
Abstract
Problematic smartphone use is rising across the world. We tested an intervention with ten strategies that nudge users to reduce their smartphone use, for example by disabling non-essential notifications and changing their display to greyscale. Participants first completed baseline measures of smartphone use, well-being, and cognition before choosing which intervention strategies to follow for 2 to 6 weeks. Study 1 (\(N=51\)) used a pre–post design while study 2 (\(N=70\)) compared the intervention to a control group who monitored their screen time. Study 1 found reductions in problematic smartphone use, screen time, and depressive symptoms after 2 weeks. Study 2 found that the intervention reduced problematic smartphone use, lowered screen time, and improved sleep quality compared to the control group. Our brief intervention returned problematic smartphone use scores to normal levels for at least 6 weeks. These results demonstrate that various strategies can be combined while maintaining feasibility and efficacy.
Similar content being viewed by others

Introduction
Around half of the global population owns a smartphone and this number continues to rise (Newzoo, 2021; O’Dea, 2021). Screen time is similarly increasing: young adults across the world now spend 2 to 3 h per day on social media alone (GlobalWebIndex, 2021). Accordingly, there have been growing concerns about problematic smartphone use, in which compulsive patterns of use impair daily functioning (Busch & McCarthy, 2021). A recent meta-analysis of 24 countries found that problematic smartphone use has been increasing across the world for the past decade (Olson et al., 2022), despite the growing availability of technological interventions such as screen time tracking aiming to reduce it (Deloitte, 2019).
Problematic smartphone use has been associated with various negative effects, such as cognitive impairments across the domains of driving, work, and education (Wilmer et al., 2017). Using a phone while driving slows reaction time, increases erratic behaviour, and can cause collisions (Caird et al., 2014; National Center for Statistics and Analysis, 2020; Perlman et al., 2019). At work, receiving notifications can impair task performance as much as writing a text message or talking on the phone (Stothart et al., 2015). Even the mere presence of one’s smartphone can reduce performance on working memory tasks (Ward et al., 2017). Problematic smartphone use and social networking site use also negatively correlate with university grades (Kirschner & Karpinski, 2010; Li et al., 2015), though the effect sizes may be small (Bjerre-Nielsen et al., 2020).
The evidence is mixed regarding the relationship between problematic smartphone use and well-being. Some studies have found that smartphone use at night is associated with later bedtimes and lower sleep quality (Demirci et al., 2015; Lemola et al., 2014); others have argued that these correlations are present but weak (Orben & Przybylski, 2020; Przybylski, 2019). There is even less agreement about the relationship between phone use and depression. Country-wide smartphone ownership has coincided with increases in depression and anxiety among teenagers and young adults (Twenge et al., 2019). Cross-sectional surveys show negative correlations between screen time and well-being (Sarris et al., 2020; Twenge et al., 2018), and laboratory studies have found an association between problematic smartphone use and depression (Elhai et al., 2017). These links may be strongest when phones are used for passive social media consumption (e.g. scrolling through feeds without interaction) rather than to actively socialise (Elhai et al., 2017; Escobar-Viera et al., 2018). In contrast, other researchers have argued that these correlations may be inflated by flexible definitions of well-being (Orben & Przybylski, 2019a; Orben & Przybylski, 2019b), screen time (Kaye et al., 2020), and problematic smartphone use (Connolly et al., 2021). Evidence is also mixed regarding the effectiveness of behavioural interventions that target phone use to reduce depression. One study found that limiting social networking site use to 10 min per platform per day reduced depression (Hunt et al., 2018); another intervention also reduced screen time but found no such effect (Holte & Ferraro, 2020). Researchers continue to debate the nature and magnitude of the link between smartphone use and specific aspects of well-being (Twenge et al., 2020).
Perhaps the simplest argument for reducing smartphone use is that many people would rather spend their time doing something else (Deloitte, 2018; Lukoff et al., 2018). Nearly half of smartphone users in developed countries consider themselves to be over-using their phones (Deloitte, 2019). Problematic smartphone use may have negative consequences because it replaces or interferes with activities that increase well-being, such as sleeping, exercising, or (in-person) socialising (Kushlev & Leitao, 2020). Indeed, adolescents worldwide are doing less of these healthy activities than in the past (Guthold et al., 2018; Keyes et al., 2015; Sarris et al., 2020; Twenge et al., 2019), likely in part due to technology use (Oberle et al., 2020).
Individual Interventions
The most common method of reducing problematic smartphone use involves screen time monitoring (Zimmermann, 2021), which is now built in to most smartphones. Still, only a minority of smartphone owners report using it (Deloitte, 2019), and screen time notifications alone may be ineffective at reducing screen time or phone checking behaviour (Loid et al., 2020; Zimmermann, 2021). Some researchers have also argued that “fighting tech with tech” may pose a conflict of interest, since phone manufacturers or app designers may be financially motivated to maximise rather than reduce engagement (Rezaee & Pedret, 2018). In addition to monitoring, over 100 apps claim to help with reducing screen time (Bychkov & Young, 2018). Most of these do not rely on psychological theories or mechanisms (van Velthoven et al., 2018) and only a handful have been formally tested (Mac Cárthaigh, 2020). Some of the more effective ones can reduce social media use (Okeke et al., 2018) or screen time (Busch & McCarthy, 2021; Kim et al., 2019), but one survey found that most people are not willing to use additional technology to help them do so; they would rather have more control over the process (Hiniker et al., 2015).
Other approaches have focused on monetary incentives and self-control, such as limiting daily time spent on social networking sites (Allcott et al., 2011; Collis & Eggers, 2019; Hunt et al., 2018; Okeke et al., 2018). Such restrictions can reduce screen time and depressive symptoms (Hunt et al., 2018) as well as improve well-being during the study period (Allcott et al., 2020). These approaches, while effective, may be less feasible for some populations in the long term. Participants tend to stop their restrictions at the end of the intervention period (Hunt et al., 2018), and others say they would need to be paid over $1,000 to deactivate their Facebook account for 1 year (Corrigan et al., 2018; Mosquera et al., 2019). People generally struggle to regulate their smartphone use (Ko et al., 2015) and over-estimate their level of self-control while doing so (Allcott et al., 2020). These issues are exacerbated by technological design decisions: many apps use psychological factors such as motivation and reward schedules to intentionally promote habitual use (Chen et al., 2019; Eyal, 2014; Fogg, 2009; Oulasvirta et al., 2011). Smartphones and their interfaces are also designed to be easy to use with little friction, which results in appealing products but also habitual behaviour (Anderson & Wood, 2020). These various factors may help explain why, in one survey, only half of Americans trying to reduce their phone use reported successfully doing so (Deloitte, 2018).
Combined Interventions
Although various studies have tested individual strategies for reducing smartphone use, few have attempted to combine them (e.g. Throuvala et al., 2020; Myers et al., 2021) and almost none have used a more customised approach. Allowing people to “mix and match” various strategies based on their lifestyle may have several advantages over a one-size-fits-all approach (cf. Sunstein, 2021). Because they are based on personal preference, the strategies may achieve higher compliance or efficacy over the long term. Accordingly, we sought to develop a personalised and multi-faceted behavioural intervention to reduce problematic smartphone use and screen time.
Our intervention focuses on nudges (Thaler and Sunstein, 2021): here, small changes to phone settings or the environment intended to reduce phone use. Changing the smartphone display to greyscale, for example, can reduce screen time, problematic smartphone use, and anxiety (Holte et al., 2021; Holte & Ferraro, 2020). The effectiveness of such nudges can be explained by the Fogg Behaviour Model, which posits that habitual behaviours result from the combination of motivation, ability, and prompts (Fogg, 2019). Habitual smartphone use, for example, may result from a prompt such as a social media notification, the ease (ability) of picking up the phone and scrolling through a feed, and the motivation to pass time when bored (Oulasvirta et al., 2011). Crucially, many app developers draw from this model to intentionally promote habitual use (Eyal, 2014; Fogg, 2009), so reversing the same principles may help reduce usage (Eyal, 2019; Fogg, 2019). For example, reducing notifications (prompts), keeping the phone out of reach at night (ability), and making the phone less aesthetically pleasing with the greyscale setting (motivation) can all reduce phone usage and improve various aspects of well-being (Fitz et al., 2019; Holte et al., 2021; Hughes & Burke, 2018). Table 1 shows the ten components of our intervention.
We tested this combined intervention on university students in two pre-registered studies. First, we tested the feasibility and initial efficacy using a pre–post design over 2 weeks. Given the results of studies testing similar individual strategies, we hypothesised that the combined intervention would reduce problematic smartphone use, screen time, and depressive symptoms as well as improve sleep quality and cognition (sustained attention and working memory). Second, we compared our intervention to an active control group who only enabled screen time monitoring. We had confirmatory assessments at 2 weeks and exploratory assessments at 6 weeks. Combined, these studies demonstrate the preliminary feasibility and efficacy of a multi-faceted nudge-based intervention to reduce problematic smartphone use.
Methods
Study 1
Participants
We recruited a convenience sample of 51 participants (36 women) from social media advertisements and from the psychology participant pool at McGill University. Most were students and all were between 18 and 34 years old (M = 21.7, SD = 2.8). To be eligible, participants needed an iPhone with iOS version 12 (or later) which includes built-in screen time tracking. We included only participants with normal or corrected-to-normal vision who were not taking any medication and had no history of neurological or psychiatric issues. Participants received $20 or course credit. The protocols for both studies were approved by the McGill University Research Ethics Board II (#451-0518) and followed the Declaration of Helsinki.
We were interested in detecting medium effect sizes; smaller effects may not justify the complexity of a multi-faceted intervention. We posted weekly experiment slots until we reached 50 participants with complete data, which gave us 80% power to detect small-to-medium effects (d = 0.36) for our directional confirmatory tests.
Procedure
Baseline Measures
After completing an online screening for eligibility, participants were asked if they had screen time tracking enabled on their phone. Those who did scheduled a lab visit; those who did not were asked to enable it and schedule a visit 1 week later. This procedure gave 1 week of baseline tracking before the intervention began, allowing us to disentangle the effects of the intervention from the effects of enabling the tracking. At the lab, the experimenter obtained informed consent and then asked the participants to silence their phone and place it in the corner of the room to reduce distractions (Ward et al., 2017). Participants then completed baseline measures of cognition, depression, problematic smartphone use, sleep, mood, and personality.
Intervention
The experimenter explained that the study was testing the feasibility of a 10-part behavioural intervention to reduce smartphone use. The experimenter led the participants through each strategy, asked if they would like to follow it, and if so, guided them through the implementation. Participants chose the extent to which they followed each strategy, for example ranging from disabling only sounds to disabling any visual notifications. They were then asked to follow the intervention for 2 weeks. To increase compliance, we offered them an additional $20 incentive to follow the strategies, which we provided at the end of the study period. Finally, the participants took a screenshot of the screen time summary on their phone and emailed it to the experimenter as the baseline measurement (i.e. for the week prior to the study). They also completed this procedure the following week at home; we did not analyse this at-home data because we expected lower compliance and more variability in the reporting since participants could send the screenshots at any time. We present the at-home data in figures for completeness.
Post Measures
Two weeks after the first visit (13 to 15 days later), participants returned to the lab to complete the same measures except for the (trait-level) personality questionnaires. The experimenter then debriefed and compensated the participants.
Measures
Sustained Attention to Response Task (SART)
Participants first completed the SART, which measures sustained attention and response inhibition (Robertson et al., 1997). The task involves pressing a key when any digit appears on the screen except for a “3”; the computer recorded errors of omission and commission. Since phone notifications can impair SART performance (Stothart et al., 2015), we were interested in testing whether the intervention could lead to longer-term improvements on the task.
Operation Span Task (OSpan)
The OSpan measures working memory capacity (Unsworth et al., 2005) and is affected by the presence of a smartphone (Ward et al., 2017). Participants remembered sequences of letters while completing simple math problems.
Beck Depression Inventory II (BDI-II)
The BDI assesses the severity of depressive symptoms such as sadness and loss of pleasure over the previous 2 weeks (Beck et al., 1996). An example item ranges from “I do not feel sad” (0 points) to “I am so sad or unhappy that I can’t stand it” (3 points). Total scores range from from 0 to 63, with 14 being the cut-off for mild depression. The scale’s internal consistency for college students is high (\(\alpha = .93\)) (Beck et al., 1996) and was similar in our samples (study 1: \(\alpha = .93\), study 2: \(\alpha = .88\)).
Smartphone Addiction Scale — Short Version (SAS-SV)
The SAS-SV is the most common measure of problematic smartphone use (Olson et al., 2022) and asks about disturbances in daily life and withdrawal symptoms related to phones (Kwon et al., 2013). We used the 10-item version of this scale with minor edits for clarity from a previous study (Olson et al., 2020). An example item is: “I have a hard time concentrating in class, while doing assignments, or while working, due to smartphone use”. Each item uses a Likert scale ranging from 1 (strongly disagree) to 6 (strongly agree), for a total score between 10 and 60. The scale usually has high internal consistency (\(\alpha = .91\)) (Kwon et al., 2013); it was slightly lower in our samples (study 1: \(\alpha = .82\), study 2: \(\alpha = .78\)) but was similar to another sample from the same university (.83) (Olson et al., 2020). This and the subsequent non-trait questionnaires asked about the previous 2 weeks to stay consistent with the intervention period and the BDI.
Sleep Quality Scale (SQS)
The SQS measures sleep quality with one item: “Rate your sleep quality from 0 to 10, with 0 being the worst possible sleep, and 10 being the best”. The measure correlates well with longer sleep questionnaires (Cappelleri et al., 2009).
International Positive and Negative Affect Scale (PANAS) — Short Form
The PANAS measures positive and negative affect as independent dimensions (Thompson, 2007). Participants rate 10 items (e.g. interested, hostile) on 5-point scales ranging from 1 (never) to 5 (always). The scale usually has acceptable reliability (\(\alpha\) of .75 for positive affect and .76 for negative), which was similar in our sample for positive (study 1: \(\alpha = .66\), study 2: \(\alpha = .80\)) and negative affect (study 1: \(\alpha = .82\), study 2: \(\alpha = .75\)).
Trait-Level Measures
Finally, participants completed the Big Five Inventory (BFI) for basic personality traits (John et al., 1991) and the Internal Control Index (ICI) which measures how much control they feel they have over their lives (Duttweiler, 1984). They also completed a creativity measure (Olson et al., 2021) for a study described elsewhere (Olson et al., 2022).
Analysis
The design and analysis were pre-registered (https://osf.io/wmvje); all pre-registered tests are labelled as confirmatory and the rest as exploratory. We conducted 6 directional paired-samples t tests, predicting that participants would (1) report lower problematic smartphone use (SAS-SV), (2) use their phone less (screen time), (3) reduce depression (BDI-II), (4) improve sleep quality (SQS), (5) increase working memory capacity (OSpan), and (6) make fewer attentional errors (SART). We used a type I error rate of .05 with no family-wise error control. We included all participants regardless of how much of the intervention they followed, in order to better assess feasibility and promote external generalisability (Heintzelman & Kushlev, 2020). One participant missed 1 week of screen time reporting and was thus excluded from the test of screen time.
Study 2
Participants
Using the same procedure as in study 1, we recruited 82 participants. Based on the pre-registration, we excluded 12 of them: 7 dropped out (6 control and 1 intervention; 4 during the pandemic), 1 updated his phone which deleted all screen time data, and 4 did not follow most of the intervention. Because we were interested in testing efficacy for study 2, we included only participants who followed at least 5 strategies of the intervention. The final sample included 70 participants (54 women; aged 18 to 33, \(M = 20.7\), \(SD = 2.6\)).
Procedure
Participants completed two lab visits over 2 weeks, with the same tasks and questionnaires as in study 1. We excluded the SART given its length and the lack of effect in the previous study. After the baseline measurements, participants were randomly assigned to an experimental condition. Neither group was told about the other condition, nor about any condition assignment at all. Consistent with study 1, the experimenter explained as a cover story that we were exploring patterns of smartphone use and their relation to demographics. Both groups then enabled screen time tracking. We chose screen time tracking as the control since it is likely the most popular smartphone reduction intervention (Zimmermann, 2021) and is feasible to implement. The intervention participants were additionally led through the ten strategies which resembled those of study 1 with minor changes based on new research (see Table 5).
Two weeks later, participants returned to the lab to complete the same measures and a questionnaire assessing the feasibility of the intervention. The final 11 participants completed their second visit online after the university closed due to the COVID-19 pandemic, which meant they could not complete the OSpan task. We also asked participants how they spent any additional free time; two raters later categorised their responses and a third resolved discrepancies.
We gave participants $20 and told them that the intervention period was now complete. We suggested that they continue to follow the intervention as much as is feasible but they would not be compensated for doing so. Another 4 weeks later, participants completed online questionnaires to assess compliance after the main study period. All participants then reported compliance and the last half of the sample (\(N = 44\)) re-completed all of the questionnaire measures (e.g. depression) to monitor improvements over a longer period. We only assessed the last half of the sample due to menial procedural delays as the pandemic approached. Participants received an additional $20 for completing the follow-up measures.
Measures
Our confirmatory outcomes were all of the measures that showed effects in study 1: screen time, problematic smartphone use, depression, and working memory. Our exploratory outcomes were sleep quality, positive affect, and negative affect.
Analysis
The design and analysis were pre-registered (https://osf.io/3p7rz). We used mixed-effect linear regression to predict each measure given the condition (control or intervention), time (baseline or 2 weeks later), and the interaction, with a random intercept for each participant. We did confirmatory tests of the interactions for the primary outcomes and exploratory tests for the secondary outcomes. We used a type I error rate of .05 and directional tests, predicting that intervention participants would show larger improvements on each measure. We deviated from our pre-registered sample size (\(N = 70\) rather than 80) when the university closed due to the pandemic.
Based on the pre-registration, we excluded two additional participants from only the test of screen time: one had an extreme score (\(z > 4\)) and one sent the screen time data too late. For the OSpan test, an additional five participants were excluded due to technical errors during the task.
Results
Compliance
In study 1, participants reported following an average of 7.50 out of the 10 strategies by week 2 (\(SD=1.49\)). In study 2, with a slightly modified intervention, participants initially agreed to follow 8.79 (1.37) of the strategies; 2 weeks later, they reported successfully following 7.28 (1.41) of them. After these 2 weeks, we told participants that the main study period had ended but to continue to follow the intervention as much as is feasible. At 6 weeks, participants continued to follow most of the strategies (\(M = 5.55\), \(SD=2.27\)). The participants were most likely to comply with reducing notifications and least likely to keep their screen on greyscale (study 1) or to leave their phone at home (study 2). See Tables 4 and 5 for individual compliance rates.
Confirmatory Tests
Problematic Smartphone Use
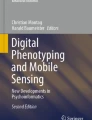
The intervention reduced problematic smartphone use. In study 1, participants initially scored 35.29 on the Smartphone Addiction Scale (Short Version), which ranges from 10 to 60. Based on the scale authors’ original cut-offs of 31 for men and 33 for women (Kwon et al., 2013), 67% would be considered at a high risk of smartphone addiction. During the intervention, participants dropped to a score of 28.08 (\(t(50) = -6.85\), \(d =-0.96\,[-1.21, -0.69]\), \(p <.001\); Fig. 1a), putting only 35% above the high-risk threshold and thereby returning them to a more normal range for samples in North America (Olson et al., 2022). Study 2 showed similar reductions; the intervention group dropped by 5.49 points while the control group dropped by only 0.63. See Table 2 for regression models and Tables 6 and 7 for descriptive statistics.
Screen Time
The intervention also reduced screen time. In study 1, daily usage dropped from 4.67 to 3.40 h, for a difference of 1.27 h per day at week 2 (\(t(49) = -6.18\), \(d =-0.87\,[-1.22, -0.45]\), \(p <.001\); Fig. 1b). In study 2, daily screen time dropped by an average of 11 min in the control group and 57 min in the intervention group. The largest proportion of screen time was spent on social networking, consistent with other studies (Panova et al., 2019). This amount increased by 8 min in the control group and decreased by 16 min in the intervention group.

Dependent measures by time and condition. In both studies, during the intervention, participants reduced their problematic smartphone use (A) and screen time (B). In study 1, participants reduced in depression (C), but there was relatively little change between the groups in study 2. Only in study 2, sleep quality increased (D). Dots show means and bands show 95% confidence intervals. Solid lines show main study period; dotted lines show exploratory follow-up period
Depression
There were inconsistent results for depression (Fig. 1c). In study 1, participants began with a depression score of 11.57, with 33% in the range of at least mild depression. During the intervention, their depression scores decreased to 6.90, with only 14% at the clinical cut-off (\(t(50) = -4.25\), \(d =-0.59\,[-0.92, -0.12]\), \(p <.001\)). Study 2, however, found no difference in depression between the groups; both appeared to show similar reductions.
Cognition
In study 1, working memory improved (\(t(50) = 1.95\), \(d =0.27\,[-0.01, 0.53]\), \(p =.029\)), but both groups showed similar changes in study 2. We did not see any changes in sustained attention errors, which we only tested in study 1 (\(t(50) = 1.12\), \(d =0.16\,[-0.11, 0.43]\), \(p =.866\)).
Exploratory Tests
Sleep Quality
Study 1 found little change in sleep quality, which went from 6.61 to 6.94 out of 10 (\(t(50) = 1.07\), \(d =0.15\,[-0.14, 0.43]\), \(p =.144\); Fig. 1d). In study 2, the control group showed no increase (\(-0.60\) points) while the intervention group showed an increase of 1.23 points. This improvement would be considered clinically significant (Zisapel and Nir, 2003) and persisted for at least 6 weeks while the gap between the groups diminished.
Mood
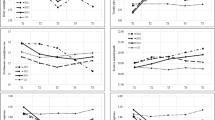
There was comparatively little change in mood. Positive affect remained fairly consistent and negative affect seemed to reduce by similar amounts across both studies and groups. Figure 2 summarises the overall effects of all measures.

Effect sizes across studies between the baseline and 2 weeks later. Error bars show bootstrapped 95% confidence intervals
Individual Differences
Combining both intervention groups for greater statistical power (\(N = 86\)), exploratory analyses revealed that people who followed more of the intervention strategies showed greater reductions in depression (\(r(77) = -.37\ [-.55, -.17]\), \(p<.001\)) and screen time (\(r(75) = -.23\ [-.43, -.00]\), \(p=.048\)) as well as improvements in positive mood (\(r(77) = .32\ [.10, .50]\), \(p=.005\)). Across both studies, we also saw negative correlations between baseline problematic smartphone use, depression, and mood (Fig. 3). Based on exploratory regression models predicting composite standardised improvements across the variables common in both studies, the strategies that predicted the most improvements were reducing notifications (strategy #1, study 2 \(b = 2.35\)), intending to use the phone less (#10, study 2 \(b = 1.82\)), and changing the phone’s display properties (#5, study 1 \(b = 1.46\), study 2 \(b = 1.34\)). There were no strong sex differences in the results.
Interviews
In study 2, participants in the intervention group reported various positive effects such as more focus and better social interactions (Table 3), consistent with other studies (Myers et al., 2021). The only adverse effect reported was an increase in anxiety due to fear of missing out on conversations (cf. Hunt et al., 2018; Myers et al., 2021). The control group reported fewer effects, whether positive or negative.
We also asked participants how they spent any additional free time, in case they simply replaced phone use with computer use. Intervention participants commonly reported spending more time on studying or work (51%), enjoyable activities such as hobbies or cooking (26%), or interacting with friends and family (21%). Less frequently, they spent time on household chores (13%), computers (13%), exercise (5%), or sleep (5%).
Discussion
As problematic smartphone use rises across the world (Olson et al., 2022), there will be a growing need for feasible and effective approaches to reduce it. We developed a behavioural intervention to reduce phone use without relying on additional technology or considerable self-control. The intervention, which takes around 10 min to explain and begin implementing, returned problematic smartphone use to normal levels, improved sleep quality, and reduced screen time by around an hour per day. The participants commonly reported spending this extra free time on studying, hobbies, or socialising. Our results support the idea that problematic smartphone use may reduce well-being in part by replacing or interfering with these healthy activities (Kushlev & Leitao, 2020).
Our intervention caused larger improvements than screen time monitoring alone. Some of these effect sizes were also larger than those seen in studies testing individual strategies. For example, our intervention groups reduced problematic smartphone use scores by 5.5 to 7.2 points (studies 1 and 2), which is larger than when changing the display to greyscale (2.6 points; Holte et al., 2021), leaving the phone outside the bedroom (1.6 points; Hughes & Burke, 2018), or batching notifications (\(< 1\) point between groups; Fitz et al., 2019). We did not see any backfire effects: across both studies, only one participant (1%) increased problematic smartphone use (by 1 point) and screen time (by half an hour) following the intervention, compared to 23% in the control group.
The results were mixed for sleep quality: Study 1 found little change while study 2 found an improvement during the intervention. Other experimental and correlational studies have also found a link between sleep and smartphone use (Demirci et al., 2015; Hughes & Burke, 2018; Lemola et al., 2014), though the strength of this relationship may be small (Orben & Przybylski, 2020). We also saw little change in cognition and mood, though we lacked the statistical power to detect any potential small effects. Overall, all of the sample effects were in the predicted directions when comparing between the groups.
The causal effects on depression were also unclear. In study 2, both groups appeared to show similar reductions in depressive symptoms (\(b = -0.24\); Fig. 2) and negative affect (\(b = -0.41\); Table 1). It is thus difficult to tell whether these reductions were caused by the intervention, consistent screen time tracking, or incidental aspects of the study such as demand characteristics or observation effects. Still, participants who followed the intervention more closely showed larger reductions in depressive symptoms, and these symptoms positively correlated with both screen time and problematic smartphone use (Fig. 3). It is possible that closely following the intervention reduced depressive symptoms, or perhaps people with more malleable depressive symptoms were more likely to comply with the intervention strategies. Our results are consistent with studies suggesting that there may be a link between well-being and smartphone use, though this link may be weaker than was previously believed (Coyne et al., 2020; Orben & Przybylski, 2019a).
Strengths
Our results demonstrate that combining different behavioural strategies can form a feasible and efficacious intervention to reduce smartphone use. Such an intervention could be useful to reach a larger population than those who would be willing to apply any specific strategy. For example, switching the screen to greyscale has several benefits (Holte et al., 2021; Holte & Ferraro, 2020), but this strategy had some of the lowest compliance rates (e.g. 38% in study 1; Table 4). Furthermore, combining intervention strategies in a more flexible approach could allow for easier recruiting of larger samples and may improve long-term compliance. Indeed, participants in study 2 continued to follow most of the intervention strategies for at least 4 weeks beyond the main study period (Table 5). Some of this high compliance was likely because several of the strategies are “set and forget” — the phone settings only need to be changed once — which may make them more sustainable rather than relying solely on consistent self-control. Finally, because the intervention is based on general behavioural principles (Fogg, 2019), the strategies could be adapted for other technologies such as smart watches or virtual reality devices.
Limitations
The flexibility of the intervention also presented limitations. Because the intervention used a combination of strategies and participants chose which ones to follow, it is difficult to determine their mechanisms or relative efficacy. We have previously argued that intervention development could involve an initial “shotgun” approach to first determine whether the intervention as a whole is feasible and efficacious before assessing its key components and underlying mechanisms (Olson et al., 2021).
Another potential issue was related to the pre-existing differences between conditions in study 2. The intervention and control groups differed in their initial screen time (\(p = .026\); Table 7) even though they were randomised after the baseline measures. Although we only saw these differences in screen time and controlled for them in our regression model, our effect sizes may have been either under- or over-estimated. For example, people in the intervention group who began with lower smartphone use may have had less room to improve, reducing the effect size; or, they may have found their habitual behaviours easier to change, increasing the effect size.
Future Research and Implications
Future studies could assess compliance in real-world or clinical settings and test additional demographic characteristics to better predict who may benefit from which components of the intervention (Sunstein, 2021). These studies could also help determine which strategies are best for people who are already following particular guidelines, such as those with notifications disabled. More research on these topics will help balance long-term feasibility with effectiveness for different people.
Our results may be useful for phone manufacturers and app developers interested in improving digital well-being. Screen time tracking alone — though commonly included in smartphones — had little effect on phone behaviour 6 weeks later (Fig. 1b), consistent with other studies (Loid et al., 2020; Zimmermann, 2021). To effectively reduce screen time, several of our intervention strategies could be adapted for future operating systems. Apple’s app store has started disclosing privacy ratings of various apps; a similar approach for digital well-being could also be useful. For example, apps could be penalised for giving too many notifications that participants end up muting or ignoring. Reducing notifications could also be made easier; there could be a setting to allow notifications from particular apps only if they have been used recently, which would prevent transactional apps from sending unnecessary notifications. Another setting could make the phone unlock slightly slower in order to add a small amount of friction to phone checking. Of course, these practices may make phones less accessible, less attractive, or harder to use — and perhaps less profitable. Given recent criticisms of technology companies and their role in well-being (e.g. Hemphill & Banerjee, 2021), a longer-term profitable approach may involve preventive and proactive maintenance of healthy digital habits to sustain public trust.
Technology alone, however, cannot offer a complete solution. We agree with researchers and ethicists who argue that reducing problematic smartphone use should ultimately result from re-establishing healthy habits, a broader philosophy of technology use, and cooperation with technology companies (Heitmayer & Lahlou, 2020; Newport, 2019). Newport (2019, p. 28), who argues for “digital minimalism”, states that:
What all of us who struggle with these issues need [...] is a philosophy of technology use, something that covers from the ground up which digital tools we allow into our life, for what reasons, and under what constraints. In the absence of this introspection, we’ll be left struggling in a whirlwind of addictive and appealing cyber-trinkets, vainly hoping that the right mix of ad hoc hacks will save us.
Until our habits are rewired and such a philosophy of technology gains traction, we hope that our particular mix of strategies can at least serve as a stopgap. These strategies will be especially important following recent global increases in remote work and online schooling. Feasible behavioural interventions could help people use technology in ways that are beneficial while minimising any negative effects. With half of the population owning a smartphone, and many of them trying to reduce their screen time, even small changes to phone habits could free an immeasurable amount of collective time across the world.
Data Availability
Anonymised data sets are available (https://osf.io/5mqnp/).
Change history
02 September 2022
A Correction to this paper has been published: https://doi.org/10.1007/s11469-022-00898-8
References
Allcott, H., Braghieri, L., Eichmeyer, S., & Gentzkow, M. (2020). The welfare effects of social media. American Economic Review, 110(3), 629–676. https://doi.org/10.1257/aer.20190658.
Allcott, H., Gentzkow, M., & Song, L. (2021). Digital addiction. National Bureau of Economic Research.
Anderson, I. A., & Wood, W. (2020). Habits and the electronic herd: The psychology behind social media’s successes and failures. Consumer Psychology Review, 4(1), 83–99. https://doi.org/10.1002/arcp.1063.
Beck, A. T., Steer, R. A., & Brown, G. K. (1996). Beck Depression Inventory (BDI-II). Pearson.
Bjerre-Nielsen, A., Andersen, A., Minor, K., & Lassen, D. D. (2020). The negative effect of smartphone use on academic performance may be overestimated: Evidence from a 2-year panel study. Psychological Science, 095679762095661. https://doi.org/10.1177/0956797620956613.
Busch, P. A., & McCarthy, S. (2021). Antecedents and consequences of problematic smartphone use: A systematic literature review of an emerging research area. 114, 106414. https://doi.org/10.1016/j.chb.2020.106414.
Bychkov, D., & Young, S. D. (2018). Facing up to nomophobia: A systematic review of mobile phone apps that reduce smartphone usage. In Studies in big data (pp. 161–171). Springer Singapore. https://doi.org/10.1007/978-981-10-8476-8_8.
Caird, J. K., Johnston, K. A., Willness, C. R., Asbridge, M., & Steel, P. (2014). A meta-analysis of the effects of texting on driving. Accident Analysis & Prevention, 71, 311–318. https://doi.org/10.1016/j.aap.2014.06.005.
Cappelleri, J. C., Bushmakin, A. G., McDermott, A. M., Sadosky, A. B., Petrie, C. D., & Martin, S. (2009). Psychometric properties of a single-item scale to assess sleep quality among individuals with fibromyalgia. Health and Quality of Life Outcomes, 7(1), 54. https://doi.org/10.1186/1477-7525-7-54.
Chang, A.-M., Aeschbach, D., Duffy, J. F., & Czeisler, C. A. (2014). Evening use of light-emitting eReaders negatively affects sleep, circadian timing, and next-morning alertness. Proceedings of the National Academy of Sciences, 112(4), 1232–1237. https://doi.org/10.1073/pnas.1418490112.
Chen, C., Zhang, K. Z. K., Gong, X., & Lee, M. (2019). Dual mechanisms of reinforcement reward and habit in driving smartphone addiction. 29(6), 1551–1570. https://doi.org/10.1108/intr-11-2018-0489.
Collis, A., & Eggers, F. (2019). Effects of restricting social media usage. SSRN. https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3518744.
Connolly, T., Atherton, G., Cross, L., Piovesan, A., & Kaye, L. K. (2021). The wild west of measurement: Exploring problematic technology use cut off scores and their relation to psychosocial and behavioural outcomes in adolescence. 125, 106965. https://doi.org/10.1016/j.chb.2021.106965.
Corrigan, J. R., Alhabash, S., Rousu, M., & Cash, S. B. (2018). How much is social media worth? Estimating the value of Facebook by paying users to stop using it. PLOS One, 13(12), e0207101. https://doi.org/10.1371/journal.pone.0207101.
Coyne, S. M., Rogers, A. A., Zurcher, J. D., Stockdale, L., & Booth, M. (2020). Does time spent using social media impact mental health?: An eight year longitudinal study. Computers in Human Behavior, 104, 106160. https://doi.org/10.1016/j.chb.2019.106160.
Deloitte. (2018). 2018 global mobile consumer survey: US edition. https://www2.deloitte.com/content/dam/Deloitte/us/Documents/technology-media-telecommunications/us-tmt-global-mobile-consumer-survey-exec-summary-2018.pdf.
Deloitte. (2019). Deloitte’s 2019 global mobile consumer survey. https://www2.deloitte.com/us/en/insights/industry/telecommunications/global-mobile-consumer-survey-2019.html.
Demirci, K., Akgönül, M., & Akpinar, A. (2015). Relationship of smartphone use severity with sleep quality, depression, and anxiety in university students. Journal of Behavioral Addictions, 4(2), 85–92. https://doi.org/10.1556/2006.4.2015.010.
Duttweiler, P. C. (1984). The Internal Control Index: A newly developed measure of locus of control. Educational and Psychological Measurement, 44(2), 209–221. https://doi.org/10.1177/0013164484442004.
Elhai, J. D., Dvorak, R. D., Levine, J. C., & Hall, B. J. (2017). Problematic smartphone use: A conceptual overview and systematic review of relations with anxiety and depression psychopathology. Journal of Affective Disorders, 207, 251–259. https://doi.org/10.1016/j.jad.2016.08.030.
Escobar-Viera, C. G., Shensa, A., Bowman, N. D., Sidani, J. E., Knight, J., James, A. E., & Primack, B. A. (2018). Passive and active social media use and depressive symptoms among United States adults. Cyberpsychology, Behavior, and Social Networking, 21(7), 437–443. https://doi.org/10.1089/cyber.2017.0668.
Eyal, N. (2014). Hooked: How to build habit-forming products. Penguin UK.
Eyal, N. (2019). Indistractable: How to control your attention and choose your life. BenBella Books.
Fitz, N., Kushlev, K., Jagannathan, R., Lewis, T., Paliwal, D., & Ariely, D. (2019). Batching smartphone notifications can improve well-being. Computers in Human Behavior, 101, 84–94. https://doi.org/10.1016/j.chb.2019.07.016.
Fogg, B. (2009). A behavior model for persuasive design. Proceedings of the 4th International Conference on Persuasive Technology – Persuasive ’09. https://doi.org/10.1145/1541948.1541999.
Fogg, B. J. (2019). Tiny habits: The small changes that change everything. Houghton Mifflin Harcourt.
GlobalWebIndex. (2021). Social. GlobalWebIndex’s Flagship Report on the Latest Trends in Social Media. https://www.gwi.com/reports/social.
Guthold, R., Stevens, G. A., Riley, L. M., & Bull, F. C. (2018). Worldwide trends in insufficient physical activity from 2001 to 2016: A pooled analysis of 358 population-based surveys with 1.9 million participants. The Lancet Global Health, 6(10), e1077–e1086. https://doi.org/10.1016/s2214-109x(18)30357-7.
Heintzelman, S. J., & Kushlev, K. (2020). Emphasizing scientific rigor in the development, testing, and implementation of positive psychological interventions. The Journal of Positive Psychology, 1–6. https://doi.org/10.1080/17439760.2020.1789701.
Heitmayer, M., & Lahlou, S. (2020). Why are smartphones disruptive? An empirical study of smartphone use in real-life contexts. Computers in Human Behavior, 106637. https://doi.org/10.1016/j.chb.2020.106637.
Hemphill, T. A., & Banerjee, S. (2021). Facebook and self-regulation: Efficacious proposals—Or ’smoke-and-mirrors’? Technology in Society, 101797.
Hiniker, A., Sobel, K., Suh, H., Sung, Y.-C., Lee, C. P., & Kientz, J. A. (2015). Texting while parenting. Proceedings of the 33rd Annual ACM Conference on Human Factors in Computing Systems — CHI ’15. https://doi.org/10.1145/2702123.2702199.
Holte, A. J., & Ferraro, F. R. (2020). True colors: Grayscale setting reduces screen time in college students. The Social Science Journal, 1–17. https://doi.org/10.1080/03623319.2020.1737461.
Holte, A. J., Giesen, D. T., & Ferraro, F. R. (2021). Color me calm: Grayscale phone setting reduces anxiety and problematic smartphone use. https://doi.org/10.1007/s12144-021-02020-y.
Hughes, N., & Burke, J. (2018). Sleeping with the frenemy: How restricting “bedroom use” of smartphones impacts happiness and wellbeing. Computers in Human Behavior, 85, 236–244. https://doi.org/10.1016/j.chb.2018.03.047.
Hunt, M. G., Marx, R., Lipson, C., & Young, J. (2018). No more FOMO: Limiting social media decreases loneliness and depression. Journal of Social and Clinical Psychology, 37(10), 751–768. doi: 10.1521/jscp.2018.37.10.751.
John, O. P., Donahue, E. M., & Kentle, R. L. (1991). Big Five Inventory. American Psychological Association (APA). https://doi.org/10.1037/t07550-000.
Kaye, L. K., Orben, A., Ellis, D. A., Hunter, S. C., & Houghton, S. (2020). The conceptual and methodological mayhem of ‘screen time.’ International Journal of Environmental Research and Public Health, 17(10), 3661. https://doi.org/10.3390/ijerph17103661.
Keyes, K. M., Maslowsky, J., Hamilton, A., & Schulenberg, J. (2015). The great sleep recession: Changes in sleep duration among US adolescents, 1991–2012. Pediatrics, 135(3), 460–468. https://doi.org/10.1542/peds.2014-2707.
Kim, J., Park, J., Lee, H., Ko, M., & Lee, U. (2019). LocknType: Lockout task intervention for discouraging smartphone app use. Proceedings of the 2019 Chi Conference on Human Factors in Computing Systems, 1–12. https://doi.org/10.1145/3290605.3300927.
Kirschner, P. A., & Karpinski, A. C. (2010). Facebook and academic performance. Computers in Human Behavior, 26(6), 1237–1245. https://doi.org/10.1016/j.chb.2010.03.024.
Ko, M., Yang, S., Lee, J., Heizmann, C., Jeong, J., Lee, U., Shin, D., Yatani, K., Song, J., & Chung, K.-M. (2015). NUGU: A group-based intervention app for improving self-regulation of limiting smartphone use. https://doi.org/10.1145/2675133.2675244.
Kushlev, K., Hunter, J. F., Proulx, J., Pressman, S. D., & Dunn, E. (2019). Smartphones reduce smiles between strangers. Computers in Human Behavior, 91, 12–16. https://doi.org/10.1016/j.chb.2018.09.023.
Kushlev, K., & Leitao, M. R. (2020). The effects of smartphones on well-being: Theoretical integration and research agenda. Current Opinion in Psychology, 36, 77–82. https://doi.org/10.1016/j.copsyc.2020.05.001.
Kwon, M., Kim, D.-J., Cho, H., & Yang, S. (2013). The smartphone addiction scale: Development and validation of a short version for adolescents. PLOS One, 8(12), e83558. https://doi.org/10.1371/journal.pone.0083558.
Lemola, S., Perkinson-Gloor, N., Brand, S., Dewald-Kaufmann, J. F., & Grob, A. (2014). Adolescents’ electronic media use at night, sleep disturbance, and depressive symptoms in the smartphone age. Journal of Youth and Adolescence, 44(2), 405–418. https://doi.org/10.1007/s10964-014-0176-x.
Li, J., Lepp, A., & Barkley, J. E. (2015). Locus of control and cell phone use: Implications for sleep quality, academic performance, and subjective well-being. Computers in Human Behavior, 52, 450–457. https://doi.org/10.1016/j.chb.2015.06.021.
Loid, K., Täht, K., & Rozgonjuk, D. (2020). Do pop-up notifications regarding smartphone use decrease screen time, phone checking behavior, and self-reported problematic smartphone use? Evidence from a two-month experimental study. Computers in Human Behavior, 102, 22–30. https://doi.org/10.1016/j.chb.2019.08.007.
Lukoff, K., Yu, C., Kientz, J., & Hiniker, A. (2018). What makes smartphone use meaningful or meaningless? Proceedings of the ACM on Interactive, Mobile, Wearable and Ubiquitous Technologies, 2(1), 1–26. https://doi.org/10.1145/3191754.
Mac Cárthaigh, S. (2020). The effectiveness of interventions to reduce excessive mobile device usage among adolescents: A systematic review. Neurology, Psychiatry and Brain Research, 35, 29–37. https://doi.org/10.1016/j.npbr.2019.11.002.
Mosquera, R., Odunowo, M., McNamara, T., Guo, X., & Petrie, R. (2019). The economic effects of Facebook. Experimental Economics, 23(2), 575–602. https://doi.org/10.1007/s10683-019-09625-y.
Myers, E., Drees, E. T., & Cain, J. (2021). Student experiences with an intervention utilizing the salience principle to reduce psychological attraction to smartphones. 8717. https://doi.org/10.5688/ajpe8717.
National Center for Statistics and Analysis. (2020). Distracted driving 2018. National Highway Traffic Safety Administration. https://crashstats.nhtsa.dot.gov/Api/Public/ViewPublication/812926.
Newport, C. (2019). Digital minimalism: Choosing a focused life in a noisy world. Portfolio.
Newzoo. (2021). Global mobile market report. https://newzoo.com/insights/trend-reports/newzoo-global-mobile-market-report-2021-free-version/.
Oberle, E., Ji, X. R., Kerai, S., Guhn, M., Schonert-Reichl, K. A., & Gadermann, A. M. (2020). Screen time and extracurricular activities as risk and protective factors for mental health in adolescence: A population-level study. Preventive Medicine, 141, 106291. https://doi.org/10.1016/j.ypmed.2020.106291.
O’Dea, S. (2021). Number of smartphone users worldwide from 2016 to 2021. Statista. https://www.statista.com/statistics/330695/number-of-smartphone-users-worldwide/.
Okeke, F., Sobolev, M., Dell, N., & Estrin, D. (2018). Good vibrations. Proceedings of the 20th International Conference on Human-Computer Interaction with Mobile Devices and Services, 1–12. https://doi.org/10.1145/3229434.3229463.
Olson, J. A., Stendel, M., & Veissière, S. (2020). Hypnotised by your phone? Smartphone addiction correlates with hypnotisability. Frontiers in Psychiatry, 11. https://doi.org/10.3389/fpsyt.2020.00578.
Olson, J. A., Lifshitz, M., Raz, A., & Veissière, S. P. L. (2021). Super placebos: A feasibility study combining contextual factors to promote placebo effects. Frontiers in Psychiatry, 12. https://doi.org/10.3389/fpsyt.2021.644825.
Olson, J. A., Nahas, J., Chmoulevitch, D., Cropper, S. J., & Webb, M. E. (2021). Naming unrelated words predicts creativity. Proceedings of the National Academy of Sciences, 118(25), e2022340118. https://doi.org/10.1073/pnas.2022340118.
Olson, J. A., Sandra, D. A., Langer, E. J., Raz, A., & Veissière, S. P. L. (2022). Creativity and smartphone use. PsyArXiv. https://doi.org/10.31234/osf.io/6grz7.
Olson, J. A., Sandra, D. A., S. Colucci, Bikaii, A. A., Chmoulevitch, D., Nahas, J., Raz, A., & Veissière, S. P. L. (2022). Smartphone addiction is increasing across the world: A meta-analysis of 24 countries. Computers in Human Behavior, 129, 107138. https://doi.org/10.1016/j.chb.2021.107138.
Orben, A., & Przybylski, A. K. (2019a). The association between adolescent well-being and digital technology use. Nature Human Behaviour, 3(2), 173–182. https://doi.org/10.1038/s41562-018-0506-1.
Orben, A., & Przybylski, A. K. (2020). Teenage sleep and technology engagement across the week. Peer Journal, 8, e8427. https://doi.org/10.7717/peerj.8427.
Orben, A., & Przybylski, A. K. (2019b). Screens, teens, and psychological well-being: Evidence from three time-use-diary studies. Psychological Science, 30(5), 682–696. https://doi.org/10.1177/0956797619830329.
Oulasvirta, A., Rattenbury, T., Ma, L., & Raita, E. (2011). Habits make smartphone use more pervasive. Personal and Ubiquitous Computing, 16(1), 105–114. https://doi.org/10.1007/s00779-011-0412-2.
Panova, T., Carbonell, X., Chamarro, A., & Puerta-Cortés, D. X. (2019). Specific smartphone uses and how they relate to anxiety and depression in university students: A cross-cultural perspective. Behaviour & Information Technology, 39(9), 944–956. https://doi.org/10.1080/0144929x.2019.1633405.
Perlman, D., Samost, A., Domel, A. G., Mehler, B., Dobres, J., & Reimer, B. (2019). The relative impact of smartwatch and smartphone use while driving on workload, attention, and driving performance. Applied Ergonomics, 75, 8–16. https://doi.org/10.1016/j.apergo.2018.09.001.
Przybylski, A. K. (2019). Digital screen time and pediatric sleep: Evidence from a preregistered cohort study. The Journal of Pediatrics, 205, 218-223.e1. https://doi.org/10.1016/j.jpeds.2018.09.054.
Rezaee, F., & Pedret, A. (2018). A critical review of silicon valley solutions for smartphone addiction. Idealogy, 3(3), 189–196.
Robertson, I. H., Manly, T., Andrade, J., Baddeley, B. T., & Yiend, J. (1997). “Oops!”: Performance correlates of everyday attentional failures in traumatic brain injured and normal subjects. Neuropsychologia, 35(6), 747–758. https://doi.org/10.1016/s0028-3932(97)00015-8.
Sarris, J., Thomson, R., Hargraves, F., Eaton, M., Manincor, M. de, Veronese, N., Solmi, M., Stubbs, B., Yung, A. R., & Firth, J. (2020). Multiple lifestyle factors and depressed mood: A cross-sectional and longitudinal analysis of the UK biobank (n = 84,860). BMC Medicine, 18(1). https://doi.org/10.1186/s12916-020-01813-5.
Stothart, C., Mitchum, A., & Yehnert, C. (2015). The attentional cost of receiving a cell phone notification. Journal of Experimental Psychology: Human Perception and Performance, 41(4), 893–897. https://doi.org/10.1037/xhp0000100.
Sunstein, C. R. (2021). The distributional effects of nudges. Nature Human Behaviour, 6(1), 9–10. https://doi.org/10.1038/s41562-021-01236-z.
Thaler, R. H., & Sunstein, C. R. (2021). Nudge. Yale University Press.
Thompson, E. R. (2007). Development and validation of an internationally reliable short-form of the Positive and Negative Affect Schedule (PANAS). Journal of Cross-Cultural Psychology, 38(2), 227–242. https://doi.org/10.1177/0022022106297301.
Throuvala, M. A., Griffiths, M. D., Rennoldson, M., & Kuss, D. J. (2020). Mind over matter: Testing the efficacy of an online randomized controlled trial to reduce distraction from smartphone use. International Journal of Environmental Research and Public Health, 17(13), 4842. https://doi.org/10.3390/ijerph17134842.
Twenge, J. M., Blake, A. B., Haidt, J., & Campbell, W. K. (2020). Commentary: Screens, teens, and psychological well-being: Evidence from three time-use-diary studies. Frontiers in Psychology, 11. https://doi.org/10.3389/fpsyg.2020.00181.
Twenge, J. M., Cooper, A. B., Joiner, T. E., Duffy, M. E., & Binau, S. G. (2019). Age, period, and cohort trends in mood disorder indicators and suicide-related outcomes in a nationally representative dataset, 20052017. Journal of Abnormal Psychology, 128(3), 185–199. https://doi.org/10.1037/abn0000410.
Twenge, J. M., Martin, G. N., & Campbell, W. K. (2018). Decreases in psychological well-being among American adolescents after 2012 and links to screen time during the rise of smartphone technology. Emotion, 18(6), 765–780. https://doi.org/10.1037/emo0000403.
Twenge, J. M., Spitzberg, B. H., & Campbell, W. K. (2019). Less in-person social interaction with peers among U.S. adolescents in the 21st century and links to loneliness. Journal of Social and Personal Relationships, 36(6), 1892–1913. https://doi.org/10.1177/0265407519836170.
Unsworth, N., Heitz, R. P., Schrock, J. C., & Engle, R. W. (2005). An automated version of the operation span task. Behavior Research Methods, 37(3), 498–505. https://doi.org/10.3758/bf03192720.
Veissière, S. P. L., & Stendel, M. (2018). Hypernatural monitoring: A social rehearsal account of smartphone addiction. Frontiers in Psychology, 9, 141.
Velthoven, M. H. van, Powell, J., & Powell, G. (2018). Problematic smartphone use: Digital approaches to an emerging public health problem. Digital Health, 4, 205520761875916. https://doi.org/10.1177/2055207618759167.
Ward, A. F., Duke, K., Gneezy, A., & Bos, M. W. (2017). Brain drain: The mere presence of one’s own smartphone reduces available cognitive capacity. Journal of the Association for Consumer Research, 2(2), 140–154. https://doi.org/10.1086/691462.
Wilmer, H. H., Sherman, L. E., & Chein, J. M. (2017). Smartphones and cognition: A review of research exploring the links between mobile technology habits and cognitive functioning. Frontiers in Psychology, 8, 1–16. https://doi.org/10.3389/fpsyg.2017.00605.
Zimmermann, L. (2021). “Your screen-time app is keeping track”: Consumers are happy to monitor but unlikely to reduce smartphone usage. Journal of the Association for Consumer Research, 6(3), 377–382. https://doi.org/10.1086/714365.
Zisapel, N., & Nir, T. (2003). Determination of the minimal clinically significant difference on a patient visual analog sleep quality scale. Journal of Sleep Research, 12(4), 291–298. https://doi.org/10.1046/j.0962-1105.2003.00365.x.
Acknowledgements
We would like to thank Johnny Nahas for helping run participants, Ceren Kaypak for acting as the psychiatrist, and Véronique Bohbot, Mariève Cyr, Suparna Choudhury, Ana María Ruiz-Ruano García, Ashesh Mukherjee, Jorge López Puga, Signy Sheldon, Gregory West, the Stanford Behavior Design Lab, and the Langer Mindfulness Lab for helpful discussions and feedback. We also thank Gordon Rose for inspiring interest in this topic.
Funding
This research was supported by the Canada First Research Excellence Fund, awarded to the Healthy Brains for Healthy Lives initiative (#3c-KM-10) at McGill University. JO acknowledges funding from the Fonds de recherche du Québec — Santé (FRQS).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Informed Consent
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000. Informed consent was obtained from all patients for being included in the study.
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original version of this article was revised: The fifth, sixth, and seventh sentences in the Procedure section for Study 2 were incorrect in the HTML version of this article as originally published and have been corrected.
Appendix
Appendix
Figures and Tables
Figure 3 shows the correlations between the measures. Tables 4 and 5 show the interventions used in the studies along with their compliance rates. Tables 6 and 7 show descriptive statistics.

Exploratory baseline correlations across both studies. There were notable positive correlations between problematic smartphone use, depression, and negative mood. ** p < .01, *** p < .001
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Olson, J.A., Sandra, D.A., Chmoulevitch, D. et al. A Nudge-Based Intervention to Reduce Problematic Smartphone Use: Randomised Controlled Trial. Int J Ment Health Addiction 21, 3842–3864 (2023). https://doi.org/10.1007/s11469-022-00826-w
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11469-022-00826-w