
Abstract
Purpose
Malignant external otitis is an aggressive and potentially life-threatening infection. This rare disorder is typically caused by Pseudomonas aeruginosa and affects almost exclusively elderly diabetic patients. However, fungal malignant external otitis have been identified, especially in immunocompromised hosts.
Methods
We report a rare case of invasive malignant external otitis caused by Aspergillus flavus in a diabetic patient without other underlying immunosuppression. A review of Aspergillus spp. malignant external otitis since voriconazole became the first line for invasive aspergillosis was performed.
Results
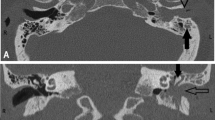
A 72-year-old man with diabetes mellitus developed invasive malignant external otitis with a vascular involvement. The patient was treated with empiric courses of antibiotics until a fungal infection was diagnosed. Proven Apsergillus infection was based on histopathological examination and isolation of A. flavus from culture of osteo-meningeal biopsies. Despite optimal antimicrobial therapy with voriconazole, the patient presented with cerebral infarction in the setting of an angioinvasive fungal infection leading to a fatal outcome. From a review of the literature, we found 39 previously published cases of proven Aspergillus spp. malignant external otitis treated with new triazoles.
Conclusion
Given our experience and the literature review, a fungal etiology should be considered early in the course of malignant external otitis unresponsive to a conventional broad spectrum antibiotic therapy, with the need for a tissue biopsy to confirm the diagnosis.




Similar content being viewed by others


References
Chandler JR. Malignant external otitis. Laryngoscope. 1968;78:1257–94.
Hedayati MT, Pasqualotto AC, Warn PA, Bowyer P, Denning DW. Aspergillus flavus: human pathogen, allergen and mycotoxin producer. Microbiology. 2007;153:1677–92.
Marzo SJ, Leonetti JP. Invasive fungal and bacterial infections of the temporal bone. Laryngoscope. 2003;113:1503–7.
Amonoo-Kuofi K, Tostevin P, Knight JR. Aspergillus mastoiditis in a patient with systemic lupus erythematosus: a case report. Skull Base. 2005;15:109–12.
Ling SS, Sader C. Fungal malignant otitis externa treated with hyperbaric oxygen. Int J Infect Dis. 2008;12:550–2.
van Tol A, van Rijswijk J. Aspergillus mastoiditis, presenting with unexplained progressive otalgia, in an immunocompetent (older) patient. Eur Arch Otorhinolaryngol. 2009;266:1655–7.
Parize P, Chandesris MO, Lanternier F, et al. Antifungal therapy of Aspergillus invasive otitis externa: efficacy of voriconazole and review. Antimicrob Agents Chemother. 2009;53:1048–53.
Soudry E, Hamzany Y, Preis M, et al. Malignant external otitis: analysis of severe cases. Otolaryngol Head Neck Surg. 2011;144:758–62.
Bovo R, Benatti A, Ciorba A, et al. Pseudomonas and Aspergillus interaction in malignant external otitis: risk of treatment failure. Acta Otorhinolaringol Ital. 2012;32:416–9.
Tarazi AE, Al-Tawfiq A, Abdi RF. Fungal malignant otitis externa: pitfalls, diagnosis, and treatment. Otol Neurotol. 2012;33:769–73.
Bhatt YM, Pahade N, Nair B. Aspergillus petrous apicitis associated with cerebral and peritubular abscesses in an immunocompetent man. J Laryngol Otol. 2013;127:404–7.
Walton J, Coulson C. Fungal malignant otitis externa with facial nerve palsy: tissue biopsy aids diagnosis. Case Rep Otolaryngol. 2014;2014:192318.
Ho HC, Hsiao SH, Lee CY, Tsai CC. Treatment of refractory Aspergillus otomycosis with voriconazole: case series and review. J Laryngol Otol. 2014;128:547–51.
Morgand M, Rammaert B, Poirée S, et al. Chronic invasive Aspergillus sinusitis and otitis with meningeal extension successfully treated with voriconazole. Antimicrob Agents Chemother. 2015;59:7857–61.
Marchionni E, Parize P, Lefevre A, et al. Aspergillus spp. invasive external otitis: favourable outcome with a medical approach. Clin Microbiol Infect 2016;22:434–7.
Lortholary O, Gangneux JP, Sitbon K, et al. Epidemiological trends in invasive aspergillosis in France: the SAIF network (2005–2007). Clin Microbiol Infect. 2011;17:1882–9.
Hot A, Maunoury C, Poiree S, et al. Diagnostic contribution of positron emission tomography with [18F]fluorodeoxyglucose for invasive fungal infections. Clin Microbiol Infect. 2011;17:409–17.
Balajee SA, Borman AM, Brandt ME, et al. Sequence-based identification of Aspergillus, Fusarium and Mucorales species in the clinical mycology laboratory: where are we and where should we go from here ? J Clin Microbiol. 2009;47:877–84.
Samson RA, Hong SB, Peterson SW, Frisvad JC, Varga J. Polyphasic taxonomy of Aspergillus section Fumigati and its teleomorph Neosartorya. Stud Mycol. 2007;59:1–47.
Pasqualotto AC. Differences in pathogenicity and clinical syndromes due to Aspergillus fumigatus and Aspergillus flavus. Med Mycol 2009;47:S261–70.
Delsing CE, Becker KL, Simon A, et al. Th17 cytokine deficiency in patients with Aspergillus skull base osteomyelitis. BMC Infect Dis. 2015;15:140.
Walsh TJ, Anaissie EJ, Denning DW, et al. Treatment of aspergillosis: clinical practice guidelines of the Infectious Diseases Society of America. Clin Infect Dis. 2008;46:327–60.
Herbrecht R, Denning DW, Patterson TF, et al. Voriconazole versus amphotericin B for primary therapy of invasive aspergillosis. N Eng J Med. 2002;347:408–15.
Chen D, Lalwani AK, House JW, Choo D. Aspergillus mastoiditis in acquired immunodeficiency syndrome. Am J Otol. 1999;20:561–7.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Authors declare that there is no conflict of interest.
Rights and permissions
About this article

Cite this article
Pichon, M., Joly, V., Argy, N. et al. Aspergillus flavus malignant external otitis in a diabetic patient: case report and literature review. Infection 48, 193–203 (2020). https://doi.org/10.1007/s15010-020-01394-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s15010-020-01394-8