
Abstract
Background:
Complicated skin and skin structure infections (cSSSIs) are an important healthcare concern worldwide, as they can be life-threatening and challenging to treat. cSSSIs are normally managed using a combination of surgical intervention and prompt antibiotic use. New therapeutic options, including novel antibiotics, are required to improve outcomes in terms of duration of illness and to reduce the consumption of healthcare resources.
Methods:
This was a prospective, randomized, open-label, parallel-group, multinational clinical study comparing sequential intravenous/oral (iv/po) moxifloxacin, 400 mg once daily, and iv amoxicillin/clavulanate, 1,000 mg/ 200 mg three times daily followed by po amoxicillin/ clavulanate, 500 mg/125 mg three times daily, for 7–21 days in hospitalized patients.
Results:
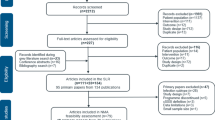
A total of 804 patients were enrolled (mean age 51.8 years). The most common clinical diagnosis was complicated erysipelas (32.1% moxifloxacin; 30.0% amoxicillin/ clavulanate) and major abscess (31.1% moxifloxacin; 29.3% amoxicillin/clavulanate). Overall clinical success rates at the test-of-cure (TOC) visit (14–28 days post-treatment) for the per-protocol population (primary efficacy variable) were 80.6% (254/315) for patients in the moxifloxacin group and 84.5% (268/317) for those receiving amoxicillin/clavulanate (95% confidence interval [CI] –9.41, 2.18). Similar results were obtained for the intention-to-treat population (95% CI –7.56, 4.31). In both treatment groups, the highest clinical success rates were recorded for patients with complicated erysipelas, major abscess, surgical wound infection, and cellulitis. The lowest clinical cure rates were reported for diabetic foot infection and necrotizing fasciitis. In the microbiologically evaluable population, the bacteriological success rate (eradication and presumed eradication) was 76.0% (127/ 167) in the moxifloxacin group and 81.4% (140/172) in the amoxicillin/clavulanate group (95% CI –12.96, 4.41). Staphylococcus aureus (137 isolates) and Escherichia coli (50 isolates) were the most frequently isolated skin pathogens. Adverse event rates were comparable between treatment groups.
Conclusions:
Treatment with sequential iv/po moxifloxacin monotherapy once daily is clinically comparable to that with iv/po amoxicillin/clavulanate three times daily in the management of cSSSIs. Moxifloxacin’s simple dose regimen offers an advantage over amoxicillin/clavulanate and represents a valuable addition to current antibiotic regimens used in the treatment of cSSSIs.
Similar content being viewed by others

References
Di Nubile MJ, Lipsky BA: Complicated infections of skin and skin structures: when the infection is more than skin deep. J Antimicrob Chemother 2004; 53: 37–50.
Fung HB, Chang JY, Kuczynski S: A practical guide to the treatment of complicated skin and soft tissue infections. Drugs 2003; 63: 1459–1480.
Nichols RL: Optimal treatment of complicated skin and skin structure infections. J Antimicrob Chemother 1999; 44(Suppl A): 19–23.
Lipsky BA, Weigelt JA, Gupta V, Killian A, Peng MM: Skin, soft tissue, bone, and joint infections in hospitalized patients: epidemiology and microbiological, clinical, and economic outcomes. J Antimicrob Chemother 2007; 60: 370–376.
Giordano P, Weber K, Gesin G, Kubert J: Skin and skin structure infections: treatment with newer generation fluoroquinolones. Ther Clin Risk Manage 2007; 3: 1–9.
Bayer HealthCare and Schering-Plough: Avelox iv US Prescribing Information. Bayer HealthCare and Schering-Plough: Wuppertal, 2007.
Lipsky BA, Giordano P, Choudhri S, Song J: Treating diabetic foot infections with sequential intravenous to oral moxifloxacin compared with piperacillin-tazobactam/amoxicillin-clavulanate. J Antimicrob Chemother 2007; 60: 370–376.
Müller M, Stass H, Brunner M, Möller JG, Lackner E, Eichler HG: Penetration of moxifloxacin into peripheral compartments in humans. Antimicrob Agents Chemother 1999; 43: 2345–2349.
Joukhadar C, Stass H, Müller-Zellenberg U, Lackner E, Kovar F, Minar E, Müller M: Penetration of moxifloxacin into healthy and inflamed subcutaneous adipose tissues in humans. Antimicrob Agents Chemother 2003; 47: 3099–3103.
Majcher-Peszynska J, Karrasch K, Saß M, Mundkowski R, Gussmann A, Lübbert C, Kujath P, Ruf B, Schareck W, Koch H, Drewelow B: Tissue penetration and pharmacokinetics of moxifloxacin in diabetic foot infections - an interim analysis. ECCMID 2006, Poster P1516.
Ball P, Stahlmann R, Kublin R, Choudhri S, Owens R: Safety profile of oral and intravenous moxifloxacin: cumulative data from clinical trials and postmarketing studies. Clin Ther 2004; 26: 940–950.
Stass H, Kubitza D: Pharmacokinetics and elimination of moxifloxacin after oral and intravenous administration in man. J Antimicrob Chemother 1999; 43(Suppl B): 83–90.
Wise R, Andrews JM, Marshall G, Hartman G: Pharmacokinetics and inflammatory-fluid penetration of moxifloxacin following oral or intravenous administration. Antimicrob Agents Chemother 1999; 43: 1508–1510.
Wilson SE, Solomkin JS, Le V, Cammarata SK, Bruss JB: A severity score for complicated skin and soft tissue infections derived from Phase III studies of linezolid. Am J Surg 2003; 185: 369–375.
Wagner FW Jr: The diabetic foot. Orthopedics 1987; 10: 163–172.
Giordano P, Song J, Pertel P, Herrington J, Kowalsky S: Sequential intravenous/oral moxifloxacin versus intravenous piperacillin-tazobactam followed by oral amoxicillin-clavulanate for the treatment of complicated skin and skin structure infection. Int J Antimicrob Agents 2005; 26: 357–365.
Lipsky BA: Medical treatment of diabetic foot infections. Clin Infect Dis 2004; 39(Suppl 1): S104–S114.
Lipsky BA, Berendt AR, Deery HG, Embil JM, Joseph WS, Karchmer AW, LeFrock JL, Lew DP, Mader JT, Norden C, Tan JS: Diagnosis and treatment of diabetic foot infections. Clin Infect Dis 2004; 39: 885–910.
Author information
Authors and Affiliations
Consortia
Corresponding author
Rights and permissions
About this article
Cite this article
Vick-Fragoso, R., Hernández-Oliva, G., Cruz-Alcázar, J. et al. Efficacy and safety of sequential intravenous/oral moxifloxacin vs intravenous/oral amoxicillin/clavulanate for complicated skin and skin structure infections. Infection 37, 407–417 (2009). https://doi.org/10.1007/s15010-009-8468-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s15010-009-8468-x