
Abstract
Purpose
Patients with type 2 diabetes (T2D) have demonstrated a higher risk for developing more severe cases of COVID-19, but the complex genetic mechanism between them is still unknown. The aim of the present study was to untangle this relationship using genetically based approaches.
Methods
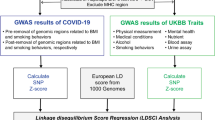
By leveraging large-scale genome-wide association study (GWAS) summary statistics of T2D and COVID-19 severity, linkage disequilibrium score regression and Mendelian randomization (MR) analyses were utilized to quantify the genetic correlations and causal relationships between the two traits. Gene-based association and enrichment analysis were further applied to identify putative functional pathways shared between T2D and COVID-19 severity.
Results
Significant, moderate genetic correlations were detected between T2D and COVID-19 hospitalization (rg = 0.156, SE = 0.057, p = 0.005) or severe disease (rg = 0.155, SE = 0.057, p = 0.006). MR analysis did not support evidence for a causal effect of T2D on COVID-19 hospitalization (OR 1.030, 95% CI 0.979, 1.084, p = 0.259) or severe disease (OR 0.999, 95% CI 0.934, 1.069, p = 0.982). Genes having pgene < 0.05 for both T2D and COVID-19 severe were significantly enriched for biological pathways, such as response to type I interferon, glutathione derivative metabolic process and glutathione derivative biosynthetic process.
Conclusions
Our findings further confirm the comorbidity of T2D and COVID-19 severity, but a non-causal impact of T2D on severe COVID-19. Shared genetically modulated molecular mechanisms underlying the co-occurrence of the two disorders are crucial for identifying therapeutic targets.
Similar content being viewed by others

Introduction
As of 14 April 2022, SARS-CoV-2 infection has killed over 6.1 million of individuals and has posed a serious threat to public health worldwide [1, 2]. There is high heterogeneity in clinical severity of SARS-CoV-2 infection, ranging from asymptomatic to fatal [3]. Solid evidence from epidemiological studies reported that type 2 diabetes (T2D) is strongly associated with COVID-19 adverse outcomes [4,5,6,7,8,9,10]. But whether the occurrence of T2D and severe COVID-19 is coincidence or causally associated has not been determined due to the limited number of cases and follow-up time, and whether this association is attributed to the correlation between T2D and other comorbidities remains unclear.
Therefore, a better understanding of the pathogenic mechanism underlying the co-occurrence of T2D and COVID-19 severity is warranted, which may help to allocate proper medical resource, make vaccination decisions for patients with T2D as well as develop effective therapeutic strategies for severe COVID-19. Recently, shared genetic architecture can provide insight into the biological basis of the comorbidity phenomenon. For example, Fadista et al. observed shared genetic overlap between idiopathic pulmonary fibrosis and severe COVID-19 [11]. A recent study detected strong genetic correlations between gastro-esophageal reflux disease and COVID-19 severity [12]. Both T2D and severe COVID-19 are moderately heritable, with estimates from the literature ranging from approximately 18.0% for T2D [13] and 6.5% for severe COVID-19 [14], respectively. Moreover, co-shared genetic etiology between T2D and numerous psychiatric disorders characterized by both internalizing and externalizing symptomatology that also shared molecular genetics with COVID-19 outcomes [15, 16]. Therefore, we speculated that genetic determinants contribute to the comorbidity of T2D with severe COVID-19.
To fill this urgent gap, we utilized large-scale genome-wide association study (GWAS) datasets to appraise genetic correlations, potential causality, and shared genetic components between T2D and COVID-19 severity.
Methods
Data source
The dataset of T2D was obtained from the most recent meta-analysis of T2D conducted by Mahajan et al. based on 32 European-descent GWASes, reaching 898,130 individuals [13]. Meanwhile, the T2D-unadjusted for BMI and T2D-adjusted for BMI datasets are subsets of the GWASes meta-analysis of T2D conducted by Mahajan et al. [13]. As obesity is an established risk factor for both T2D and severe COVID-19, we selected the BMI-adjusted T2D-association data for analysis in the current study. Summary genetic association estimates for COVID-19 severity (hospitalization and severe disease) were extracted from largest GWAS meta-analysis of COVID-19 to data, by the COVID-19 Host Genetics Initiative (HGI, round 5, shared publicly on 18 January 2021) [17]. The hospitalized outcome compared 9986 hospitalized COVID-19 patients (vs. 1,877,672 general population). The severe disease outcome compared 5101 confirmed as "very severe respiratory" cases (vs. 1,383,241 general population). The details of these GWASes were elaborated in Supplementary Table 1 and further information is provided elsewhere [13, 17, 18]. To minimize the potential bias due to ethnic heterogeneity, participants included in the above summary statistics were restricted to European ancestry only. Since all analyses were based on publicly available data, no ethical approval was required for present study.
Linkage disequilibrium score regression (LDSC) of cross-trait genetic correlation
We applied LDSC to estimate single nucleotide polymorphism (SNP)-based heritability (h2) of T2D and COVID-19 severity (including hospitalization and severe disease) as well as their genetic correlation (rg) [19, 20]. Briefly, LDSC carried out a weighted linear model by regressing the cross products of z statistics for two phenotypes on the LD scores across all available genetic variants. We used the pre-computed LD scores of European samples from the 1000 Genomes Project provided in the website of this software (http://github.com/bulik/ldsc). The regression slope provides an estimation of genetic correlation between T2D and COVID-19 severity.
Assessing the causality of T2D with COVID-19 severity
Selection of genetic instruments
Independent T2D-related SNPs (p < 5 × 10–8) were initially selected as the instrumental variables (IVs) for MR analyses. Where an initial genetic instrument was not present in the outcome GWAS datasets (here, COVID-19 hospitalization and severe disease), it can be replaced by a suitable proxy variant that were in high LD with the initial variant (r2 > 0.6). Furthermore, we computed R2 of each T2D-related SNP and calculated the F statistic with the following formula: F statistic = R2 × (SampleSize − 2)/(1 − R2) [21, 22]. A threshold of F statistic over 10 indicated lower risk of weak instrument bias [22].
Mendelian randomization analyses
To investigate causality of T2D with COVID-19 severity, two-sample MR analyses were employed across four different MR methods: inverse-variance weighted (IVW) [23, 24], weighted-median [25], weighted mode [26] and MR Egger [27] methods. To ensure the robustness of results, Cochran Q test and MR-Egger intercept test were used to examine heterogeneity and directional horizontal pleiotropy, respectively. Leave-one-out analysis and MR-Pleiotropy Residual Sum and Outlier (MR-PRESSO) were used to identify outlier IVs reflecting pleiotropic bias [28]. We further applied the PhenoScanner v2 [29] to check whether any of the selected IVs for T2D were associated (p < 1 × 10–5) with other phenotypes at risk of affecting COVID-19 severity, restricting to obesity and vascular or heart problems diagnosed by doctor: high blood pressure.
All MR analyses were carried out using the R packages ''TwoSampleMR'', ''MendelianRandomization'' and ''MR-PRESSO'' [30, 31]. A p value less than 0.05 was considered as statistically significant.
Gene-based association and enrichment analysis
Gene-based association analysis was conducted using Multi-marker Analysis of Genomic Annotation (MAGMA) based on SNP-wise mean model [30]. SNPs were assigned to a gene if they located within the gene body or mapped within the 20 kb upstream or downstream region. The Phase 3 of 1000 Genomes European population was used for reference panel to calculate the LD information. The maximum and minimum numbers of permutations were set to ten thousand and ten for per gene, respectively. The gene-based p value was calculated based on asymptotic sampling distribution. Potentially pleiotropic genes that were significantly associated with both T2D and COVID-19 severity with p values less than 0.05 were identified for the subsequent gene set enrichment analysis. The Gene Ontology (GO) enrichment analysis was carried out using the "clusterProfiler" package with the ontology term "BP" for biological process [31]. p values were adjusted for multiple comparisons using the Benjamini–Hochberg method.
Results
Genetic correlation of T2D with COVID-19 severity
The SNP-based heritability was estimated to 17.53% (SE = 0.013) for T2D, 0.20% (SE = 0.0005) for COVID-19 hospitalization, and 0.35% (SE = 0.0007) for COVID-19 severe. Significant positive genetic correlations between T2D and COVID-19 hospitalization (rg = 0.156, SE = 0.057, p = 0.005) or severe COVID-19 (rg = 0.155, SE = 0.057, p = 0.006) were detected with the LDSC software.
Causal relationship assessment between T2D and COVID-19 severity
A total of 191 independent SNPs were included as IVs for T2D, the F-statistic values for each SNP was above the threshold 10 (ranging from 28 to 1280, with means of 70) (Supplementary Table 2). Genetically predicted T2D was not associated with COVID-19 hospitalization or severe disease across four MR approaches (Table 1). Furthermore, the testing of Cochran’s Q test suggested evidence of heterogeneity, and MR-PRESSO detected horizontal pleiotropy outliers across estimates of included SNPs for COVID-19 hospitalization (Supplementary Table 3 and Fig. 1). After removing the outliers, no heterogeneity for T2D remained and consistent null causal association was observed (all p > 0.05). In addition, leave-one-out analysis did not detect any leverage points with significant influence (Supplementary Fig. 2). We further utilized the PhenoScanner tool to check if the SNPs used in this MR study were associated with any other phenotypes. Eighteen SNPs were associated with at least one of obesity and high blood pressure as shown in Supplementary Table 4. After removing these SNPs, non-causal effect estimation remained for COVID-19 hospitalization and severe disease (all p > 0.05) (Table 1).

Scatter plots for effect sizes of SNPs for T2D and those for COVID-19 hospitalization and severe disease. The x-axis represents the effect size of SNPs on T2D; the y-axis represents the effect size of SNPs on COVID-19 hospitalization (A) and severity (B). Colors of fitted line represents for four MR approaches. T2D type 2 diabetes, SNPs single nucleotide polymorphisms, MR Mendelian randomization
Gene-based analysis and functional enrichment analyses
MAGMA gene-based association analysis identified 9 005, 1 438 and 1 393 genes nominally significant (pgene < 0.05) in the T2D, COVID-19 hospitalization, and severe disease GWAS level association results, respectively. Then, by leveraging gene-based test outputs, we looked for overlapping genes between T2D and COVID-19 hospitalization, and severe disease, and revealed a total of 770 and 784 significantly enriched genes shared by the two disorders at pgene < 0.05, respectively. Further GO enrichment analysis identified 58, 16 enriched biological pathways between T2D and COVID-19 hospitalization, severe disease at pFDR less than 0.2, respectively, including response to type I interferon (GO:0034340), glutathione derivative metabolic process (GO:1901685), glutathione derivative biosynthetic process (GO:1901687), regulation of ATPase activity (GO:0043462), natural killer cell activation involved in immune response (GO:0002323), interleukin-7-mediated signaling pathway (GO: 0038111), etc. (Supplementary Tables 5–6).
Discussion
By leveraging the genetic correlation estimation, MR analysis, gene-based association and enrichment analyses, our results provided insights into the relationship between T2D and severe COVID-19.
We detected positive genetic correlations and further identified shared molecular mechanisms between T2D and severe COVID-19. Some of the molecular mechanisms that lead to T2D are also crucial in the progression of COVID-19. In agreement with this, Byun et al. utilized the summarized data from the UK Biobank observed robust positive genetic correlations between diabetes and COVID-19 severity (rg = 0.254) or hospitalization (rg = 0.309) [32]. We found that genetically predicted T2D did not increase the risk of COVID-19 severity, in keeping with earlier MR studies employing data from the previous data freeze (COVID-19 HGI, release 3 and 4, 2020) with smaller sample size for hospitalized as well as severe COVID-19 cases [33, 34]. Our current work also improves on previous MR investigations, as multiple complementary MR techniques and sensitivity analysis (MR-PRESSO and manually pruning pleiotropic variants) were performed to appraise the robustness of causal inference.
The relation between T2D and severe COVID-19 is more likely to be coincidental rather than causal, some other mechanisms of connection may account for their co-occurrence. This notion is supported by the results of our gene-set analysis, which identified common shared etiological pathways underlying T2D and COVID-19 severity such as response to type I interferon, glutathione derivative metabolic process, and glutathione derivative biosynthetic process. T2D and severe COVID-19 are hypothesized to be linked by several pathophysiological mechanisms including the role of inflammation, altered immune status, glucose homeostasis and activation of the renin–angiotensin–aldosterone system [35]. Notably, inflammation is central to the aetiology of the two traits [36]. The type I interferon (INF, INF-α and INF-β) response induce the expression of various interferon-stimulated genes (ISGs) that confer antiviral activities to host cells, but the aberrant and inappropriate activation can exacerbate inflammation [37], and this response was significantly enriched biological mechanism underpinning T2D and COVID-19 hospitalization and severe disease. Delayed but exaggerated type I INF responses, associated with hyperinflammation and contributing to severe progression of COVID-19, were observed in patients with severe COVID-19 [38]. Specifically, in early stage of infection, SARS-CoV-2 inhibits the host type I INF responses, resulting in delayed virus clearance and higher SARS-CoV-2 viral loads, which makes patients have a higher risk of developing severe disease [39]. A recent study reported that high glucose suppressed type I INF production and subsequent signaling in human peripheral blood mononuclear cells [40]. Another study also found that dendritic cells, which are the “professional” IFN producing cells, are poor producers of INF-α in human diabetes [41]. Furthermore, Bhavya et al. suggested that host microRNAs play a pivotal role in linking the diabetes and COVID-19 severity [42].
"Glutathione derivative metabolic process" and "glutathione derivative biosynthetic process" are well confirmed in the pathway of T2D and severe COVID-19 illness in present research. Glutathione (GSH), a thiol-containing tripeptide made up of L-glutamate, cysteine and glycine, exerts function against oxidative stress in most living organisms, based on its redox buffering action and abundance in the cell [43, 44]. The main cause of oxidative stress is an imbalance between creation and buildup of reactive oxygen species (ROS) [45]. Angiotensin-converting enzyme 2 (AEC2), the receptor of SARS-CoV-2, forms angiotensin (Ang) 1–7 from Ang II [46]. High Ang II concentrations and low Ang 1–7 concentrations lead to oxidative stress and, consequently, causes oxidation of the cysteine residues in the peptidase domain of receptors ACE2 as well as the receptor binding domain of proteins SARS-CoV-2 spike protein, being associated with more severe forms of COVID-19 [45]. T2D was widely considered to be associated with oxidative damage, and characterized by increased oxidized glutathione (GSSG/GSH ratio and decreased GSH content in different tissues [47]. Weaken antioxidant defense system exposed to the pathogenesis of T2D, might help to explain why patients with T2D are more likely to develop severe COVID-19 illness.
The major advantage of our current study is the efficient use of a series of genetic statistical techniques to address an important clinical association between T2D and COVID-19 severity at the molecular genetic level. However, several limitations ought to be noted. First, according to lack of the individual genetic data, we were unable to quantify the proportion of sample overlap between T2D and COVID-19 severity datasets, which may confound LDSC and MR analyses. Second, study participants included in the COVID-19 severity GWAS meta-analysis were not screened for T2D at baseline. In MR studies, the existence of exposure in the outcome dataset may have an impact on the causal estimates. However, this is a general restriction of two-sample MR analyses and is inevitable without individual-level data [48]. Third, since all analyses herein utilized summary data from Europeans and focused on severe COVID-19, the associations may not apply to other populations or patients with asymptomatic to moderate COVID-19. Lastly, genetic factors only explained a tiny fraction of T2D etiology, the causality of T2D and severe COVID-19 cannot be fully ruled out with these analyses.
In conclusion, our findings further confirm the comorbidity of T2D and COVID-19 severity, but a non-causal impact of T2D on severe COVID-19. Shared genetically modulated molecular mechanisms underlying the co-occurrence of the two disorders are crucial for identifying therapeutic targets.
Data availability statement
The publicly available datasets used in this study are included in the article/Supplementary material.
References
Wiersinga WJ, Rhodes A, Cheng AC et al (2020) Pathophysiology, transmission, diagnosis, and treatment of coronavirus disease 2019 (COVID-19): a review. JAMA 324:782–793. https://doi.org/10.1001/jama.2020.12839
Liu S, Zhi Y, Ying S (2020) COVID-19 and asthma: reflection during the pandemic. Clin Rev Allergy Immunol 59:78–88. https://doi.org/10.1007/s12016-020-08797-3
Chen Y, Klein SL, Garibaldi BT et al (2021) Aging in COVID-19: vulnerability, immunity and intervention. Ageing Res Rev 65:101205. https://doi.org/10.1016/j.arr.2020.101205
Holman N, Knighton P, Kar P et al (2020) Risk factors for COVID-19-related mortality in people with type 1 and type 2 diabetes in England: a population-based cohort study. Lancet Diabetes Endocrinol 8:823–833. https://doi.org/10.1016/S2213-8587(20)30271-0
Grasselli G, Zangrillo A, Zanella A et al (2020) Baseline characteristics and outcomes of 1591 patients infected with SARS-CoV-2 admitted to ICUs of the Lombardy region, Italy. JAMA 323:1574–1581. https://doi.org/10.1001/jama.2020.5394
Bhatraju PK, Ghassemieh BJ, Nichols M et al (2020) COVID-19 in critically ill patients in the Seattle Region-Case Series. N Engl J Med 382:2012–2022. https://doi.org/10.1056/NEJMoa2004500
Barron E, Bakhai C, Kar P et al (2020) Associations of type 1 and type 2 diabetes with COVID-19-related mortality in England: a whole-population study. Lancet Diabetes Endocrinol 8:813–822. https://doi.org/10.1016/S2213-8587(20)30272-2
Wu C, Chen X, Cai Y et al (2020) Risk factors associated with acute respiratory distress syndrome and death in patients with coronavirus disease 2019 pneumonia in Wuhan, China. JAMA Intern Med 180:934–943. https://doi.org/10.1001/jamainternmed.2020.0994
Myers LC, Parodi SM, Escobar GJ, Liu VX (2020) Characteristics of hospitalized adults with COVID-19 in an integrated health care system in California. JAMA 323:2195–2198. https://doi.org/10.1001/jama.2020.7202
Piva S, Filippini M, Turla F et al (2020) Clinical presentation and initial management critically ill patients with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection in Brescia, Italy. J Crit Care 58:29–33. https://doi.org/10.1016/j.jcrc.2020.04.004
Fadista J, Kraven LM, Karjalainen J et al (2021) Shared genetic etiology between idiopathic pulmonary fibrosis and COVID-19 severity. EBioMedicine 65:103277. https://doi.org/10.1016/j.ebiom.2021.103277
Ong JS, Gharahkhani P, Vaughan TL et al (2022) Assessing the genetic relationship between Gastro-esophageal Reflux Disease and risk of COVID-19 infection. Hum Mol Genet 31(3):471–480. https://doi.org/10.1093/hmg/ddab253
Mahajan A, Taliun D, Thurner M et al (2018) Fine-mapping type 2 diabetes loci to single-variant resolution using high-density imputation and islet-specific epigenome maps. Nat Genet 50:1505–1513. https://doi.org/10.1038/s41588-018-0241-6
Magalhães AC, Pedro N, Pereira L (2021) Genomic insights into the human susceptibility to SARS-CoV-2 infection. Acta Med Port 34:407–409. https://doi.org/10.20344/amp.16168
Postolache TT, Del Bosque-Plata L, Jabbour S et al (2019) Co-shared genetics and possible risk gene pathway partially explain the comorbidity of schizophrenia, major depressive disorder, type 2 diabetes, and metabolic syndrome. Am J Med Genet B Neuropsychiatr Genet 180:186–203. https://doi.org/10.1002/ajmg.b.32712
Yang AC, Kern F, Losada PM et al (2021) Dysregulation of brain and choroid plexus cell types in severe COVID-19. Nature 595:565–571. https://doi.org/10.1038/s41586-021-03710-0
The COVID-19 Host Genetics Initiative (2020) A global initiative to elucidate the role of host genetic factors in susceptibility and severity of the SARS-CoV-2 virus pandemic. Eur J Hum Genet 28:715–718. https://doi.org/10.1038/s41431-020-0636-6
Qiu LJ, Yin KJ, Pan GX, Ni J, Wang B (2022) Non-causal effects of asthma on COVID-19 susceptibility and severity. Front Genet 12:762697. https://doi.org/10.3389/fgene.2021.762697
Bulik-Sullivan BK, Loh PR, Finucane HK et al (2015) LD Score regression distinguishes confounding from polygenicity in genome-wide association studies. Nat Genet 47:291–295. https://doi.org/10.1038/ng.3211
Bulik-Sullivan B, Finucane HK, Anttila V et al (2015) An atlas of genetic correlations across human diseases and traits. Nat Genet 47:1236–1241. https://doi.org/10.1038/ng.3406
Gill D, Efstathiadou A, Cawood K et al (2019) Education protects against coronary heart disease and stroke independently of cognitive function: evidence from Mendelian randomization. Int J Epidemiol 48:1468–1477. https://doi.org/10.1093/ije/dyz200
Palmer TM, Lawlor DA, Harbord RM et al (2012) Using multiple genetic variants as instrumental variables for modifiable risk factors. Stat Methods Med Res 21:223–242. https://doi.org/10.1177/0962280210394459
Burgess S, Butterworth A, Thompson SG (2013) Mendelian randomization analysis with multiple genetic variants using summarized data. Genet Epidemiol 37:658–665. https://doi.org/10.1002/gepi.21758
Burgess S, Scott RA, Timpson NJ et al (2015) Using published data in Mendelian randomization: a blueprint for efficient identification of causal risk factors. Eur J Epidemiol 30(7):543–552. https://doi.org/10.1007/s10654-015-0011-z
Bowden J, Davey Smith G, Haycock PC, Burgess S (2016) Consistent estimation in Mendelian randomization with some invalid instruments using a weighted median estimator. Genet Epidemiol 40(4):304–314. https://doi.org/10.1002/gepi.21965
Hartwig FP, Davey Smith G, Bowden J (2017) Robust inference in summary data Mendelian randomization via the zero modal pleiotropy assumption. Int J Epidemiol 46:1985–1998. https://doi.org/10.1093/ije/dyx102
Bowden J, Davey Smith G, Burgess S (2015) Mendelian randomization with invalid instruments: effect estimation and bias detection through Egger regression. Int J Epidemiol 44:512–525. https://doi.org/10.1093/ije/dyv080
Verbanck M, Chen CY, Neale B, Do R (2018) Detection of widespread horizontal pleiotropy in causal relationships inferred from Mendelian randomization between complex traits and diseases. Nat Genet 50:693–698. https://doi.org/10.1038/s41588-018-0099-7
Kamat MA, Blackshaw JA, Young R et al (2019) PhenoScanner V2: an expanded tool for searching human genotype-phenotype associations. Bioinformatics 35:4851–4853. https://doi.org/10.1093/bioinformatics/btz469
de Leeuw CA, Mooij JM, Heskes T, Posthuma D (2015) MAGMA: generalized gene-set analysis of GWAS data. PLoS Comput Biol 11:e1004219. https://doi.org/10.1371/journal.pcbi.1004219
Yu G, Wang LG, Han Y, He QY (2012) clusterProfiler: an R package for comparing biological themes among gene clusters. OMICS 16(5):284–287. https://doi.org/10.1089/omi.2011.0118
Byun J, Han Y, Walsh KM et al (2022) Shared genomic architecture between COVID-19 severity and numerous clinical and physiologic parameters revealed by LD score regression analysis. Sci Rep 12:1891. https://doi.org/10.1038/s41598-022-05832-5
Qu HQ, Qu J, Glessner J, Hakonarson H (2022) Mendelian randomization study of obesity and type 2 diabetes in hospitalized COVID-19 patients. Metabolism 129:155156. https://doi.org/10.1016/j.metabol.2022.155156
Au Yeung SL, Zhao JV, Schooling CM (2021) Evaluation of glycemic traits in susceptibility to COVID-19 risk: a Mendelian randomization study. BMC Med 19:72. https://doi.org/10.1186/s12916-021-01944-3
Lim S, Bae JH, Kwon HS, Nauck MA (2021) COVID-19 and diabetes mellitus: from pathophysiology to clinical management. Nat Rev Endocrinol 17:11–30. https://doi.org/10.1038/s41574-020-00435-4
Alzaid F, Julla JB, Diedisheim M et al (2020) Monocytopenia, monocyte morphological anomalies and hyperinflammation characterise severe COVID-19 in type 2 diabetes. EMBO Mol Med 12:e13038. https://doi.org/10.15252/emmm.202013038
McFadden MJ, Sacco MT, Murphy KA et al (2021) FTO suppresses STAT3 activation and modulates proinflammatory interferon-stimulated gene expression. J Mol Biol. https://doi.org/10.1016/j.jmb.2021.167247
Kim YM, Shin EC (2021) Type I and III interferon responses in SARS-CoV-2 infection. Exp Mol Med 53:750–760. https://doi.org/10.1038/s12276-021-00592-0
Ramasamy S, Subbian S (2021) Critical Determinants of cytokine storm and type I interferon response in COVID-19 pathogenesis. Clin Microbiol Rev 34:e00299-e320. https://doi.org/10.1128/CMR.00299-20
Hu R, Xia CQ, Butfiloski E, Clare-Salzler M (2018) Effect of high glucose on cytokine production by human peripheral blood immune cells and type I interferon signaling in monocytes: Implications for the role of hyperglycemia in the diabetes inflammatory process and host defense against infection. Clin Immunol 195:139–148. https://doi.org/10.1016/j.clim.2018.06.003
Summers KL, Marleau AM, Mahon JL et al (2006) Reduced IFN-alpha secretion by blood dendritic cells in human diabetes. Clin Immunol 121:81–89. https://doi.org/10.1016/j.clim.2006.05.015
Bhavya PE, Mishra R (2022) Deciphering the link between Diabetes mellitus and SARS-CoV-2 infection through differential targeting of microRNAs in the human pancreas. J Endocrinol Invest 45:537–550. https://doi.org/10.1007/s40618-021-01693-3
Lv H, Zhen C, Liu J et al (2019) Unraveling the potential role of glutathione in multiple forms of cell death in cancer therapy. Oxid Med Cell Longev 2019:3150145. https://doi.org/10.1155/2019/3150145
Ogawa K (2005) Glutathione-associated regulation of plant growth and stress responses. Antioxid Redox Signal 7:973–981. https://doi.org/10.1089/ars.2005.7.973
Fodor A, Tiperciuc B, Login C et al (2021) Endothelial dysfunction, inflammation, and oxidative stress in COVID-19-mechanisms and therapeutic targets. Oxid Med Cell Longev 2021:8671713. https://doi.org/10.1155/2021/8671713
Yamamoto K, Takeshita H, Rakugi H (2020) ACE2, angiotensin 1–7 and skeletal muscle: review in the era of COVID-19. Clin Sci (Lond) 134:3047–3062. https://doi.org/10.1042/CS20200486
Silvagno F, Vernone A, Pescarmona GP (2020) The role of glutathione in protecting against the severe inflammatory response triggered by COVID-19. Antioxidants (Basel) 9:624. https://doi.org/10.3390/antiox9070624
Li GH, Cheung CL, Chung AK et al (2020) Evaluation of bi-directional causal association between depression and cardiovascular diseases: a Mendelian randomization study. Psychol Med 52:1765–1776. https://doi.org/10.1017/S0033291720003566
Funding
This study was funded by grants from the Natural Science Foundation of Anhui Province (1808085QH252) and Nature Science Foundation of Anhui Medical University (2020xkj011).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no competing interests to declare.
Ethical approval
Received approval from the appropriate local institutional review boards.
Informed consent
Each participating study obtained written informed consent from all participants.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Ni, J., Qiu, LJ., Yin, KJ. et al. Shared genetic architecture between type 2 diabetes and COVID-19 severity. J Endocrinol Invest 46, 501–507 (2023). https://doi.org/10.1007/s40618-022-01920-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40618-022-01920-5