
Abstract
Mammographic density (MD) is a strong independent risk factor for breast cancer. It has been suggested that breast cancer is related to the exposure to circulating sex hormones. However, relations between MD and hormones have been inconsistent. In addition, such relations are mainly evaluated in Western populations. Therefore, we conducted a cross-sectional study in 396 cancer-free postmenopausal Korean women who had never used hormone replacement therapy. We assayed estradiol, testosterone, and sex hormone-binding globulin (SHBG) levels. We then calculated free testosterone (cFT) levels. Total and dense areas of digital mammogram were measured using a computer-assisted thresholding method, and non-dense area and percent dense area were calculated. Linear mixed model was used for analyses. Estradiol and testosterone levels were not associated with any MD measures after adjusting for reproductive factors and body mass index. However, cFT was persistently associated with non-dense area even after adjusting for covariates, with non-dense area increased by 3.5% per 1 standard deviation increase of cFT. SHBG showed an inverse association with non-dense area, although it showed a positive association with dense area and percent dense area regardless of adjustment for covariates. Non-dense area was decreased by 5.6% while percent dense area was increased by 13.4% per 1 standard deviation increase of SHBG. These findings suggest that SHBG might be related with breast cancer risk, probably through its association with breast density.
Similar content being viewed by others


Introduction
Mammographic density (MD) that radiologically reflects proliferation of the breast parenchyma has been consistently associated with female breast cancer risk in diverse ethnic populations [1,2,3,4]. MD has been associated with several reproductive and menstrual risk factors of breast cancer. It has been suggested that breast cancer is probably related to exposure to endogenous estrogen, including nulliparity, late age at menopause, and late age at first pregnancy [5,6,7]. In a co-twin control study of Korean female twins that allowed complete elimination of genetic influence on MD, percent dense area (PDA) of mammogram was found to be inversely associated with age at the first full-term childbirth and parity after adjusting for body mass index (BMI), although such associations were marginally significant [7].
Given associations of MD with both breast cancer and sex hormone-related risk factors of breast cancer, sex hormones might be involved in breast cancer development through their proliferative effect on breast tissue that may be reflected in high breast density [8, 9]. However, relations between circulating sex hormones and MD were inconsistent between studies in both premenopausal women [9,10,11,12,13] and postmenopausal women [14,15,16,17,18,19,20,21,22,23]. Therefore, it remains uncertain whether circulating sex hormone level is directly associated with MD and plays a role as an intermediate phenotype that integrates the effect of sex hormones on breast cancer risk [24]. In addition, relations between MD and circulating hormones in Asian women have been scarcely evaluated.
To improve understanding of biological mechanisms that underlie relations among sex hormone, MD, and breast cancer, we evaluated the association between circulating sex hormones and MD in postmenopausal Korean women whose sex hormone levels were less likely to fluctuate.
Materials and Methods
Study Participants
Study subjects were 396 postmenopausal women who had never used hormone replacement therapy and had undertaken mammogram with measurement of circulating sex hormones when they participated in the Healthy Twin study between April 2005 and January 2009. The Healthy Twin study was conducted as a part of the Korean Genome Epidemiology Study. It recruited Korean like-sex adult twins over 30 years of age and their first-degree adult family members nationwide. Details of the Healthy Twin study have been published previously [25].
Among the initial 512 women with available MD measurement and sex hormone data, we included 396 women in final analysis after excluding 116 women for the following reasons: breast cancer (one woman), did not fulfill operational criteria for postmenopausal status (86 women), ever use of hormone replacement (22 women), and higher (> 55 pg/mL) estradiol levels (7 women). We considered the subject as postmenopausal if she reported no menstrual cycle within the past 12 months and fulfilled one of the following criteria: who reported natural menopause, who had undertaken bilateral oophorectomy, who were 55 years of age or older.
Study Variables
Mammograms were taken in a study center using the same full-field digital mammography system (Senographe 2000D/DMR/DS, General Electric Company, Milwaukee, WI, USA). MD was measured in a right cranio-caudal view of the mammogram using a computer-assisted thresholding technique (Cumulus) by a single observer who was blinded to sex hormone levels and all identifying information. We measured total area and area of absolute dense tissue (ADA) of mammogram directly. Using these information, we calculated non-dense area (NDA) and percent dense area (PDA). Cumulus has been shown to be highly reliable [26]. Intra-class correlation coefficients for total area, dense area, non-dense area, and percent dense area in our Healthy Twin study were estimated to be 0.99, 0.98, 0.97, and 0.98, respectively.
Venous blood samples were obtained from participants between 8 and 10 AM after overnight fast followed by immediate separation of sera through centrifugation. Sera samples were then frozen at below − 70 °C. Total testosterone, total estradiol, and sex hormone-binding globulin (SHBG) levels were immediately measured after thawing the frozen sera in a central laboratory with chemiluminescence immunoassay using ADVIA Centaur XP Kits (Siemens, Erlange, Germany) and an electrochemiluminescence immunoassay using Cobas e602 (Roche Diagnostics, Basel, Switzerland), respectively. Detection lower limits of the assay were 1.0 ng/dL for total testosterone and 5.0 pg/mL for total estradiol. Upper limit for measuring SHBG was 200 nmol/L. When we needed to do a calculation using the level of each sex hormone, we set the undetectably low estradiol concentration (< 5.0 pg/mL) as 4.99 pg/mL, the undetectably low testosterone concentration (< 1.0 ng/dL) as 0.9 ng/dL, and unmeasurably high SHBG concentration (> 200 nmol/L) as 201 nmol/L.
Intra-assay coefficients of variation and inter-assay coefficients of variation were < 6.2% and < 4.7% for total testosterone, < 6.7 and 10.6% for estradiol, and < 1.7% and < 4.0% for SHBG, respectively. We calculated free testosterone (cFT) from the measured levels of total testosterone and SHBG, using calculation method that was reported to have higher validity than measured value by dialysis-based methods [27, 28].
We measured body weight (kg) and height (cm) using a digital scale and a stadiometer for the subject in light clothing without wearing shoes. BMI was calculated as weight divided by height squared (kg/m2). We obtained information on menstrual and reproductive history (age at menarche, age at the first childbirth, number of live children, and duration of breast feeding) using a self-administered questionnaire.
All participants provided a written informed consent form. The study protocol was approved by the Institutional Review Board of the participating center (approval number: SMC 2005-08-113).
Statistical Analysis
To see the relation between age-adjusted levels of MD measures and the levels of circulating sex hormones, we categorized study participants into four groups based on quartile distribution of total testosterone, cFT, and SHBG. For estradiol, three groups were applied: subjects with estradiol concentration below the lowest detectable level were assigned into one group (287 women) and remaining subjects were dichotomized by the median level of estradiol as a cutoff point. Age-adjusted least squares means of mammographic measures were then calculated for each sex hormone group. The presence of trends in the distribution of mammographic measures according to levels of sex hormones was tested by age-adjusted linear regression analysis.
We evaluated associations between each sex hormone and each mammographic density measure using mixed linear model. We estimated percent difference of each MD measure for each 1 standard deviation (SD) increase of testosterone, cFT, and SHBG. For this analysis, subjects with undetectably low level of testosterone (16 women) or unmeasurably high SHBG (2 women) were excluded, as needed. We estimated percent difference of each MD measure for women with detectible level of estradiol as compared to those with undetectable level of estradiol. Prior to this analysis, each MD measure was log transformed because their distribution did not fulfill normality assumption. Correlation structures from family relationships were adjusted by considering family (as family number) as a random effect in the mixed linear model. At first, we performed age-adjusted analysis. Then we repeated the analysis in two models with different steps of covariates adjustment. Reproductive and menstrual factors such as age at menarche, age at the first full-term childbirth, number of live children, and duration of breast feeding were inputted to the model as fixed effects based on previously reported probable associations of those factors with sex hormones and MD [6, 7]. To minimize reduction of study power, we imputed missing values for the number of child using mean values obtained from women with the same age and assigned a separate category for missing values for age at menarche, age at first childbirth, and duration of breast feeding.
BMI is closely correlated with mammographic measures [29] and circulating sex hormones (Supplementary Table 1). Thus, we examined the influence of BMI on the association between sex hormones and MD by inputting BMI to the final model.
We also examined the presence of interaction between BMI and circulating sex hormones by repeating the mixed linear analysis in two BMI subgroups after adjusting for covariates (Supplementary Table 1). The presence of statistically significant interaction between BMI and sex hormones was examined by putting an interaction term (BMI group × sex hormone level) in the model.
Results
Table 1 shows characteristics of study subjects. Their mean age was 60.3 years (standard deviation (SD) 7.19; range 39–79 years). Mean PDA was 14.28% (SD 13.54). Mean (SD) levels of circulating hormones were 6.31 (3.48) pg/mL for estradiol, 37.34 (30.78) ng/dL for total testosterone, 0.439 (0.538) ng/dL for cFT, and 75.44 (35.78) nmol/L for SHBG.
Table 2 shows age-adjusted mean levels of MD measures according to levels of circulating sex hormones. Levels of all MD measures did not significantly differ by estradiol levels. With increasing levels of total testosterone, and cFT, non-dense area among MD measures tended to increase whereas ADA and PDA tended to decrease. On the other hand, with increasing SHBG levels, non-dense mammographic area was decreased while ADA and PDA were increased gradually.
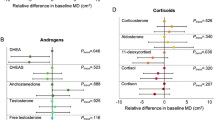
Percent differences of MD measures associated with one-standard deviation increase of each circulating sex hormone are presented in Table 3. Estradiol level was not associated with any MD measures. Testosterone was positively associated with non-dense area. However, this association did not persist in fully adjusted analysis. The cFT was associated with non-dense area. This association persisted even after BMI adjustment, with non-dense area increased by 3.5% per 1 SD increase of cFT. SHBG showed an inverse association with non-dense area but a positive association with ADA and PDA in age and reproductive factor adjusted models. When we additionally made an adjustment for BMI, associations of SHBG with non-dense area and PDA remained significant, with non-dense area decreased by 5.6% and PDA increased by 13.4% per 1 SD increase of SHBG.
Discussions
In this cross-sectional study on postmenopausal Korean women, we found that SHBG had a significant association with MD after adjusting for BMI and reproductive factors. Women with higher SHBG levels showed higher PDA of mammogram. This might be due to the positive association between SHBG and ADA and an inverse association between SHBG and non-dense area. Among sex hormones, testosterone and cFT had borderline positive and positive association with NDA, respectively, after adjusting for covariates including BMI.
It has been suggested that testosterone can stimulate epithelial proliferation of mammary gland in animal and experimental studies [30, 31]. It plays an unfavorable role in MD change and breast cancer development. On the other hand, anti-proliferative, pro-apoptotic, and inhibitory effects of testosterone on breast cancer cell growth via its action on androgen receptor have also been suggested [32, 33]. In accordance with pro-proliferative effect of testosterone, Jung et al. [34] have reported that testosterone has a positive association with percentage of dense breast volume measured by magnetic resonance imaging after adjusting for BMI and other covariates in young women, although free testosterone is not associated with breast density. However, studies that support the anti-proliferative effect of testosterone in human breast are more abundant. An inverse association between testosterone and PDA has been frequently observed in other population based studies [12, 15, 17, 21, 23], although most studies with an adjustment for BMI have reported that testosterone or cFT is not associated with MD in either premenopausal [11,12,13] or postmenopausal women [14, 15, 18, 21]. Studies have also consistently shown a null association of total or cfT with ADA or PDA regardless of BMI adjustment [21, 22], as found in the present study.
The association of NDA reflecting lobular involution with testosterone and cFT also seems somewhat controversial. In our study, testosterone was positively associated with NDA after adjusting for age and reproductive factors. However, this association was markedly attenuated to borderline significant level after additional adjustment for BMI. Similar finding has been repeatedly found in other studies [12, 15, 17]. On the other hand, we found a positive association between cFT and NDA that was slightly attenuated but persisted even after adjusting for BMI. This is an unexpected finding because many previous studies showed no significant association between cFT and NDA after adjusting for BMI [14, 15, 34] or even before adjusting for BMI [22]. One study has shown persistent positive association between testosterone and NDA regardless of BMI adjustment [23]. Although inconsistency exists between studies, these findings seem to be in favor of an anti-proliferative effect of testosterone on breast tissue, thus having a protective role against breast cancer.
Animal and in vivo studies have suggested that estrogen has proliferative and growth-promoting effects on epithelial cells of breast [35, 36]. Increase in MD after exogenous hormone use in postmenopausal women supports results of non-human studies [37, 38], suggesting that estrogen increases the risk of breast cancer development by increasing breast density. However, the relationship between MD and estrogen has been inconsistent even among studies limited to postmenopausal women. Only a few studies have reported a positive association between estradiol and MD [16, 21]. After adjusting for covariates in postmenopausal women, no association [11, 18, 19, 22] or inverse association between estrogen and MD was more frequently found [9, 20]. There are several explanations for such inconsistent association between estradiol and MD. First, given the main source of estrogen secretion, menopausal status of study participants might have caused various findings. However, the inconsistency in the observed relation of estradiol and free estradiol with MD has been seen in premenopausal women [9, 11, 13] and postmenopausal women between studies [16, 18, 21]. Second, exogenous hormones may generate a steroidal environment that affects MD differently than endogenous hormones [20]. To examine this hypothesis, Verheus et al. [15] have performed stratified analyses by ever-use of HRT. In their study, they found that estrogen level was significantly inversely related to both percentage breast density and dense area in subgroup of HRT ever-users, but not in the subgroup of HRT never-users. Estrogen metabolism might differ by previous use of HRT. This may in part explain different associations with MD between former users (inverse) and never users (null). Third, very low level of estradiol in postmenopausal women may not exert detectable effect on MD while body fat may act as a more important predictor of MD than estrogen levels in postmenopausal women [20]. In several studies on postmenopausal women [15, 18, 19, 22], the inverse association of estradiol and free estradiol with MD disappeared after adjusting for BMI, suggesting a confounding role of BMI. Interestingly, some studies have reported a positive association between estradiol and MD after adjusting for BMI [16, 21]. These findings support the role of BMI as an important confounder to be considered in studies on the association between MD and estradiol. Fourth, although we did not examine the association between progesterone and MD, some studies showed a positive association between progesterone and MD [39, 40] which might explain the positive association between HRT and MD.
SHBG binds to testosterone and estradiol, and thus, bioavailability of these sex hormones is influenced by the level of SHBG. Although SHBG is associated with breast cancer risk through its inhibitory role in steroid signaling pathway by sequestering bioavailable estradiol and testosterone, SHBG may have independent effect on its own [41]. SHBG can exert an independent role by mediating steroid signaling through SHBG receptor [42]. Although mechanism has not been defined yet, studies on patients with polycystic ovary syndrome who tend to have lower risk of developing breast cancer have commonly found a low SHBG level [43, 44]. This also supports the independent effect of SHBG. The present study found a positive association between SHBG and PDA and an inverse association between SHBG and non-dense area regardless of adjustment for BMI. We repeated this analysis in subgroups stratified by BMI level (< 25, ≥ 25) and found no modifying effect of BMI on the association between SHBG and MD (Supplementary Table 2). There have been several previous studies showing a significant positive association between SHBG and MD [11, 13,14,15, 18, 21, 22, 45, 46], although some other studies have found no association in premenopausal [9, 10, 12] or postmenopausal women [15,16,17,18,19,20, 22]. The direction of association between SHBG and MD which is opposite to the inverse association between SHBG and breast cancer supports SHBG-receptor-mediating effect of SHBG.
BMI was reported to be positively correlated with levels of total estradiol and free testosterone and had an inverse correlation with SHBG level, although it had no correlation with total testosterone [18]. Although there was a slight inconsistency with the findings of previous study, we also found that BMI was correlated with sex hormones (supplementary Table 1). Given the strong association of BMI with MD, the association between each hormone and MD may be influenced by the relation between BMI and each hormone [24]. Therefore, considering BMI seems essential when examining the association between each hormone and MD. In fact, some studies have shown significant attenuation of the association after adjusting for BMI [10, 15, 19, 22]. However, the attenuation of the association between hormones and MD after adjusting for BMI is inconsistent by types of hormones and types of MD [12, 16,17,18, 21, 23, 34], as found in the present study.
The present study has some strength. To the best of our knowledge, this is the first large scale study evaluating the association between MD and sex hormones in Asian women. Large sample of postmenopausal women was recruited. We could take account of a wide range of reproductive factors and BMI that may confound the relation between hormone and MD. External hormonal effects were not involved because previous or current HRT users were excluded. We measured mammographic density quantitatively using the Cumulus technique that provided more accurate density information compared to previously used qualitative methods.
However, our study also has several limitations. First, only postmenopausal women were included. Thus, findings of this study could not be generalized to premenopausal women. The advantage of these samples was that the influence of fluctuating level of sex hormones in premenopausal women could be avoided. Second, we did not measure progesterone level. Third, we could not evaluate an association between MD and free estradiol. We could not estimate free estradiol level even using calculation method in too many subjects because of their undetectably low estradiol level. Fourth, we could not use gold standard method for measuring sex hormones such as mass spectrometry-based methods, because they are expensive and technically demanding processes. Fifth, we used single measured sex hormones level which might not reflect long-term exposure to hormones. However, a previous study has reported high intra-class correlation coefficients between sex hormone levels repeatedly measured up to 3 years apart in the same postmenopausal woman [20]. Thus, such single measurement might not incur significantly biased findings. Finally, we could not consider the effect of locally generated estradiol that is produced by aromatase in the breast and could have direct influence on the breast tissue without entering circulation.
In conclusion, SHBG had a positive association with PDA in postmenopausal Korean women who had never used HRT. Such association was independent of reproductive risk factors or BMI. This finding suggests that SHBG, not circulating sex hormone, might be related with breast cancer risk, probably through its association with breast density.
References
Boyd NF, Martin LJ, Sun L, Guo H, Chiarelli A, Hislop G, Yaffe M, Minkin S (2006) Body size, mammographic density, and breast cancer risk. Cancer Epidemiol Biomark Prev 15:2086–2092
Li T, Sun L, Miller N, Nicklee T, Woo J, Hulse-Smith L, Tsao MS, Khokha R, Martin L, Boyd N (2005) The association of measured breast tissue characteristics with mammographic density and other risk factors for breast cancer. Cancer Epidemiol Biomark Prev 14:343–349
Kim BK, Choi YH, Nguyen TL, Nam SJ, Lee JE, Hopper JL, Sung J, Song YM (2015) Mammographic density and risk of breast cancer in Korean women. Eur J Cancer Prev 24:422–429
Maskarinec G, Pagano I, Lurie G, Wilkens LR, Kolonel LN (2005) Mammographic density and breast cancer risk: the multiethnic cohort study. Am J Epidemiol 162:743–752
Vachon CM, Kuni CC, Anderson K, Anderson VE, Sellers TA (2000) Association of mammographically defined percent breast density with epidemiologic risk factors for breast cancer (United States). Cancer Causes Control 11:653–662
Hankinson SE, Colditz GA, Willett WC (2004) Towards an integrated model for breast cancer etiology: the lifelong interplay of genes, lifestyle, and hormones. Breast Cancer Res 6:213–218
Sung J, Song YM, Stone J, Lee K, Lee D (2011) Reproductive factors associated with mammographic density: a Korean co-twin control study. Breast Cancer Res Treat 128:567–572
Martin LJ, Boyd NF (2008) Mammographic density. Potential mechanisms of breast cancer risk associated with mammographic density: hypotheses based on epidemiological evidence. Breast Cancer Res 10:201
Boyd NF, Stone J, Martin LJ, Jong R, Fishell E, Yaffe M, Hammond G, Minkin S (2002) The association of breast mitogens with mammographic densities. Br J Cancer 87:876–882
Noh JJ, Maskarinec G, Pagano I, Cheung LW, Stanczyk FZ (2006) Mammographic densities and circulating hormones: a cross-sectional study in premenopausal women. Breast 15:20–28
Borugian MJ, Spinelli JJ, Gordon PB, Abanto Z, Brooks-Wilson A, Pollak MN, Warren LJ, Hislop TG, Gallagher RP (2014) Fasting insulin and endogenous hormones in relation to premenopausal breast density (Canada). Cancer Causes Control 25:385–394
Walker K, Fletcher O, Johnson N, Coupland B, McCormack VA, Folkerd E, Gibson L, Hillier SG, Holly JM, Moss S, Dowsett M, Peto J, dos Santos SI (2009) Premenopausal mammographic density in relation to cyclic variations in endogenous sex hormone levels, prolactin, and insulin-like growth factors. Cancer Res 69:6490–6499
Yong M, Atkinson C, Newton KM, Aiello Bowles EJ, Stanczyk FZ, Westerlind KC, Holt VL, Schwartz SM, Leisenring WM, Lampe JW (2009) Associations between endogenous sex hormone levels and mammographic and bone densities in premenopausal women. Cancer Causes Control 20:1039–1053
Bremnes Y, Ursin G, Bjurstam N, Rinaldi S, Kaaks R, Gram IT (2007) Endogenous sex hormones, prolactin and mammographic density in postmenopausal Norwegian women. Int J Cancer 121:2506–2511
Verheus M, Peeters PH, van Noord PA, van der Schouw YT, Grobbee DE, van Gils CH (2007) No relationship between circulating levels of sex steroids and mammographic breast density: the Prospect-EPIC cohort. Breast Cancer Res 9:R53
Johansson H, Gandini S, Bonanni B, Mariette F, Guerrieri-Gonzaga A, Serrano D, Cassano E, Ramazzotto F, Baglietto L, Sandri MT, Decensi A (2008) Relationships between circulating hormone levels, mammographic percent density and breast cancer risk factors in postmenopausal women. Breast Cancer Res Treat 108:57–67
McCormack VA, Dowsett M, Folkerd E, Johnson N, Palles C, Coupland B, Holly JM, Vinnicombe SJ, Perry NM, dos Santos SI (2009) Sex steroids, growth factors and mammographic density: a cross-sectional study of UK postmenopausal Caucasian and Afro-Caribbean women. Breast Cancer Res 11:R38
Sprague BL, Trentham-Dietz A, Gangnon RE, Buist DS, Burnside ES, Bowles EJ, Stanczyk FZ, Sisney GS (2011) Circulating sex hormones and mammographic breast density among postmenopausal women. Horm Cancer 2:62–72
Woolcott CG, Courneya KS, Boyd NF, Yaffe MJ, McTiernan A, Brant R, Jones CA, Stanczyk FZ, Terry T, Cook LS, Wang Q, Friedenreich CM (2013) Association between sex hormones, glucose homeostasis, adipokines, and inflammatory markers and mammographic density among postmenopausal women. Breast Cancer Res Treat 139:255–265
Aiello EJ, Tworoger SS, Yasui Y, Stanczyk FZ, Potter J, Ulrich CM, Irwin M, McTiernan A (2005) Associations among circulating sex hormones, insulin-like growth factor, lipids, and mammographic density in postmenopausal women. Cancer Epidemiol Biomark Prev 14:1411–1417
Greendale GA, Palla SL, Ursin G, Laughlin GA, Crandall C, Pike MC, Reboussin BA (2005) The association of endogenous sex steroids and sex steroid binding proteins with mammographic density: results from the Postmenopausal Estrogen/Progestin Interventions Mammographic Density Study. Am J Epidemiol 162:826–834
Tamimi RM, Hankinson SE, Colditz GA, Byrne C (2005) Endogenous sex hormone levels and mammographic density among postmenopausal women. Cancer Epidemiol Biomark Prev 14:2641–2647
Varghese JS, Smith PL, Folkerd E, Brown J, Leyland J, Audley T, Warren RM, Dowsett M, Easton DF, Thompson DJ (2012) The heritability of mammographic breast density and circulating sex-hormone levels: two independent breast cancer risk factors. Cancer Epidemiol Biomark Prev 21:2167–2175
Becker S, Kaaks R (2009) Exogenous and endogenous hormones, mammographic density and breast cancer risk: can mammographic density be considered an intermediate marker of risk? Recent Results Cancer Res 181:135–157
Gombojav B, Song YM, Lee K, Yang S, Kho M, Hwang YC, Ko G, Sung J (2013) The healthy twin study, Korea updates: resources for omics and genome epidemiology studies. Twin Res Hum Genet 16:241–245
Byng JW, Yaffe MJ, Jong RA, Shumak RS, Lockwood GA, Tritchler DL, Boyd NF (1998) Analysis of mammographic density and breast cancer risk from digitized mammograms. Radiographics 18:1587–1598
Vermeulen A, Verdonck L, Kaufman JM (1999) A critical evaluation of simple methods for the estimation of free testosterone in serum. J Clin Endocrinol Metab 84:3666–3672
Rinaldi S, Geay A, Dechaud H, Biessy C, Zeleniuch-Jacquotte A, Akhmedkhanov A, Shore RE, Riboli E, Toniolo P, Kaaks R (2002) Validity of free testosterone and free estradiol determinations in serum samples from postmenopausal women by theoretical calculations. Cancer Epidemiol Biomark Prev 11:1065–1071
Sung J, Song YM, Stone J, Lee K, Kim SY (2010) Association of body size measurements and mammographic density in Korean women: the Healthy Twin study. Cancer Epidemiol Biomark Prev 19:1523–1531
Sonne-Hansen K, Lykkesfeldt AE (2005) Endogenous aromatization of testosterone results in growth stimulation of the human MCF-7 breast cancer cell line. J Steroid Biochem Mol Biol 93:25–34
James VH, McNeill JM, Lai LC, Newton CJ, Ghilchik MW, Reed MJ (1987) Aromatase activity in normal breast and breast tumor tissues: in vivo and in vitro studies. Steroids 50:269–279
Eigeliene N, Elo T, Linhala M, Hurme S, Erkkola R, Harkonen P (2012) Androgens inhibit the stimulatory action of 17 beta-estradiol on normal human breast tissue in explant cultures. J Clin Endocrinol Metab 97:E1116–E1127
Hofling M, Hirschberg AL, Skoog L, Tani E, Hagerstrom T, von Schoultz B (2007) Testosterone inhibits estrogen/progestogen-induced breast cell proliferation in postmenopausal women. Menopause 14:183–190
Jung S, Stanczyk FZ, Egleston BL, Snetselaar LG, Stevens VJ, Shepherd JA, Van Horn L, LeBlanc ES, Paris K, Klifa C, Dorgan JF (2015) Endogenous sex hormones and breast density in young women. Cancer Epidemiol Biomark Prev 24:369–378
Doisneau-Sixou SF, Sergio CM, Carroll JS, Hui R, Musgrove EA, Sutherland RL (2003) Estrogen and antiestrogen regulation of cell cycle progression in breast cancer cells. Endocr Relat Cancer 10:179–186
Yager JD, Davidson NE (2006) Estrogen carcinogenesis in breast cancer. N Engl J Med 354:270–282
Greendale GA, Reboussin BA, Slone S, Wasilauskas C, Pike MC, Ursin G (2003) Postmenopausal hormone therapy and change in mammographic density. J Natl Cancer Inst 95:30–37
Rutter CM, Mandelson MT, Laya MB, Seger DJ, Taplin S (2001) Changes in breast density associated with initiation, discontinuation, and continuing use of hormone replacement therapy. JAMA 285:171–176
Chen JH, Chen WP, Chan S, Yeh DC, Su MY, McLaren CE (2013) Correlation of endogenous hormonal levels, fibroglandular tissue volume and percent density measured using 3D MRI during one menstrual cycle. Ann Oncol 24:2329–2335
Greendale GA, Reboussin BA, Sie A, Singh HR, Olson LK, Gatewood O, Bassett LW, Wasilauskas C, Bush T, Barrett-Connor E (1999) Effects of estrogen and estrogen-progestin on mammographic parenchymal density. Postmenopausal Estrogen/Progestin Interventions (PEPI) investigators. Ann Intern Med 130:262–269
Zeleniuch-Jacquotte A, Shore RE, Koenig KL, Akhmedkhanov A, Afanasyeva Y, Kato I, Kim MY, Rinaldi S, Kaaks R, Toniolo P (2004) Postmenopausal levels of oestrogen, androgen, and SHBG and breast cancer: long-term results of a prospective study. Br J Cancer 90:153–159
Kahn SM, Hryb DJ, Nakhla AM, Romas NA, Rosner W (2002) Sex hormone-binding globulin is synthesized in target cells. J Endocrinol 175:113–120
Jayagopal V, Kilpatrick ES, Jennings PE, Hepburn DA, Atkin SL (2003) The biological variation of testosterone and sex hormone-binding globulin (SHBG) in polycystic ovarian syndrome: implications for SHBG as a surrogate marker of insulin resistance. J Clin Endocrinol Metab 88:1528–1533
Gammon MD, Thompson WD (1991) Polycystic ovaries and the risk of breast cancer. Am J Epidemiol 134:818–824
Boyd N, Martin L, Chavez S, Gunasekara A, Salleh A, Melnichouk O, Yaffe M, Friedenreich C, Minkin S, Bronskill M (2009) Breast-tissue composition and other risk factors for breast cancer in young women: a cross-sectional study. Lancet Oncol 10:569–580
Warren R, Skinner J, Sala E, Denton E, Dowsett M, Folkerd E, Healey CS, Dunning A, Doody D, Ponder B, Luben RN, Day NE, Easton D (2006) Associations among mammographic density, circulating sex hormones, and polymorphisms in sex hormone metabolism genes in postmenopausal women. Cancer Epidemiol Biomark Prev 15:1502–1508
Funding
This study was supported by a grant from the National R&D Program for Cancer Control, Ministry of Health & Welfare, Republic of Korea (1720270).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
All participants provided a written informed consent form. The study protocol was approved by the Institutional Review Board of the participating center (approval number: SMC 2005-08-113).
Conflict of Interest
The authors declare that they have no conflict of interest.
Electronic Supplementary Material
ESM 1
(DOCX 24 kb)
Rights and permissions
About this article

Cite this article
Lee, K., Yoo, J.E., Nguyen, T.L. et al. Mammographic Density and Circulating Sex Hormones: a Cross-Sectional Study in Postmenopausal Korean Women. HORM CANC 9, 383–390 (2018). https://doi.org/10.1007/s12672-018-0344-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12672-018-0344-7