health compliance in the COVID-19 pandemic. International Journal of Mental Health and Addiction. Advance online publication. https://doi.org/10.1007/s11469-020-00281-5.
Harris, R. (2009). ACT made simple: an easy-to-read primer on acceptance and commitment therapy. New Harbinger: Publications.
Hayes, S. C., Luoma, J. B., Bond, F. W., Masuda, A., & Lillis, J. (2006). Acceptance and commitment therapy: model, processes and outcomes. Behaviour Research and Therapy, 44(1), 1–25.
Hayes, S. C., Strosahl, K., & Wilson, K. G. (2012). Acceptance and commitment therapy: the process and practice of mindful change (2nd ed.). NewYork: The Guilford Press.
Hu, L., & Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Structural Equation Modeling, 6, 1–55. https://doi.org/10.1080/10705519909540118.
Ingram, R. E., & Luxton, D. D. (2005). Vulnerability-stress models. Development of psychopathology: A vulnerability-stress perspective, 32–46.
Karademas, E. C. (2006). Self-efficacy, social support and well-being: the mediating role of optimism. Personality and Individual Differences, 40(6), 1281–1290.
Kline, R. B. (2015). Principles and practice of structural equation modeling. New York: Guilford.
Kurz, A. S., Bethay, J. S., & Ladner-Graham, J. M. (2014). Mediating the relation between workplace stressors and distress in ID support staff: comparison between the roles of psychological inflexibility and coping styles. Research in Developmental Disabilities, 35(10), 2359–2370.
Kwok, S. Y., & Gu, M. (2017). The role of emotional competence in the association between optimism and depression among Chinese adolescents. Child Indicators Research, 10(1), 171–185.
Larson, R. W. (2011). Positive development in a disorderly world. Journal of Research on Adolescence, 21(2), 317–334. https://doi.org/10.1111/j.1532-7795.2010.00707.x.
Lee, S. A. (2020). Coronavirus Anxiety Scale: A brief mental health screener for COVID-19 related anxiety. Death Studies. Advance online publicaion. https://doi.org/10.1080/07481187.2020.1748481.
Levens, S. M., & Gotlib, I. H. (2012). The effects of optimism and pessimism on updating emotional information in working memory. Cognition & Emotion, 26(2), 341–350.
Levin, M. E., MacLane, C., Daflos, S., Seeley, J. R., Hayes, S. C., Biglan, A., & Pistorello, J. (2014). Examining psychological inflexibility as a transdiagnostic process across psychological disorders. Journal of Contextual Behavioral Science, 3(3), 155–163. https://doi.org/10.1016/j.jcbs.2014.06.003.
Liu, S., Yang, L., Zhang, C., Xiang, Y. T., Liu, Z., Hu, S., & Zhang, B. (2020). Online mental health services in China during the COVID-19 outbreak. The Lancet Psychiatry, 7(4), e17–e18. https://doi.org/10.1016/S2215-0366(20)30077-8.
Mamun, M. A., & Griffiths, M. D. (2020). First COVID-19 suicide case in Bangladesh due to fear of COVID-19 and xenophobia: possible suicide prevention strategies. Asian Journal of Psychiatry, 51, 102073. https://doi.org/10.1016/j.ajp.2020.102073.
Masuda, A., & Latzman, R. D. (2011). Examining associations among factor-analytically derived components of mental health stigma, distress, and psychological flexibility. Personality and Individual Differences, 51(4), 435–438.
Masuda, A., & Tully, E. C. (2012). The role of mindfulness and psychological flexibility in somatization, depression, anxiety, and general psychological distress in a nonclinical college sample. Journal of Evidence-Based Complementary & Alternative Medicine, 17(1), 66–71.
Mendoza, H., Goodnight, B. L., Caporino, N. E., & Masuda, A. (2018). Psychological distress among Latina/o college students: the roles of self-concealment and psychological inflexibility. Current Psychology, 37(1), 172–179.
Nes, L. S. (2016). Optimism, pessimism, and stress. In G. Fink (Ed.), Stress: Concepts, cognition, emotion, and behavior (pp. 405–411). Elsevier Academic Press.
Nes, L. S., & Segerstrom, S. C. (2006). Dispositional optimism and coping: a meta-analytic review. Personality and Ssocial Ppsychology Rreview, 10(3), 235–251.
Peterson, C., & Chang, E. C. (2003). Optimism and flourishing. In C. L. M. Keyes & J. Haidt (Eds.), Flourishing: Positive psychology and the life well-lived (pp. 55–79). American Psychological Association.
Praharso, N. F., Tear, M. J., & Cruwys, T. (2017). Stressful life transitions and wellbeing: a comparison of the stress-buffering hypothesis and the social identity model of identity change. Psychiatry Research, 247, 265–275. https://doi.org/10.1016/j.psychres.2016.11.039.
Preacher, K. J., & Hayes, A. F. (2008). Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behavior Research Methods, 40(3), 879–891. https://doi.org/10.3758/BRM.40.3.879.
Reed, D. J. (2016). Coping with occupational stress: the role of optimism and coping flexibility. Psychology Research and Behavior Management, 9, 71–79. https://doi.org/10.2147/PRBM.S97595.
Revelle, W. (2019). Ppsych: procedures for psychological, psychometric, and personality research. Northwestern University, Evanston, Illinois. R package version 1.9.12. https://CRAN.R-project.org/package=psych.
Rosseel, Y. (2012). Lavaan: an R package for structural equation modeling. Journal of Statistical Software, 48(2), 1–36.
Sapmaz, F., & Doğan, T. (2012). Mutluluk ve yaşam doyumunun yordayıcısı olarak iyimserlik. Mersin Üniversitesi Eğitim Fakültesi Dergisi, 8(3), 63–69.
Satici, B., Saricali, M., Satici, S. A., & Griffiths, M. D. (2020). Intolerance of uncertainty and mental wellbeing: serial mediation by rumination and fear of COVID-19. International Journal of Mental Health Addiction. https://doi.org/10.1007/s11469-020-00305-0.
Scheier, M. F., & Carver, C. S. (1985). Optimism, coping, and health: assessment and implications of generalized outcome expectancies. Health Psychology, 4(3), 219–247. https://doi.org/10.1037/0278-6133.4.3.219.
Scheier, M. F., & Carver, C. S. (1992). Effects of optimism on psychological and physical well-being: theoretical overview and empirical update. Cognitive Therapy and Research, 16(2), 201–228. https://doi.org/10.1007/BF01173489.
Scheier, M. F., Carver, C. S., & Bridges, M. W. (1994). Distinguishing optimism from neuroticism (and trait anxiety, self-mastery, and self-esteem): a reevaluation of the Life Orientation Test. Journal of Personality and Social Psychology, 67(6), 1063–1107.
Scheier, M. F., Carver, C. S., & Bridges, M. W. (2001). Optimism, pessimism, and psychological well-being, C. In E. C. Chang (Ed.), (pp. 189–216). American Psychological Association.
Tanhan, A. (2019). Acceptance and commitment therapy with ecological systems theory: addressing Muslim mental health issues and wellbeing. Journal of Positive Psychology and Wellbeing, 3(2), 197–219.
Tanhan, A., Yavuz K. F., Young, J. S., Nalbant, A., Arslan, G., Yıldırım, M., Ulusoy, S., Genç, E., Uğur, E., & Çiçek, İ. (2020). A proposed framework based on literature review of online contextual mental health services to enhance wellbeing and address psychopathology during COVID-19. Electronic Journal of General Medicine.
Tavakoli, N., Broyles, A., Reid, E. K., Sandoval, J. R., & Correa-Fernández, V. (2019). Psychological inflexibility as it relates to stress, worry, generalized anxiety, and somatization in an ethnically diverse sample of college students. Journal of Contextual Behavioral Science, 11, 1–5. https://doi.org/10.1016/j.jcbs.2018.11.001.
Taylor, S. E., & Armor, D. A. (1996). Positive illusions and coping with adversity. Journal of Personality, 64(4), 873–898.
Taylor, S., Landry, C., Paluszek, M., Fergus, T. A., McKay, D., & Asmundson, G. J. (2020). Development and initial validation of the COVID stress scales. Journal of Anxiety Disorders, 102232, 102232. https://doi.org/10.1016/j.janxdis.2020.102232.
Towsyfyan, N., & Hossein Sabet, F. (2017). The effectiveness of acceptance and commitment therapy on the improving of resilience and optimism in adolescents with major depressive disorder. International Journal of Humanities and Social Science, 7(3), 239–245.
Turkish Ministry of Health (2020). Türkiye’deki güncel durum. https://covid19.saglik.gov.tr/.
Uğur, E., Kaya, Ç., & Tanhan, A. (2020). Psychological inflexibility mediates the relationship between fear of negative evaluation and psychological vulnerability. Submitted for publication.
Vickers, K. S., & Vogeltanz, N. D. (2000). Dispositional optimism as a predictor of depressive symptoms over time. Personality and Individual Differences, 28(2), 259–272.
Wang, C., Pan, R., Wan, X., Tan, Y., Xu, L., Ho, C. S., & Ho, R. C. (2020). Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. International Journal of Environmental Research and Public Health, 17(5), 1729. https://doi.org/10.3390/ijerph17051729.
Woldgabreal, Y., Day, A., & Ward, T. (2016). Linking positive psychology to offender supervision outcomes: the mediating role of psychological flexibility, general self-efficacy, optimism, and hope. Criminal Justice and Behavior, 43(6), 697–721. https://doi.org/10.1177/0093854815620816.
Woodruff, S. C., Glass, C. R., Arnkoff, D. B., Crowley, K. J., Hindman, R. K., & Hirschhorn, E. W. (2014). Comparing self-compassion, mindfulness, and psychological inflexibility as predictors of psychological health. Mindfulness, 5(4), 410–421.
World Health Organization. (2020). Naming the coronavirus disease (COVID-19) and the virus that causes it. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance.
Yadavaia, J. E., Hayes, S. C., & Vilardaga, R. (2014). Using acceptance and commitment therapy to increase self-compassion: a randomized controlled trial. Journal of Contextual Behavioral Science, 3(4), 248–257.
Yao, H., Chen, J. H., & Xu, Y. F. (2020). Rethinking online mental health services in China during the COVID-19 epidemic. Asian Journal of Psychiatry, 50, 102015. https://doi.org/10.1016/j.ajp.2020.102015.
Yavuz, F., Ulusoy, S., Iskin, M., Esen, F. B., Burhan, H. S., Karadere, M. E., & Yavuz, N. (2016). Turkish version of Acceptance and Action Questionnaire-II (AAQ-II): A reliability and validity analysis in clinical and non-clinical samples. Klinik Psikofarmakoloji Bülteni-Bulletin of Clinical Psychopharmacology, 26(4), 397–408.
Yildirim, M., & Alanazi, Z. S. (2018). Gratitude and life satisfaction: mediating role of perceived stress. International Journal of Psychological Studies, 10(3), 21–28.
Yildirim, M., & Arslan, G. (2020). Exploring the associations between resilience, dispositional hope, subjective well-being, and psychological health among adults during early stage of COVID-19. https://doi.org/10.31234/osf.io/vpu5q.
Yıldırım, M., & Güler (2020). Development and initial validation of the coronavirus perceived risk scale and its relationship with mental health.
Zandifar, A., & Badrfam, R. (2020). Iranian mental health during the COVID-19 epidemic. Asian Journal of Psychiatry, 51, 101990. https://doi.org/10.1016/j.ajp.2020.101990.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Consent was obtained from all participants included in the study.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Arslan, G., Yıldırım, M., Tanhan, A. et al. Coronavirus Stress, Optimism-Pessimism, Psychological Inflexibility, and Psychological Health: Psychometric Properties of the Coronavirus Stress Measure. Int J Ment Health Addiction 19, 2423–2439 (2021). https://doi.org/10.1007/s11469-020-00337-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11469-020-00337-6