
Abstract
Objective
The objective of the study is to identify the efficacy and safety of combining laparoscopic adjustable gastric banding with repair of large para-oesophageal hernias.
Background
Para-oesophageal hernias are more common in the obese with higher recurrence rates following repair. The effect and safety of combining para-oesophageal hernia repair with laparoscopic adjustable gastric banding is unknown.
Methods
One-hundred fourteen consecutive patients undergoing primary laparoscopic adjustable gastric banding with concurrent repair of a large para-oesophageal hernia were prospectively identified and matched to a control group undergoing primary laparoscopic adjustable gastric banding only. Weight loss and complication data were retrieved from a prospectively maintained database, and a standardised bariatric outcome questionnaire was used to assess post-operative symptoms, satisfaction with surgery and satiety scores.
Results
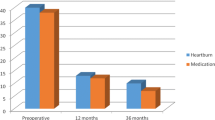
At a mean follow up of 4.9 ± 2.1 years, total weight loss was 16.4 ± 9.9 % in the hernia repair group and 17.6 ± 12.6 % in the control group (p = 0.949), with 17 vs. 11 % loss to follow up rates (p = 0.246). No statistically significant difference in revisional surgery rate and symptomatic recurrence of hiatal hernia was documented in four patients in the hernia repair group (3.5 %). No statistically significant difference in mean reflux (9.9 vs. 10.3, p = 0.821), dysphagia (20.7 vs. 20.1, p = 0.630) or satiety scores was identified.
Conclusions
Concurrent repair of large para-oesophageal hiatal hernia and laparoscopic adjustable gastric banding placement is safe and effective both in terms of symptom control and weight loss over the intermediate term. In obese patients with large hiatal hernias, consideration should be given to combining repair of the hernia with a bariatric procedure.

Similar content being viewed by others

References
Aly A, Munt J, Jamieson GG, et al. Laparoscopic repair of large hiatal hernias. Bri J Surg. 2005;92(5):648–53.
Dallemagne B, Kohnen L, Perretta S, et al. Laparoscopic repair of paraesophageal hernia. Long-term follow-up reveals good clinical outcome despite high radiological recurrence rate. Ann Surg. 2011;253(2):291–6.
Mattar SG, Bowers SP, Galloway KD, et al. Long-term outcome of laparoscopic repair of paraesophageal hernia. Surg Endosc. 2002;16(5):745–9.
Hashemi M, Peters JH, DeMeester TR, et al. Laparoscopic repair of large type III hiatal hernia: objective followup reveals high recurrence rate. J Am Coll Surg. 2000;190(5):553–60. discussion 60–1.
Khaitan L, Houston H, Sharp K, et al. Laparoscopic paraesophageal hernia repair has an acceptable recurrence rate. Am Surg. 2002;68(6):546–51. discussion 51–2.
Davis Jr SS. Current controversies in paraesophageal hernia repair. Surg Clin N Am. 2008;88(5):959–78. vi.
El-Serag H. The association between obesity and GERD: a review of the epidemiological evidence. Dig Dis Sci. 2008;53(9):2307–12.
Eusebi LH, Fuccio L, Bazzoli F. The role of obesity in gastroesophageal reflux disease and Barrett’s esophagus. Dig Dis (Basel, Switzerland). 2012;30(2):154–7.
Wilson LJ, Ma W, Hirschowitz BI. Association of obesity with hiatal hernia and esophagitis. Am J Gastroenterol. 1999;94(10):2840–4.
Pandolfino JE, Ghosh SK, Lodhia N, et al. Utilizing intraluminal pressure gradients to predict esophageal clearance: a validation study. Am J Gastroenterol. 2008;103(8):1898–905.
Suter M, Dorta G, Giusti V, et al. Gastro-esophageal reflux and esophageal motility disorders in morbidly obese patients. Obes Surg. 2004;14(7):959–66.
Perez AR, Moncure AC, Rattner DW. Obesity adversely affects the outcome of antireflux operations. Surg Endosc. 2001;15(9):986–9.
Morgenthal CB, Lin E, Shane MD, et al. Who will fail laparoscopic Nissen fundoplication? Preoperative prediction of long-term outcomes. Surg Endosc. 2007;21(11):1978–84.
Anvari M, Bamehriz F. Outcome of laparoscopic Nissen fundoplication in patients with body mass index > or = 35. Surg Endosc. 2006;20(2):230–4.
Tekin K, Toydemir T, Yerdel MA. Is laparoscopic antireflux surgery safe and effective in obese patients? Surg Endosc. 2012;26(1):86–95.
O’Brien PE, MacDonald L, Anderson M, et al. Long-term outcomes after bariatric surgery: fifteen-year follow-up of adjustable gastric banding and a systematic review of the bariatric surgical literature. Ann Surg. 2013;257(1):87–94.
O’Brien PE, Dixon JB. Lap-band: outcomes and results. J Laparoendosc Adv Surg Tech. 2003;13(4):265–70.
Peeters A, O’Brien PE, Laurie C, et al. Substantial intentional weight loss and mortality in the severely obese. Ann Surg. 2007;246(6):1028–33.
Menon S, Trudgill N. Risk factors in the aetiology of hiatus hernia: a meta-analysis. Eur J Gastroenterol Hepatol. 2011;23(2):133–8.
Kasotakis G, Mittal SK, Sudan R. Combined treatment of symptomatic massive paraesophageal hernia in the morbidly obese. J Soc Laparoendosc Surgeons. 2011;15(2):188–92.
Pham DV, Protyniak B, Binenbaum SJ, et al. Simultaneous laparoscopic paraesophageal hernia repair and sleeve gastrectomy in the morbidly obese. Surg Obes Relat Dis : Off J Am Soc Bariatric Surg. 2014;10(2):257–61.
Merchant AM, Cook MW, Srinivasan J, et al. Comparison between laparoscopic paraesophageal hernia repair with sleeve gastrectomy and paraesophageal hernia repair alone in morbidly obese patients. Am Surg. 2009;75(7):620–5.
Patel AD, Lin E, Lytle NW, et al. Combining laparoscopic giant paraesophageal hernia repair with sleeve gastrectomy in obese patients. Surg Endosc. 2014;29(5):1115–22.
Chaudhry UI, Marr BM, Osayi SN, et al. Laparoscopic Roux-en-Y gastric bypass for treatment of symptomatic paraesophageal hernia in the morbidly obese: medium-term results. Surg Obes Relat Dis : Off J Am Soc Bariatric Surg. 2014;10(6):1063–7.
Cuenca-Abente F, Parra JD, Oelschlager BK. Laparoscopic sleeve gastrectomy: an alternative for recurrent paraesophageal hernias in obese patients. J Soc Laparoendosc Surgeons / Soc Laparoendosc Surgeons. 2006;10(1):86–9.
Amini A, Vaziri K, Nagle AP. Simultaneous laparoscopic type III paraesophageal hernia repair with porcine small intestine submucosa and Roux-en-Y gastric bypass. Surg Obes Relat Dis : Off J Am Soc Bariatric Surg. 2008;4(6):764–7.
Korwar V, Peters M, Adjepong S, et al. Laparoscopic hiatus hernia repair and simultaneous sleeve gastrectomy: a novel approach in the treatment of gastroesophageal reflux disease associated with morbid obesity. J Laparoendosc Adv Surg Tech Part A. 2009;19(6):761–3.
Salvador-Sanchis JL, Martinez-Ramos D, Herfarth A, et al. Treatment of morbid obesity and hiatal paraesophageal hernia by laparoscopic Roux-en-Y gastric bypass. Obes Surg. 2010;20(6):801–3.
Rodriguez JH, Kroh M, El-Hayek K, et al. Combined paraesophageal hernia repair and partial longitudinal gastrectomy in obese patients with symptomatic paraesophageal hernias. Surg Endosc. 2012;26(12):3382–90.
Landen S. Simultaneous paraesophageal hernia repair and gastric banding. Obes Surg. 2005;15(3):435–8.
Bernante P, Breda C, Zangrandi F, et al. Emergency sleeve gastrectomy as rescue treatment for acute gastric necrosis due to type II paraesophageal hernia in an obese woman with gastric banding. Obes Surg. 2008;18(6):737–41.
Burton PR, Brown WA, Laurie C, et al. The effect of laparoscopic adjustable gastric bands on esophageal motility and the gastroesophageal junction; analysis using high resolution video manometry. Obes Surg. 2009;19(7):905–14.
Burton PR, Brown WA. The mechanism of weight loss with laparoscopic adjustable gastric banding: induction of satiety not restriction. Int J Obes (2005). 2011;35 Suppl 3:S26–30.
Egberts K, Brown WA, O’Brien PE. Systematic review of erosion after laparoscopic adjustable gastric banding. Obes Surg. 2011;21(8):1272–9.
Angrisani L, Di Lorenzo N, Favretti F, et al. The Italian Group for LAP-BAND: predictive value of initial body mass index for weight loss after 5 years of follow-up. Surg Endosc. 2004;18(10):1524–7.
O’Brien PE, Brown WA, Smith A, et al. Prospective study of a laparoscopically placed, adjustable gastric band in the treatment of morbid obesity. Br J Surg. 1999;86(1):113–8.
Fielding GA, Allen JW. A step-by-step guide to placement of the LAP-BAND adjustable gastric banding system. Am J Surg. 2002;184(6b):26s–30s.
Burton PR, Brown W, Laurie C, et al. Outcomes, satiety, and adverse upper gastrointestinal symptoms following laparoscopic adjustable gastric banding. Obes Surg. 2011;21(5):574–81.
Maddern GJ, Chatterton BE, Collins PJ, et al. Solid and liquid gastric emptying in patients with gastro-oesophageal reflux. Br J Surg. 1985;72(5):344–7.
Dakkak M, Bennett JR. A new dysphagia score with objective validation. J Clin Gastroenterol. 1992;14(2):99–100.
Vakil N, Shaw M, Kirby R. Clinical effectiveness of laparoscopic fundoplication in a U.S. community. Am J Med. 2003;114(1):1–5.
Disclosure Statement
The Centre for Obesity Research and Education has received funding for research purposes from Allergan, Inc., the manufacturer of the LAP-BAND. The authors declare that they have no additional conflicts of interest.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Long, A.J., Burton, P.R., Laurie, C.P. et al. Concurrent Large Para-oesophageal Hiatal Hernia Repair and Laparoscopic Adjustable Gastric Banding: Results from 5-year Follow Up. OBES SURG 26, 1090–1096 (2016). https://doi.org/10.1007/s11695-015-1881-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-015-1881-6