
Abstract
Antithrombotic drug use for acute coronary syndromes (ACS) varies considerably. The number of antithrombotic drugs (excluding oral anticoagulants) used pre- and in-hospital was recorded in ACS survivors enrolled at hospital discharge in the long-tErm follow-uP of antithrombotic management patterns In acute CORonary syndrome patients (EPICOR) registry (NCT01171404), a prospective cohort study. Among 10,568 patients, the number of antithrombotic drugs used early/patient ranged from 0 to 8 (interquartile range = 3–4). Overall, 250 patients (2.4%) experienced ≥ 1 in-hospital ischemic event and 343 (3.2%) ≥ 1 non-fatal bleeding event. While there was no difference in the rate of ischemic events (p = 0.75 for-trend) according to the number of antithrombotic drugs, a significantly higher incidence of non-fatal bleeds was observed (p < 0.0001 for-trend), with OR = 1.68 (95%CI = 1.51–1.88) per additional antithrombotic drug, which remained after adjustment by patient characteristics. In conclusion, careful balancing of the short-term risks for ischemic and bleeding events should be considered when adding new antithrombotic drugs.
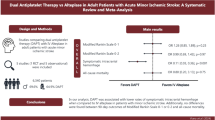
Graphical abstract


Similar content being viewed by others


Abbreviations
- ACS:
-
Acute coronary syndromes
- EPICOR:
-
Long-tErm follow-uP of antithrombotic management patterns In acute CORonary syndrome patients
- LMWH:
-
Low molecular weight heparin
- NSTEMI:
-
Non-ST-segment elevation myocardial infarction
- STEMI:
-
ST-segment elevation myocardial infarction
- UFH:
-
Unfractionated heparin
References
Rossello, X., Lobo-Gonzalez, M., & Ibanez, B. (2019). Editor’s choice- pathophysiology and therapy of myocardial ischaemia/reperfusion syndrome. European Heart Journal: Acute Cardiovascular Care, 8(5), 443–456. https://doi.org/10.1177/2048872619845283.
Rossello, X., Pocock, S. J., & Julian, D. G. (2015). Long-term use of cardiovascular drugs. Journal of the American College of Cardiology, 66(11), 1273–1285. https://doi.org/10.1016/j.jacc.2015.07.018.
Ibanez, B., James, S., Agewall, S., Antunes, M. J., Bucciarelli-Ducci, C., Bueno, H., et al. (2017). 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. European Heart Journal, 39(2), 119–177. https://doi.org/10.1093/eurheartj/ehx393.
Roffi, M., Patrono, C., Collet, J.-P., Mueller, C., Valgimigli, M., Andreotti, F., et al. (2016). 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. European Heart Journal, 37(3), 267–315. https://doi.org/10.1093/eurheartj/ehv320.
Amsterdam, E. A., Wenger, N. K., Brindis, R. G., Casey, D. E., Ganiats, T. G., Holmes, D. R., et al. (2014). 2014 AHA/ACC Guideline for the management of patients with non–ST-elevation acute coronary syndromes. Journal of the American College of Cardiology, 64(24), e139–e228. https://doi.org/10.1016/j.jacc.2014.09.017.
O’Gara, P. T., Kushner, F. G., Ascheim, D. D., Casey, D. E., Chung, M. K., de Lemos, J. A., … Yancy, C. W. (2013). 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Journal of the American College of Cardiology, 61(4), e78-140. https://doi.org/10.1016/j.jacc.2012.11.019
Rollini, F., Franchi, F., & Angiolillo, D. J. (2016, January 1). Switching P2Y12-receptor inhibitors in patients with coronary artery disease. Nature Reviews Cardiology. Nature Publishing Group. https://doi.org/10.1038/nrcardio.2015.113.
Bueno, H., Danchin, N., Tafalla, M., Bernaud, C., Annemans, L., & Van de Werf, F. (2013). EPICOR (long-tErm follow-up of antithrombotic management Patterns In acute CORonary syndrome patients) study: rationale, design, and baseline characteristics. American heart journal, 165(1), 8–14. https://doi.org/10.1016/j.ahj.2012.10.018.
Bueno, H., Pocock, S., Danchin, N., Annemans, L., Gregson, J., Medina, J., & Van de Werf, F. (2017). International patterns of dual antiplatelet therapy duration after acute coronary syndromes. Heart, 103(2), 132–138. https://doi.org/10.1136/heartjnl-2016-309509.
Rosselló, X., Huo, Y., Pocock, S., Van de Werf, F., Chin, C. T., Danchin, N., et al. (2017). Global geographical variations in ST-segment elevation myocardial infarction management and post-discharge mortality. International Journal of Cardiology, 245, 27–34. https://doi.org/10.1016/j.ijcard.2017.07.039.
Bueno, H., Rossello, X., Pocock, S., Van de Werf, F., Chin, C. T., Danchin, N., et al. (2018). Regional variations in hospital management and post-discharge mortality in patients with non-ST-segment elevation acute coronary syndrome. Clinical Research in Cardiology, 107(9), 836–844. https://doi.org/10.1007/s00392-018-1254-y.
White, I. R., Royston, P., & Wood, A. M. (2011). Multiple imputation using chained equations: Issues and guidance for practice. Statistics in medicine, 30(4), 377–399. https://doi.org/10.1002/sim.4067.
Pocock, S. J., Huo, Y., Van de Werf, F., Newsome, S., Chin, C. T., Vega, A. M., et al. (2019). Predicting two-year mortality from discharge after acute coronary syndrome: an internationally-based risk score. European Heart Journal: Acute Cardiovascular Care, 8(8), 727–737. https://doi.org/10.1177/2048872617719638.
Bueno, H., Rossello, X., Pocock, S. J., Van de Werf, F., Chin, C. T., Danchin, N., et al. (2019). In-hospital coronary revascularization rates and post-discharge mortality risk in non–ST-segment elevation acute coronary syndrome. Journal of the American College of Cardiology, 74(11), 1454–1461. https://doi.org/10.1016/j.jacc.2019.06.068.
Bueno, H., Sinnaeve, P., Annemans, L., Danchin, N., Licour, M., Medina, J., et al. (2016). Opportunities for improvement in anti-thrombotic therapy and other strategies for the management of acute coronary syndromes: insights from EPICOR, an international study of current practice patterns. European heart journal. Acute cardiovascular care, 5(1), 3–12. https://doi.org/10.1177/2048872614565912.
Raposeiras-Roubín, S., Abu-Assi, E., Muñoz-Pousa, I., Rossello, X., Cespón-Fernández, M., Melendo Viu, M., et al. (2020). Usefulness of bleeding after acute coronary syndromes for unmasking silent cancer. American Journal of Cardiology, 125(12), 1801–1808. https://doi.org/10.1016/j.amjcard.2020.03.023.
Eikelboom, J. W., Mehta, S. R., Anand, S. S., Xie, C., Fox, K. A. A., & Yusuf, S. (2006). Adverse impact of bleeding on prognosis in patients with acute coronary syndromes. Circulation, 114(8), 774–782. https://doi.org/10.1161/CIRCULATIONAHA.106.612812.
Erdem, G., & Flather, M. (2012). Assessing bleeding risk in acute coronary syndromes. Revista Espanola de Cardiologia, 65(1), 4–6. https://doi.org/10.1016/j.recesp.2011.08.005.
Steg, P. G., Huber, K., Andreotti, F., Arnesen, H., Atar, D., Badimon, L., et al. (2011). Bleeding in acute coronary syndromes and percutaneous coronary interventions: position paper by the Working Group on Thrombosis of the European Society of Cardiology. European heart journal, 32(15), 1854–1864. https://doi.org/10.1093/eurheartj/ehr204.
Valgimigli, M., Bueno, H., Byrne, R. A., Collet, J.-P., Costa, F., Jeppsson, A., et al. (2018). 2017 ESC focused update on dual antiplatelet therapy in coronary artery disease developed in collaboration with EACTS: the Task Force for dual antiplatelet therapy in coronary artery disease of the European Society of Cardiology (ESC) and of the European Association for Cardio-Thoracic Surgery (EACTS). European heart journal, 39(3), 213–260. https://doi.org/10.1093/eurheartj/ehx419.
Angiolillo, D. J., Rollini, F., Storey, R. F., Bhatt, D. L., James, S., Schneider, D. J., et al. (2017). International expert consensus on switching platelet P2Y12 receptor-inhibiting therapies. Circulation, 136(20), 1955–1975. https://doi.org/10.1161/CIRCULATIONAHA.117.031164.
Rossello, X., Medina, J., Pocock, S., Van de Werf, F., Chin, C. T., Danchin, N., et al. (2020). Assessment of quality indicators for acute myocardial infarction management in 28 countries and use of composite quality indicators for benchmarking. European Heart Journal: Acute Cardiovascular Care, 9(8), 911–922. https://doi.org/10.1177/2048872620911853.
Acknowledgments
XR has received support from the SEC-CNIC CARDIOJOVEN fellowship programme. Medical writing support was provided by Paragon, Knutsford, UK, in accordance with Good Publication Practice guidelines.
Funding
This study was funded by AstraZeneca (no grant number available). Support from the funder included development of the study design, collection and analysis of data, and provision of medical writing support during manuscript development. Being a non-interventional study, no drugs were supplied or funded.
Author information
Authors and Affiliations
Contributions
RMA and HB worked on conception of the study; JG, SP, and XR made the statistical analyses; RMA, SP, and HB contributed to the analysis and interpretation of the data; RMA and HB drafted the paper; RMA, JG, XR, FVdW, JM, ND, SP, and HB worked on further drafting and revising the paper critically. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethical Standards
No animal studies were carried out by the authors for this article. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Conflict of Interest
RMA has received consulting fees from AstraZeneca and Bayer, and speaking fees or support for attending scientific meetings from Daichii-Sankyo, Bayer, and Cardiome. JG has received grants from AstraZeneca during the conduct of the study and outside of the submitted work. XR has nothing to disclose. FVdW has received consulting fees and research grants from Boehringer Ingelheim and Merck, and consulting fees from Roche, Sanofi Aventis, AstraZeneca, and The Medicines Company. JM is an employee of AstraZeneca. ND has received consulting or speaking fees from Amgen, AstraZeneca, Bayer, Bristol-Myers Squibb, Boehringer Ingelheim, GlaxoSmithKline, Intercept, MSD, Novartis, Novo-Nordisk, Pfizer, Sanofi, and Servier. SP has received research grant support from AstraZeneca. HB has received research funding from the Instituto de Salud Carlos III (PIE16/00021), AstraZeneca, BMS, Janssen, and Novartis; consulting fees from Abbott, AstraZeneca, Bayer, BMS-Pfizer, and Novartis; and speaking fees or support for attending scientific meetings from AstraZeneca, Bayer, BMS-Pfizer, Ferrer, Novartis, Servier, and MEDSCAPE-the heart.org.
Additional information
Associate Editor Paul J. R. Barton oversaw the review of this article
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Martín-Asenjo, R., Gregson, J., Rossello, X. et al. Number of Antithrombotic Drugs Used Early and In-hospital Outcomes in Acute Coronary Syndromes. J. of Cardiovasc. Trans. Res. 14, 790–798 (2021). https://doi.org/10.1007/s12265-020-10094-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12265-020-10094-5