



Introduction
Finding strategies to alleviate loneliness is an important aspect of ensuring the wellbeing and physical health of the population at later lifestages (Hawkley and Cacioppo, Reference Hawkley and Cacioppo2010; Steptoe et al., Reference Steptoe, Shankar, Demakakos and Wardle2013; Hawkley, Reference Hawkley and Pachana2015). Such strategies often focus on reducing the social isolation of the participants but show mixed results (Dickens et al., Reference Dickens, Richards, Greaves and Campbell2011; Saito et al., Reference Saito, Kai and Takizawa2012). These mixed results are unsurprising because loneliness is not equal to the degree of social isolation but instead the subjective feeling that one's social relations cannot fulfil one's expectations (Weiss, Reference Weiss1973; Perlman and Peplau, Reference Perlman and Peplau1981; De Jong Gierveld, Reference De Jong Gierveld1987; Cacioppo and Patrick, Reference Cacioppo and Patrick2008; Hawkley, Reference Hawkley and Pachana2015). Regardless of the degree of social isolation, loneliness is likely to arise if a person perceives either the quality or the quantity of their social relationships as deficient. Consequently, some people may lead a life where they are relatively socially isolated without feeling lonely, while others may have a rich social life but still feel lonely (Hawkley and Cacioppo, Reference Hawkley and Cacioppo2010). The key to an improved understanding of why loneliness arises seems to lie in a better understanding of what influences the perception of the quality and quantity of our social relationships (Dykstra, Reference Dykstra2009). Such an understanding may be found using a lifecourse perspective (Perlman and Peplau, Reference Perlman and Peplau1981).
Both Bowlby (Reference Bowlby1979) and Fraley (Reference Fraley2002) suggest that earlier social relationships affect later perceptions and resilience to social and general life adversities. For example, Fraley (Reference Fraley2002) found that the foundation of the sense of security in one's social relationships begins with the earliest attachment relationships in childhood and is affected by all subsequent relationships experienced thereafter. According to Nurius et al. (Reference Nurius, Green, Logan-Greene and Borja2015), adversities in early life serve as primary stressors that both set the stage for and interact with later experienced stressors in the lifecourse influencing psychological health. Thus, adverse social relationship experiences in earlier lifestages may be part of the explanation for why individuals – while experiencing similar social circumstances – differ in their levels of loneliness.
A lifecourse perspective stresses that socially patterned variations in health and mental wellbeing in later life are shaped by lifetime experiences up until that point (Kuh et al., Reference Kuh, Ben-Shlomo, Lynch, Hallqvist and Power2003; Umberson et al., Reference Umberson, Williams, Thomas, Liu and Thomeer2014). The perspective offers a framework in which to build and test theoretical models that link social adversity exposures across the lifecourse to loneliness in later life (Ben-Shlomo and Kuh, Reference Ben-Shlomo and Kuh2002). In turn, this may provide a better understanding of the longer-term implications of early life social adversity and whether such exposures in early life exert an influence on loneliness in later life.
Building upon a lifecourse approach to loneliness in later adulthood, this study posits that adverse social relationship experiences are part of lifecourse cascades that influence the propensity to feeling lonely in later life. We base our hypotheses on lifecourse models expecting both independent, interactive and cumulative effects of social relationships throughout the lifecourse on loneliness in later life.
A lifecourse perspective on adverse social relationship experiences and loneliness in later life
Adverse social relationship experiences concern stressful interpersonal incidents or circumstances that can impair a person's usual activities and important relationships and potentially have long-lasting effects on the individual (Dohrenwend, Reference Dohrenwend2006; Jonsson et al., Reference Jonsson, Sebastian, Strömsten, Hammarström and Gustafsson2016). Such effects include both social and biological chains of exposure that may render them more vulnerable to later pathology such as loneliness. This vulnerability includes increased stress sensitisation (Nurius et al., Reference Nurius, Green, Logan-Greene and Borja2015), altered cognitive responses such as less optimistic social interpretations and more negative beliefs or attitudes (Matthews et al., Reference Matthews, Gallo and Taylor2010). The few studies that have utilised a lifecourse approach indicate that social relationship adversity earlier in life is associated with loneliness later in life. Both Dykstra and de Jong Gierveld (Reference Dykstra and de Jong Gierveld2004) and Peters and Liefbroer (Reference Peters and Liefbroer1997) find that marital dissolution and widowhood are predictors of subsequent loneliness. However, the focus on partner dissolution, while important, does not consider social relationship adversities across the full range of social relationships and across the lifecourse. Studies looking into other outcomes (e.g. Savla et al., Reference Savla, Roberto, Jaramillo-Sierra, Gambrel, Karimi and Butner2013; Umberson et al., Reference Umberson, Williams, Thomas, Liu and Thomeer2014) indicate that additional earlier social relationship experiences such as child abuse and having parents with marital, mental or drinking problems provide evidence of associations with both health (Umberson et al., Reference Umberson, Williams, Thomas, Liu and Thomeer2014), social support and perceived psychological wellbeing in later life (Nurius et al., Reference Nurius, Green, Logan-Greene and Borja2015). These findings suggest that broadening the scope of social adversity experiences beyond partnership dissolution may enhance our understanding of the causal mechanisms leading to loneliness viewed from a lifecourse perspective.
Further, in line with the chains of risk lifecourse model, previous studies have shown that early social relationship adversities may launch chains of disadvantage in social relationships over the lifecourse with earlier experienced social relationship adversities heightening the risk of experiencing social relationship adversities later on (Dykstra and de Jong Gierveld, Reference Dykstra and de Jong Gierveld2004; Caspi et al., Reference Caspi, Harrington, Moffitt, Milne and Poulton2006; Katz et al., Reference Katz, Conway, Hammen, Brennan and Najman2011; Umberson et al., Reference Umberson, Williams, Thomas, Liu and Thomeer2014). Earlier adverse social adversity has been associated with how well one is able to meet social needs, develop friendships and counter social isolation (Browne and Shlosberg, Reference Browne and Shlosberg2006; Newall et al., Reference Newall, Chipperfield, Clifton, Perry, Swift and Ruthig2009; Jonsson et al., Reference Jonsson, Sebastian, Strömsten, Hammarström and Gustafsson2016; Pikhartova et al., Reference Pikhartova, Bowling and Victor2016).
Lastly, earlier experienced social relationship adversities may interact with later-life social relationship exposures, thereby either enhancing or decreasing the risk of feeling lonely (Cable, Reference Cable2014). Social isolation and social relationship quality are important predictors of loneliness (Weiss, Reference Weiss1973). However, it is possible that these two predictors may interact with previous experiences on their effect on loneliness. Social isolation and relationship quality are often highlighted as important stress buffers in the pathways from social relationships to health (Thoits, Reference Thoits2011). While evidence of interactive effects over the lifecourse on loneliness is lacking, Nurius et al. (Reference Nurius, Green, Logan-Greene and Borja2015) showed that high levels of childhood adversity can amplify the effect of early adversities while protective resources can ameliorate some of the effect on psychological wellbeing. Thus, earlier experienced social relationship adversities may affect how current social relationship quantity and quality lead to, or protect against, feeling lonely. Individuals with many experienced social adversities earlier on may react more negatively to being socially isolated because their social resilience is lower, more easily triggered (Nurius et al., Reference Nurius, Green, Logan-Greene and Borja2015) and their sensitivity and world view is more negative (Matthews et al., Reference Matthews, Gallo and Taylor2010). In contrast, a high current quality of social relationship in later life may provide emotional and behavioural resources (Thoits, Reference Thoits2011) which may ameliorate the negative effect earlier social relationship adversity has on loneliness.
Current study
We propose that social relationship adversities experienced throughout the lifecourse are independently associated with loneliness in later life regardless of current social and demographic circumstances. We expect this is due to a lower sense of emotional security and less-optimistic social interpretations in the individuals who have experienced social relationship adversities earlier in life. Further, in line with the chains of risk model, we expect an association between the number of earlier experienced social relationship adversities and experienced social adversity at later lifestages. Lastly, we expect that current quality and quantity of social relationships moderate how earlier social relationship adversity affects loneliness.
Methods
Study population
The Medical Research Council National Survey of Health and Development (NSHD) is a representative sample of 5,362 men and women born to married mothers in mainland Britain during one week in March 1946. Study members have been followed up 24 times, approximately every two years in childhood and with main adult sweeps at ages 26, 36, 43, 53, 60–64 and 68–69. In 2014–2015 study members were asked to complete a postal questionnaire and then invited to have a home visit by a research nurse. Of the 2,816 people in the target sample living in England, Scotland and Wales, information was obtained from the postal questionnaire and/or visits from 2,638 (94%) of whom 2,367 (84%) completed a postal questionnaire. In addition, a postal questionnaire was sent to 126 study members living abroad who remain in contact with the study, of whom 86 (68%) returned a questionnaire. No attempt was made to contact the remaining 2,420 study members: 957 (18%) had already died, 620 (12%) had previously withdrawn from the study, 448 (8%) had emigrated and were no longer in contact with the study, and 395 (7%) had been untraceable for more than five years (Kuh et al. Reference Kuh, Wong, Shah, Moore, Popham, Curran, Davis, Sharma, Richards, Stafford, Hardy and Cooper2016). Ethical approval was obtained from the NRES Queen Square REC (14/LO/1073) and Scotland A REC (14/SS/1009).
Outcome
Loneliness was measured by the three-item short UCLA scale (Hughes et al., Reference Hughes, Waite, Hawkley and Cacioppo2004). Participants were asked how often they feel (a) a lack of companionship, (b) left out and (c) isolated from others. The items have three response options: hardly ever, some of the time and often. The three items are summed into a composite scale (range = 3–9) with higher values indicating higher levels of loneliness. The short scale's validity has been assessed in both an international (Hughes et al., Reference Hughes, Waite, Hawkley and Cacioppo2004) and a British setting (Ejlskov et al., Reference Ejlskov, Wulff, Bøggild, Kuh and Stafford2017).
Adverse social relationship experiences over the lifecourse
We conceptualised social relationship adversities based on the framework of adverse childhood experiences (Dube et al., Reference Dube, Felitti, Dong, Giles and Anda2003) but with a focus solely on experiences relating to social relationships. We considered social relationship adversities in three lifestages based on the available lifecourse data source: childhood (age <18), mid-adulthood (age 36–53) and later adulthood (age 54–64). The items are shown in Figure 1. The response for each item at each lifestage was dichotomised as either having experienced the social adversity (1) or not (0), with the exception of number of times divorced or widowed which ranged from 0 to 2. For each lifestage, the items were then summed to capture the number of social relationship adversities in each lifestage and then standardised to allow for comparison across the three lifestages.
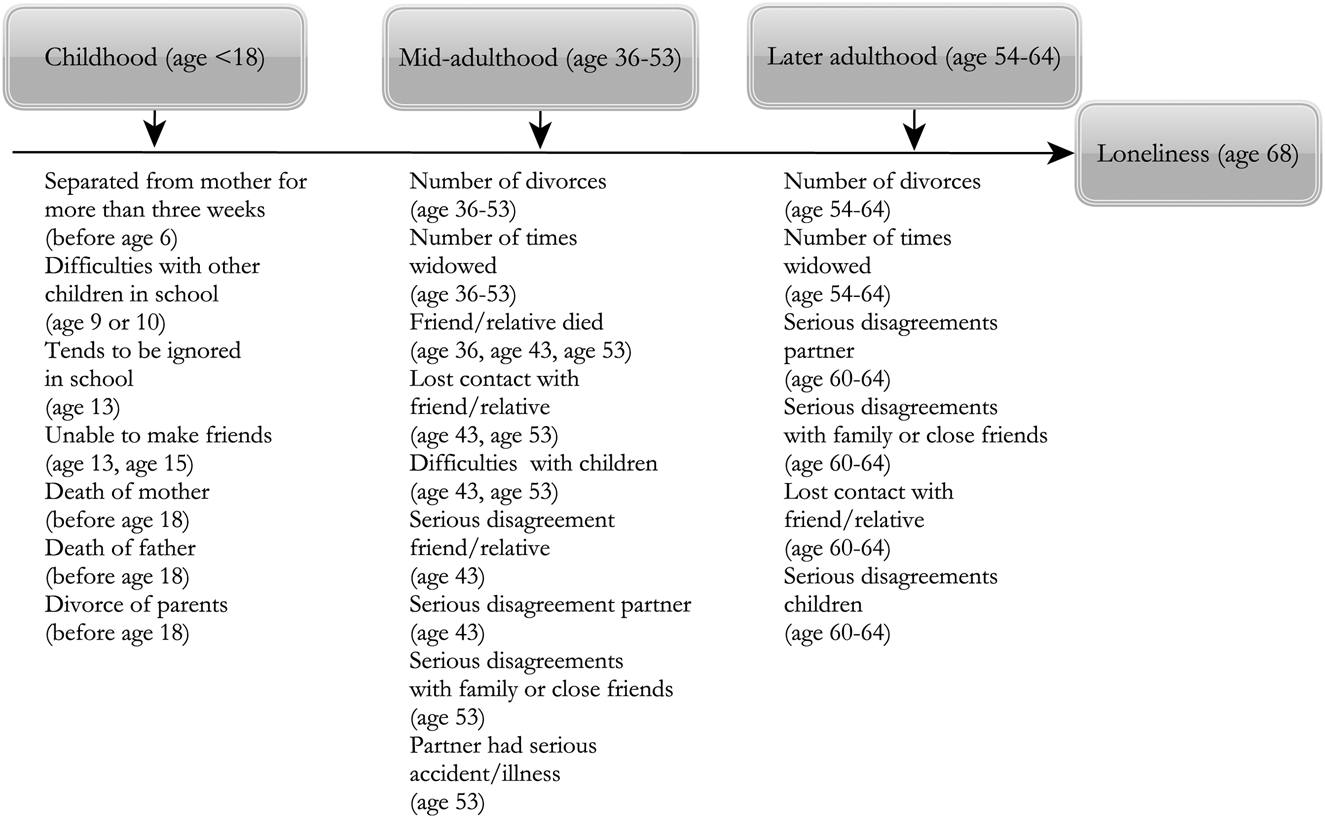
Figure 1. Overview of social relationship adversities at three lifestages.
Social relationship variables at age 68
Quantity aspects of social relationships at age 68 were measured by frequency of contact with friends or relatives (range 1–5) with higher levels indicating a lower frequency of visits. The quality of attachment to the participant's identified closest confidante was measured by the close persons questionnaire. The six items tap into the emotional support and negative aspects of the relationship between the participants and their closest confidante. Each item was ordinal with response options from ‘not at all’ to ‘a great deal’. We summed the six items to create a total quality score ranging from 6 to 30 with higher levels indicating higher quality (Stansfeld and Marmot, Reference Stansfeld and Marmot1992).
Confounding variables
We adjusted for factors that might select people into social relationship adversity. In this study we used data on the degree of extroversion and neuroticism measured at age 26 (Goldberg et al., Reference Goldberg, John, Kaiser, Lanning and Peabody1990), childhood social class measured by father's occupation (Dohrenwend, Reference Dohrenwend2006), serious illness requiring hospitalisation for 28 days or more until the age of 20 and gender.
Statistical analyses
Our analytical sample comprised 2,453 participants who completed the UCLA loneliness scale. We imputed missing exposure and covariate data using multiple imputation with the random forest technique imputing 20 data-sets (Wulff and Ejlskov, Reference Wulff and Ejlskov2017). We used ordinary least squares regression to test our hypotheses, combining estimates across imputed data-sets using Rubin's rules (Rubin, Reference Rubin1987). As the loneliness measure was highly skewed, we conducted a sensitivity analysis using logistic regression with loneliness classified as scoring 6 or above on the UCLA loneliness scale (Victor and Bowling, Reference Victor and Bowling2012). We also conducted sensitivity analyses assessing whether imputing values for participants with missing data would impact the findings. We assessed whether a high degree of missing data on social relationship adversity items would impact the findings. Thus, we re-ran the analysis removing 349 participants who had 20 per cent missing or above on social relationship adversity items to assess whether the exclusion of these would change the main findings. Further, we conducted a complete case analysis including only participants who had complete information for every variable included in the models. Each of the sensitivity analyses provided similar conclusions and are included in the online supplementary material (S1 and S2). We further re-ran the analyses with each of the single social adversity items separately to investigate whether one single item would explain the associations with loneliness in the main analysis and found no evidence of that. Lastly, we investigated whether the effects of social relationship adversity depended on gender and found no evidence of a moderating effect of gender. These analyses can be found in the online supplementary material (S3 and S4).
For each lifestage, we investigated the standardised total number of social relationship adversities (entered as a continuous variable after confirming that the assumption of a linear association with loneliness was appropriate), first controlling for gender (Models 1a, 2a and 3a) and then controlling for all confounders (Models 1b, 2b and 3b). We then included the total number of social relationship adversities in each lifestage simultaneously to examine whether social relationship adversities in earlier lifestages were independently associated with loneliness or were explained by social relationship adversities in later stages (Model 4) or by social contact at age 68 (Model 5). To investigate whether earlier social adversity moderates the association between quantity and quality of current social relationship and loneliness at age 68, we conducted separate analyses where we included an interaction term between the earlier social adversity and (a) frequency of contact with friends, (b) frequency of contact with family outside the household and (c) quality of relationship with closest confidante, respectively. We then calculated the marginal effects of frequency of contact (Figure 2) and social relationship adversities at the three earlier lifestages (Figure 3) to assess the magnitude of the moderating effect. The data management and the statistical analysis were performed using the statistical program Stata (version 14.1) and R (version 0.99.902) (R Core Team, 2017).
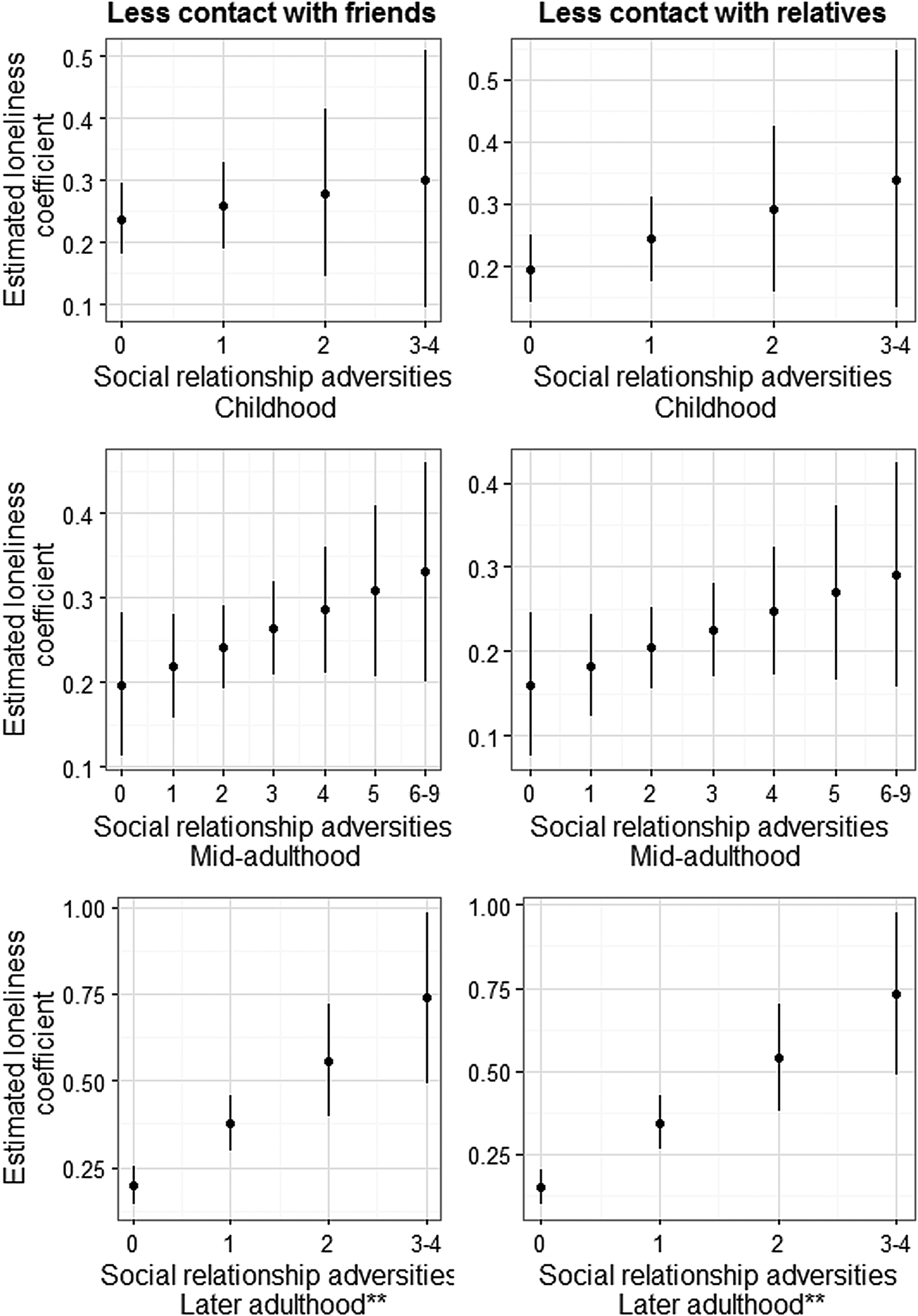
Figure 2. Associations with 95%CI between less contact with friends (left) or family (right) with loneliness conditioned on earlier experienced social relationship adversities in childhood, mid-adulthood and later adulthood.
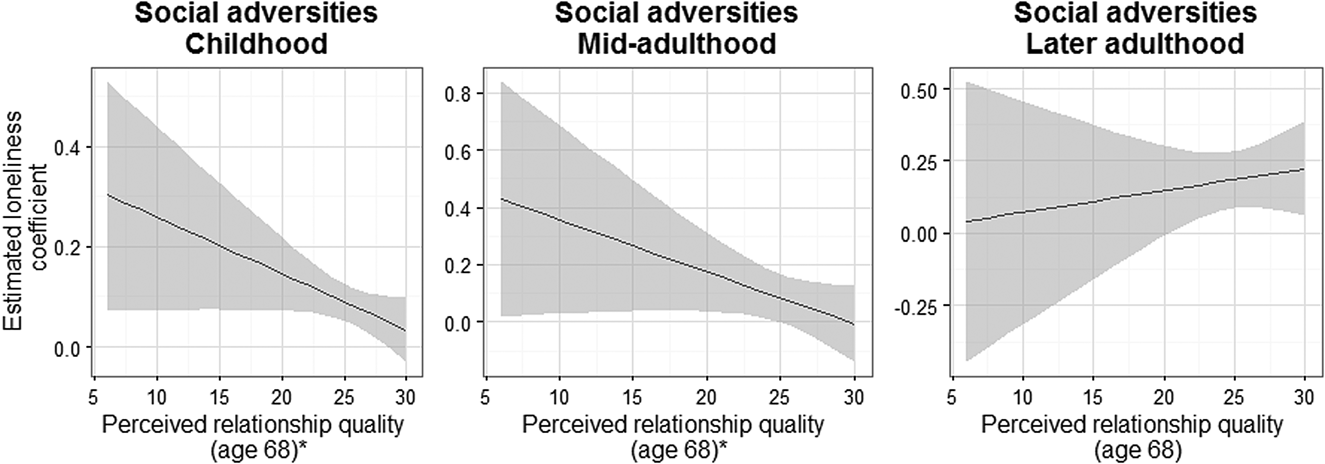
Figure 3. Associations with 95%CI between number of social relationship adversities in childhood, mid-adulthood or later adulthood with loneliness conditioned on relationship quality at age 68.
Results
Descriptive statistics
Table 1 presents the mean and standard deviation (SD) for continuous study variables, and frequency and percentage for categorical study variables. Table 2 shows the percentage of study participants in each social relationship adversity category in the three lifestages. Table 3 shows Spearman's rank correlation (ρ) between the social relationship variables. Mean loneliness in this sample was 3.8, most had daily or weekly contact with friends or family at age 68. Most of the participants (71.5%) experienced none of the childhood social relationship adversities measured in this study but 6.1 per cent experienced two or more. In mid-adulthood 59.7 per cent experienced two or more social relationship adversities with 11.6 per cent experiencing none. In later adulthood, most (79%) had experienced no social relationship adversities and 5 per cent had experienced two or more. Social relationship adversity in mid-adulthood was positively correlated with social relationship adversity in later adulthood (ρ = 0.18). Social relationship adversity experienced in later adulthood was negatively correlated with perceived relationship quality at age 68 (ρ = −0.11). All other correlations were very weak (ρ < 0.07).
Table 1. Descriptive characteristics of the study participants in the National Survey of Health and Development
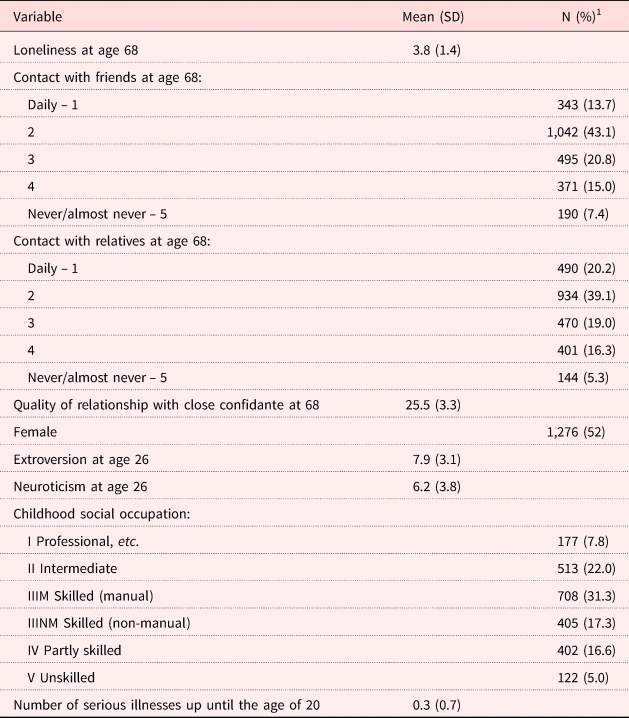
Notes: N = 2,453. 1. N is based on the complete case data; the percentage is based on all 20 imputed data-sets. SD: standard deviation.
Table 2. Distribution of the National Survey of Health and Development participants’ social relationship adversity experiences at three lifestages (childhood, mid-adulthood and later adulthood)

Notes: N = 2,453. 1. N is based on the complete case data; the percentage is an estimate based on all 20 imputed data-sets.
Table 3. Spearman's rank correlation (ρ) between social relationship variables
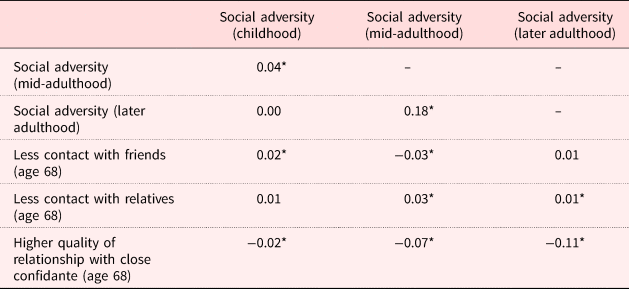
Significance level: * p < 0.05.
Social adversity at three lifestages and loneliness at age 68
Table 4 shows the results of the regression analyses (Models 1–5). Gender-adjusted models show positive associations with loneliness at age 68 and number of social relationship adversities experienced in childhood (Model 1a), mid-adulthood (Model 2a) and later adulthood (Model 3a). Models 1b, 2b and 3b show that degree of extroversion, neuroticism, childhood social status and number of childhood illnesses did not attenuate these associations. More recent social relationship adversities were more strongly related to loneliness at age 68 (fully adjusted Β = 0.05, 0.11 and 0.13 in childhood, mid-adulthood and later adulthood, respectively) than more distal ones. These associations were slightly attenuated by the inclusion of social relationship adversities at later lifestages (Model 4). Lastly, Model 5 shows that there remained an independent positive association between social relationship adversities at all three lifestages and loneliness at age 68 that was not explained by current social contact (Β = 0.04, 0.07 and 0.11 in childhood, mid-adulthood and later adulthood, respectively).
Table 4. Standardised (B) multivariable ordinary least squares estimates for social relationship variables predicting loneliness levels among the participants from the National Survey of Health and Development at age 68

Notes: 1. Adjusted for gender. 2. Adjusted for gender, extroversion, neuroticism, childhood social status and number of childhood illnesses. SE: standard error.
Moderating effects of earlier social adversity on later social relationship experiences
Figure 2 illustrates how the estimated association between less social contact at age 68 and loneliness at age 68 depended on the number of social relationship adversities earlier in life. The figure shows the associations between loneliness and less contact with friends or family by the level of social relationship adversity in childhood, mid-adulthood and later adulthood. We observed a stronger association between less contact with friends or relatives and loneliness as the number of earlier social relationship adversities increased. Among those with three or four social relationship adversities experienced in later adulthood, less-frequent contact with friends was associated with higher loneliness level (B = 0.74) compared with those who experienced no social relationship adversities (B = 0.15). The interaction terms did not attain statistical significance for childhood and mid-adulthood but did for later adulthood (p < 0.05). That is, the more earlier social relationship adversities, the stronger the negative impact of social isolation on loneliness. In addition, the higher the perceived relationship quality at age 68, the weaker the association between earlier social relationship adversity in childhood or mid-adulthood and loneliness (Figure 3). The sensitivity analysis with each social adversity item investigated separately did not indicate that any single item is driving the associations (see S3 in the online supplementary material).
Discussion
This study extends the knowledge on how experiences of social relationship adversity throughout the lifecourse are related to loneliness levels later in life. The study provides support for different pathways underlying the relationship between social relationship adversities over the lifecourse and loneliness in later life, including direct and moderated effects across four lifestages. Childhood, mid-adulthood and later adulthood social relationship adversities were associated with loneliness at age 68 independently of social relationships in later stages of the lifecourse. This suggests a long-term association between social relationship adversities in the formative years and later loneliness that is not fully explained by later social relationship experiences. The findings also indicate that the degree to which current social isolation exacerbates loneliness might depend on lifetime social experiences. Lastly, our findings suggest a high current social relationship quality may protect against some of the adverse effects of social relationship adversities in childhood and mid-adulthood.
Social relationship adversities throughout the lifecourse and loneliness in later life
While few studies have investigated the lifecourse influence of social relationship adversity on loneliness, some support for our results can be found in the literature. Dykstra and de Jong Gierveld (Reference Dykstra and de Jong Gierveld2004) investigated marital history differences in loneliness and found that previous experiences in terms of divorce matter for loneliness. Like Peters and Liefbroer's (Reference Peters and Liefbroer1997) study of marital dissolutions, we found that more-recent social relationship adversities showed a stronger association with loneliness than less-recent ones. In addition to these studies, our study broadens the scope beyond adversity in the marital relationship. Similar to studies on other aspects of psychological health (e.g. Nurius et al., Reference Nurius, Green, Logan-Greene and Borja2015), our results suggest that adverse social experiences throughout the lifecourse are associated with loneliness levels later on. Furthermore, there seems to be a dose–response relationship where greater exposure to social relationship adversities experienced at earlier lifestages mean more than any single exposure.
Several possible explanations for our finding can be proposed. First, a high number of social relationship adversities in earlier life may negatively influence one's perception of social relationships later in life. Savla et al. (Reference Savla, Roberto, Jaramillo-Sierra, Gambrel, Karimi and Butner2013) found that adverse social indicators earlier in life within one's family affect emotional closeness with family in mid- and later life (Browne and Shlosberg, Reference Browne and Shlosberg2006). Patterns of attachment behaviour shown by an individual depend partly on their current demographic and social circumstances, and partly on their experiences with attachment figures earlier in the lifecourse (Bowlby, Reference Bowlby1979; Browne and Shlosberg, Reference Browne and Shlosberg2006). A high degree of earlier experiences may also heighten maladaptive behaviour patterns, making participants with a high degree of earlier adverse social relationships more likely to experience loneliness. In addition, biological damage and altered functioning of the brain may constitute pathways of biological embedding, i.e. stress sensitisation, in which earlier social relationship experiences affect later loneliness levels (Danese and McEwen, Reference Danese and McEwen2012). While further studies are needed to confirm the findings of this study, our results indicate that cognitive responses in social situations may be affected by earlier social experiences. Thus, in line with suggestions from Masi et al. (Reference Masi, Chen, Hawkley and Cacioppo2011), further studies may benefit from a stronger focus on how to best strengthen cognitive responses in social situations. Such a focus has the potential to mitigate potential earlier experiences that otherwise might lessen the efficacy of opportunities for social engagement by focusing on altering the perception of social situations.
We also hypothesised that social relationship adversities would be positively correlated with each other throughout the lifecourse following the chains of risk lifecourse model. We based our expectation on previous studies that have shown that early social relationship adversities may launch chains of disadvantages in social relationships over the lifecourse (Dykstra and de Jong Gierveld, Reference Dykstra and de Jong Gierveld2004; Caspi et al., Reference Caspi, Harrington, Moffitt, Milne and Poulton2006; Katz et al., Reference Katz, Conway, Hammen, Brennan and Najman2011; Umberson et al., Reference Umberson, Williams, Thomas, Liu and Thomeer2014). These findings are only partially supported in this study with at most low to moderate correlations between social relationship measures at the different lifestages. Only social relationship adversity in mid-adulthood was positively correlated with social relationship adversity in later adulthood. For social relationship adversity experienced in later adulthood, we found a negative correlation with perceived relationship quality at age 68. The discrepancy between previous studies and the results of this study might be due to the different measures of social relationship adversities in this way reflecting differences in chains of risk according to whether investigating single or cumulative exposures. However, it might also reflect that the available measures of social relationship adversities in childhood in this study were too crude to assess this hypothesis in great detail, as well as the long timespan between childhood and mid-adulthood. Thus, future studies might want to assess other aspects of childhood relationship adversities.
The importance of earlier social relationship adversities for the association between social relationships and loneliness in later life
We hypothesised that earlier experienced social relationship adversities may interact with later-life social relationship exposures, thereby either enhancing or decreasing the risk of feeling lonely. Our analysis provides partial support for this hypothesis. This is an important finding that might shed light on some of the lifecourse processes that influence how similar social circumstances affect people differently depending on earlier social experiences. Our results suggest that social relationship adversities in later adulthood influence the extent to which social isolation (i.e. low social contact) is associated with loneliness at age 68. The positive association between lack of social contact with friends or family and loneliness was stronger for those who had more social relationship adversities (especially in later adulthood).
In the literature, social isolation is often highlighted as a key predictor of loneliness (Hawkley, Reference Hawkley and Pachana2015) and for this reason is often the subject of interventions aimed at alleviating loneliness (Dickens et al., Reference Dickens, Richards, Greaves and Campbell2011; Saito et al., Reference Saito, Kai and Takizawa2012). Thus, a key finding in this study is that the extent to which social isolation exacerbates loneliness depends on lifetime experiences. The explanation for this influence of earlier social relationship adversities might lie in how earlier experiences influence the standard for social comparisons (Peplau and Perlman, Reference Peplau, Perlman, Peplau and Perlman1982). In the introduction, we suggested that social relationship adversities may become embedded biologically (Nurius et al., Reference Nurius, Green, Logan-Greene and Borja2015) and socially (Matthews et al., Reference Matthews, Gallo and Taylor2010). We proposed that individuals with many social relationship adversities earlier in life react more negatively to being socially isolated because their social resilience is lower and their sensitivity and attitude towards social relationships is more negative. However, while there are similar tendencies for the social relationship adversities experienced in childhood and mid-adulthood, these did not attain statistical significance. This attenuation of effects as the adverse social relationships grow more distant suggests that not only is the direct impact of social relationship adversities on loneliness diminished over time but also how strongly earlier social relationship adversities exacerbate the influence of current social isolation on loneliness.
This is in line with our main findings that more recent social relationship adversities are more strongly related to loneliness and the study from Peters and Liefbroer (Reference Peters and Liefbroer1997). Thus, it seems that current social isolation can amplify the effect of earlier adversities. However, the further back in time the social relationship adversities have occurred, the less of an impact they have. If these findings can be replicated in other studies, it may point towards how the lasting strain of social relationship adversities affect later biological and social responses to social isolation diminishing over time.
In line with our expectations, we also found support for the ameliorating effect of a current high quality of social relationships on the effect of social relationship adversity earlier in life on later-life loneliness. The ameliorating effect may occur due to the many emotional and social resources a high degree of quality of social contact can provide the individual with (Thoits, Reference Thoits2011). Umberson et al. (Reference Umberson, Williams, Thomas, Liu and Thomeer2014) have suggested that adults’ supportive relationships can protect against the effects of childhood adversities on adult health which is in support of our more specific finding on childhood and mid-adulthood social relationship adversity and loneliness in later life. In other words, these findings suggest that having a secure and high-quality attachment later in life may protect against some of the strains that earlier experienced social adversities have inflicted on the individual. However, while the tendency was clear, further studies are needed to confirm this finding.
Study strengths and limitations
Among the strengths of this study, we count the longitudinal framework and population-based data source. By having data on social relationship adversities that have been prospectively gathered we can rule out any potential recall bias. We used data on a wide range of social relationship adversities. The single-item analysis indicates that no single item seems to be driving the associations. However, the items used to measure social relationship adversity and the number of items considered at the different lifestages are not the same and thus we cannot compare the influence of specific social relationship adversities across the lifestages. Further, the duration used for assessment of social relationship adversities differs. For this reason, we have standardised the variables to be able to compare the effect sizes. The use of the NSHD further makes it possible to rule out any potential bias coming from age differences but generalising these results to other birth cohorts should be done cautiously. Also, we cannot rule out the possibility of attrition bias. It is possible that participants with more social adversity in earlier lifestages were less likely to respond. However, analyses conducted of the NSHD at age 60–64 showed that this study is broadly comparable to the population of the United Kingdom of the same age on socio-economic indicators and that affective symptoms were not associated with non-response at that data collection point (Stafford et al., Reference Stafford, Gardner, Kumari, Kuh and Ben-Shlomo2013).
Conclusion
This study extends the current knowledge on how earlier social relationships influence later social experiences. A key finding of this study is that social relationship adversities experienced throughout the lifecourse may continue to influence loneliness levels much later in life, with more proximal social relationship adversities being more strongly related to loneliness. Another key finding is that the extent to which social isolation at later lifestages exacerbates loneliness depended on lifetime social experiences, being greater for those with more adverse social relationship experiences previously. Similarly, earlier adversities were more weakly associated with loneliness at higher levels of current close relationships. Those targeting or developing interventions to reduce loneliness in later life may benefit from measuring individual's earlier social relationship experiences and assessing how this affects their cognitive responses to social situations.
Author ORCIDs
Linda Ejlskov, 0000-0003-4917-9200.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0144686X19000345
Data
Data used in this publication are available to bona fide researchers upon request to the National Survey of Health and Development Data Sharing Committee via a standard application procedure. Further details can be found at http://www.nshd.mrc.ac.uk/data (doi:10.5522/NSHD/Q101; doi:10.5522/NSHD/Q102; doi:10.5522/NSHD/Q103).
Financial support
This work was supported by the UK Medical Research Council which provides the core funding for the MRC National Survey of Health and Development and DK and MS (grant numbers MC_UU_12019/1, MC_UU_12019/5).
Ethical standards
All procedures performed in studies involving human participants in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. At the age 68 data collection ethical approval was obtained from the NRES Queen Square REC (14/LO/1073) and Scotland A REC (14/SS/1009).









 Open access
Open access