
Abstract
Background
Liver disease is associated with altered serum osmolality, increased thrombin generation, and systemic inflammation, all of which may contribute to perihematomal edema (PHE) after intracerebral hemorrhage (ICH). We evaluated the association between a validated liver fibrosis index and PHE growth in a cohort of patients with primary ICH.
Methods
We performed a retrospective cohort study using data from the Virtual International Stroke Trials Archive-ICH. We included adult patients with primary ICH presenting within 6 h of symptom onset. The exposure of interest was the Fibrosis-4 (FIB-4) score, a validated liver fibrosis index; this was modeled as a continuous variable. The primary outcome was absolute PHE growth over 96 h. Secondary outcomes were absolute admission and 96-h PHE volumes. We used multiple linear regression models adjusted for established determinants of PHE. In a secondary analysis, the FIB-4 score was modeled as a categorical variable to compare patients with versus without liver fibrosis.
Results
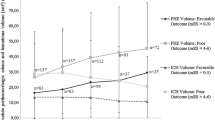
Among 354 patients with ICH, 8% had evidence of liver fibrosis based on a validated cutoff. The FIB-4 score was not associated with PHE growth in unadjusted (β, 0.03; 95% CI, − 0.01 to 0.12) or adjusted models (β, 0.04; 95% CI, − 0.03 to 0.13). In a secondary analysis treating FIB-4 as a categorical variable, patients with liver fibrosis did not have greater PHE growth than those without liver fibrosis. FIB-4 score was also not associated with absolute admission or 96-h PHE volumes.
Conclusions
In a multicenter cohort of patients with primary intracerebral hemorrhage, a liver fibrosis score was not associated with PHE volume or growth.


Similar content being viewed by others


References
Cusack TJ, Carhuapoma JR, Ziai WC. Update on the treatment of spontaneous intraparenchymal hemorrhage: medical and interventional management. Curr Treat Options Neurol. 2018;20:1.
Gross BA, Jankowitz BT, Friedlander RM. Cerebral intraparenchymal hemorrhage: a review. JAMA J Am Med Assoc. 2019;321:1295–303.
Urday S, Kimberly WT, Beslow LA, et al. Targeting secondary injury in intracerebral haemorrhage–perihaematomal oedema. Nat Rev Neurol. 2015;11:111–22.
Murthy SB, Moradiya Y, Dawson J, et al. Perihematomal edema and functional outcomes in intracerebral hemorrhage: influence of hematoma volume and location. Stroke. 2015;46:3088–92.
Liotta EM, Romanova AL, Lizza BD, et al. Osmotic shifts, cerebral edema, and neurologic deterioration in severe hepatic encephalopathy. Crit Care Med. 2018;46:280–9.
Córdoba J, García-Martinez R, Simón-Talero M. Hyponatremic and hepatic encephalopathies: similarities, differences and coexistence. Metab Brain Dis. 2010;25:73–80.
Bos S, van den Boom B, Kamphuisen PW, et al. Haemostatic profiles are similar across all aetiologies of cirrhosis. Thromb Haemost. 2019;119:246–53.
Yoneda M, Mawatari H, Fujita K, et al. High-sensitivity C-reactive protein is an independent clinical feature of nonalcoholic steatohepatitis (NASH) and also of the severity of fibrosis in NASH. J Gastroenterol. 2007;42:573–82.
Khoury T, Mari A, Nseir W, Kadah A, Sbeit W, Mahamid M. Neutrophil-to-lymphocyte ratio is independently associated with inflammatory activity and fibrosis grade in nonalcoholic fatty liver disease. Eur J Gastroenterol Hepatol. 2019;31:1110–5.
Caballería L, Pera G, Arteaga I, et al. High prevalence of liver fibrosis among European adults with unknown liver disease: a population-based study. Clin Gastroenterol Hepatol. 2018;16(1138–45):e5.
Watt GP, Lee M, Pan JJ, et al. High prevalence of hepatic fibrosis, measured by elastography, in a population-based study of Mexican Americans. Clin Gastroenterol Hepatol. 2019;17(968–75):e5.
Roulot D, Costes JL, Buyck JF, et al. Transient elastography as a screening tool for liver fibrosis and cirrhosis in a community-based population aged over 45 years. Gut. 2011;60:977–84.
Ostovaneh MR, Ambale-Venkatesh B, Fuji T, et al. Association of liver fibrosis with cardiovascular diseases in the general population: the multi-ethnic study of atherosclerosis (MESA). Circ Cardiovasc Imaging. 2018;11:e007241.
Parikh NS, Kamel H, Navi BB, et al. Liver fibrosis indices and outcomes after primary intracerebral hemorrhage. Stroke. 2020;51:830–7.
Ali M, Bath P, Brady M, et al. Development, expansion, and use of a stroke clinical trials resource for novel exploratory analyses. Int J Stroke. 2012;7:133–8.
Kabbany MN, Conjeevaram Selvakumar PK, Watt K, et al. Prevalence of nonalcoholic steatohepatitis-associated cirrhosis in the United States: an analysis of national health and nutrition examination survey data. Am J Gastroenterol. 2017;112:581–7.
Lin ZH, Xin YN, Dong QJ, et al. Performance of the aspartate aminotransferase-to-platelet ratio index for the staging of hepatitis C-related fibrosis: an updated meta-analysis. Hepatology. 2011;53:726–36.
Kim BK, Kim DY, Park JY, et al. Validation of FIB-4 and comparison with other simple noninvasive indices for predicting liver fibrosis and cirrhosis in hepatitis B virus-infected patients. Liver Int. 2010;30:546–53.
Naveau S, Gaudé G, Asnacios A, et al. Diagnostic and prognostic values of noninvasive biomarkers of fibrosis in patients with alcoholic liver disease. Hepatology. 2009;49:97–105.
Xiao G, Zhu S, Xiao X, Yan L, Yang J, Wu G. Comparison of laboratory tests, ultrasound, or magnetic resonance elastography to detect fibrosis in patients with nonalcoholic fatty liver disease: a meta-analysis. Hepatology. 2017;66:1486–501.
Sterling RK, Lissen E, Clumeck N, et al. Development of a simple noninvasive index to predict significant fibrosis in patients with HIV/HCV coinfection. Hepatology. 2006;43:1317–25.
Murthy SB, Urday S, Beslow LA, et al. Rate of perihaematomal oedema expansion is associated with poor clinical outcomes in intracerebral haemorrhage. J Neurol Neurosurg Psychiatry. 2016;87:1169–73.
Urday S, Beslow LA, Goldstein DW, et al. Measurement of perihematomal edema in intracerebral hemorrhage. Stroke. 2015;46:1116–9.
Parikh NS, Merkler AE, Schneider Y, Navi BB, Kamel H. Discharge disposition after stroke in patients with liver disease. Stroke. 2017;48:476–8.
Hoya K, Tanaka Y, Uchida T, et al. Intracerebral hemorrhage in patients with chronic liver disease. Neurol Med Chir (Tokyo). 2012;52:181–5.
Morotti A, Marini S, Lena UK, et al. Significance of admission hypoalbuminemia in acute intracerebral hemorrhage. J Neurol. 2017;264:905–11.
Di Napoli M, Behrouz R, Topel CH, et al. Hypoalbuminemia, systemic inflammatory response syndrome, and functional outcome in intracerebral hemorrhage. J Crit Care. 2017;41:247–53.
McPherson S, Hardy T, Dufour JF, et al. Age as a confounding factor for the accurate non-invasive diagnosis of advanced NAFLD fibrosis. Am J Gastroenterol. 2017;112:740–51.
Acknowledgements
VISTA-ICH Steering Committee
VISTA-ICH Steering Committee Collaborators: D.F. Hanley (Chair), K. Butcher, S. Davis, B. Gregson, K.R. Lees, P. Lyden, S. Mayer, K. Muir, and T. Steiner.
Funding
Dr. Parikh was supported by the Leon Levy Foundation, the New York State Department of Health Empire Clinical Research Investigator Program, and the Florence Gould Foundation. Dr. Jesudian has funding from the Society of Interventional Radiology Foundation. Dr. Kamel is supported by NINDS Grants R01NS097443 and U01NS095869 and the Michael Goldberg Research Fund. Dr. Hanley is supported by the NIH (1U01NS080824, U24TR001609). Dr. Ziai is supported by NIH 1U01NS080824. Dr. Murthy is funded by NINDS Grant K23NS105948 and the Leon Levy Foundation.
Author information
Authors and Affiliations
Consortia
Contributions
This study was conceptualized by NSP, HK, and SBM. Acquisition of data was done by SBM, and SBM was responsible for the analysis. NSP, AJ, HK, DFH, WCZ, and SBM interpreted the data. NSP and SBM were responsible for drafting the article, and AJ, HK, DFH, and WCZ were responsible for critical revision for important intellecutal content. All authors approved the final version of this manuscript for publication.
Corresponding author
Ethics declarations
Conflicts of interest
Dr. Parikh, Dr. Jesudian, Dr. Murthy: none. Hooman Kamel serves as the co-PI for the NIH-funded ARCADIA trial which receives in-kind study drug from the BMS-Pfizer Alliance and in-kind study assays from Roche Diagnostics, serves as a steering committee member of Medtronic’s Stroke AF trial (uncompensated), serves on an endpoint adjudication committee for a trial of empagliflozin for Boehringer Ingelheim, and has served on an advisory board for Roivant Sciences related to Factor XI inhibition. Dr. Hanley reports personal fees from Op2Lysis, personal fees from BrainScope, personal fees from Neurotrope, and non-financial support from Genentech outside the submitted work. Dr, Ziai receives consulting fees from C.R. Bard, Inc., and Portola Pharmaceuticals, Inc., outside of the area of work commented on here.
Ethical Approval
Trials included in the VISTA-ICH cohort were performed with institutional review board and/or regulatory approval, and our analysis was approved by the Weill Cornell Medicine Institutional Review Board.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Parikh, N.S., Jesudian, A., Kamel, H. et al. Liver Fibrosis and Perihematomal Edema Growth in Primary Intracerebral Hemorrhage. Neurocrit Care 34, 983–989 (2021). https://doi.org/10.1007/s12028-020-01081-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-020-01081-4