
Abstract
Background: Novel antithrombotic agents such as hirudin have shown promise in the therapy of acute coronary syndromes. PEG-hirudin (polyethyleneglycol conjugated hirudin) has been developed to provide a longer plasma half-life and more stable antithrombotic plasma levels. Privious trials indicated a narrow therapeutic window for hirudin and a number of aPTT (activated partial thromboplastin time)-monitored trials investigating hirudin in acute coronary syndromes had to be stopped because of intracranial bleeding complications.
Objectives: The present study evaluates the ecarin clotting time (ECT), a parameter based on the conversion of prothrombin by the snake venom enzyme ecarin, for the monitoring of PEG-hirudin therapy.
Methods: Plasma from either healthy volunteers (n=20) or from patients (n=10) suffering from unstable angina pectoris (UAP) was spiked with increasing PEG-hirudin concentrations. In a prospective randomized clinical trial patients with UAP were treated with intravenous PEG-hirudin or heparin over 72 hours. Patients were randomized to the following treatment groups: (1) heparin control group, n=15; (2) PEG-hirudin low dose (0.1[emsp4 ]mg/kg bolus, 0.01[emsp4 ]mg/kg/h infusion), n=19; (3) intermediate dose (0.15[emsp4 ]mg/kg and 0.015[emsp4 ]mg/kg/h), n=17; 4) high-dose (0.2[emsp4 ]mg/kg and 0.02[emsp4 ]mg/kg/h), n=16. Spiked plasma samples and plasma from UAP patients treated with i.v. PEG-hirudin were analyzed for aPTT, ECT, and PEG-hirudin levels.
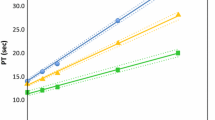
Results: A linear correlation up to the highest therapeutic concentrations could be observed between PEG-hirudin plasma concentrations and the ECT. This was true for both plasma samples spiked with PEG-hirudin in vitro as well as for samples taken from patients treated with i.v. PEG-hirudin (correlation coefficient 0.9, respect.) In contrast the aPTT did not show a reliable linear correlation to PEG-hirudin concentrations.
Conclusion: Monitoring of PEG-hirudin therapy by ECT may help to avoid inadequate anticoagulation or overdosing. Thus, the safety and efficacy profile of PEG-hirudin therapy is likely to be enhanced by ECT monitoring.
Similar content being viewed by others


References
Weitz JI. Activation of blood coagulation by plaque rupture: Mechanisms and prevention. Am J Cardiol 1995;75:18B–22B.
Bossavy J, Sakariassen K, Rübsamen K, Thalamas C, Boneu B, Cadroy Y. Camparison of the antithrombotic effect of PEG–hirudin and heparin in a human ex vivo model of arterial thrombosis. Atheroscl Thromb Vasc Biol 1999;19:1348–1353.
Rübsamen K, Hornberger W. Prevention of early reocclusion after thrombolysis of copper coil–induced thrombi in the canine carotid artery: comparison of PEG–hirudin and unfractionated heparin. Thromb Haemost 1996;76(1):105–110.
Esslinger HU, Haas S, Maurer R, Lassmann A, Dübbers K, Mueller–Peltzer H. Pharmacodynamic and safety results of PEG–hirudin in healthy volunteers. Thromb Haemost 1997;77(5):911–919.
Zeymer U, von Essen R, Tebbe U, et al. Recombinant hirudin and front–loaded alteplase in acute myocardial infarction: final results of a pilot study. HIT–I (hirudin for the improvement of thrombolysis). Eur Heart J 1995;(Suppl D):22–27.
Cannon C, McCabe C, Henry T. A pilot trial of recombinant desulfatohirudin compared with heparin in conjunction with t–PA and aspirin for acute myocardial infarction: Results of TIMI–V trial. J Am Coll Cardiol 1994;23:993–1003.
Lee L. Initial experience with hirudin and streptokinase in acute myocardial infarction: results of TIMI–6 trial. J Am Coll Cardiol 1995;75:7–13.
Antman E. Hirudin in acute myocardial infarction. Safety report from the thrombolysis and thrombin inhibition in myocardial infarction (TIMI) 9A trial. Circulation 1994;90:1624–1630.
The global use of strategies to open occluded coronary arteries (GUSTO) IIa investigators. Randomization of intravenous heparin versus recombinant hirudin for acute coronary syndromes. Circulation 1994;90: 1631–1637.
Neuhaus K, van Essen R, Tebbe U, et al. Safety observations from the pilot phase of the randomized r–hirudin for improvement of thromboiysis (HIT–III) study. Circulation 1994;90:1638–1642.
The GUSTO–IIb investigators. A comparison of recombinant hirudin with heparin for the treatment of acute coronary syndromes. N Engl J Med 1996;335:775–782.
The OASIS investigators. Comparison of the effects of two doses of recombinant hirudin compared with heparin in patients with acute myocardial ischemia without ST elevation: A pilot study. Circulation 1997;96:769–777.
The OASIS investigators. Effects of recombinant hirudin (lepirudin) compared with heparin on death, myocardial infarction, refractory angina, and revascularisation procedures in patients with acute myocardial ischemia without ST elevation: a randomized trial. Lancet 1999;353:429–438.
Nowak G, Bucha E. Quantitative determination of hirudin in blood and body fluids. Semin Thromb Hemost 1996;22:197–202.
Spannagl M, Bichler J, Birg A, Lill H, Schramm W. Development of a chromogenic substrate assay for the determination of hirudin in plasma. Blood Coagul Fibrinolysis 1991;2:121–127.
Pötsch B, Hund S, Madlener K, Unkrig C, Müller–Berghaus G. Monitoring of recombinant hirudin: assessment of a plasma–based ecarin clotting time assay. Thromb Res 1997;86:373–383.
Pötsch B, Madlener K, Seelig C, Riess C, Greinacher A, Müller–Berghaus G. Monitoring of r–hirudin anticoagulation during cardiopulmonary bypass–assessment of the whole blood ecarin clotting time. Thromb Haemost V;77:920–925.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Moser MD, M., Ruef MD, J., Peter MD, K. et al. Ecarin Clotting Time but not aPTT Correlates with PEG-Hirudin Plasma Activity. J Thromb Thrombolysis 12, 165–169 (2001). https://doi.org/10.1023/A:1012975522037
Issue Date:
DOI: https://doi.org/10.1023/A:1012975522037