
Abstract
Androgen deprivation therapy (ADT) is the standard treatment for advanced prostate cancer, but its effect on cardiovascular and metabolic function in Asian patients is still inconclusive. We prospectively assess the effects of ADT on 36 patients with advanced prostate cancer, with reference to another 24 prostate cancer patients not requiring ADT, for 2 years. Patients’ anthropometric, metabolic and vascular parameters were assessed every six-monthly. The baseline parameters of the two groups were comparable. There was a significant negative effect of the usage of ADT on the changes in BMI (p = 0.020), waist to hip ratio (p = 0.005), body fat percentage (p = 0.012), and high-density-lipoprotein (p = 0.012). ADT-patients were 4.9 times more likely to have metabolic syndrome at 24 months. (CI 0.889–27.193, p = 0.068). The Framingham risk score (p = 0.018) and pulse-wave-velocity (p = 0.024) for ADT-group were also significantly higher than controls, which signified increase in cardiovascular risk. Although there was no statistically significant difference in ischemic cardiovascular events between two groups, a trend for more events in ADT-group was observed. Therefore, Asian patients have increased cardiovascular and metabolic risks after being treated with ADT for two years. Appropriate counselling and monitoring of associated complications with ADT are essential.
Similar content being viewed by others
Introduction
Since the ground-breaking work of Charles Huggins on the role of androgen deprivation therapy (ADT) in prostate cancer, it has become one of the key players in the management of prostate cancer (PCa), particularly in metastatic disease1. Even in castration resistant stage, ADT is still considered the backbone therapy for most patients1. Currently, beside the traditional bilateral orchidectomy (surgical castration), there were also luterizing hormone releasing hormone agonist (LHRH agonist) and antagonist (LHRH antagonist) available as options for medical castration1. The choice of treatment would be depend on the clinical conditions (need of rapid testosterone suppression), financial implications, patient preference etc.
With the advancements in clinical care, the overall survival of prostate cancer patients has prolonged2. But there is also increasing concern about potential long-term side effects and even mortality related to ADT in patients with prostate cancer. In some early single-arm prospective studies, ADT were found to be associated with increased body weight and body fat3, reduced insulin sensitivity and increased arterial stiffness4. These concerns were further supported by observational studies, which showed that patients who received ADT had increased incidence of diabetes, myocardial infarction and even cardiac mortality5,6. Unfortunately these results were inconsistent. Some prospective randomized clinical studies reported that ADT were not associated with increase in cardiovascular risk7. Despite these controversies, a joint statement was issued by the American Urological Association, the American Society for Radiation Oncology and the American Heart Association to raise physicians’ awareness about the potential association between ADT and cardiovascular disease8. Nevertheless, the evidence is still inconclusive even in latest meta-analyses9.
The situation in Asia is also controversial, as information on ADT is scanty. Large-scale prospective randomized studies on prostate cancer in Asia are lacking. Studies related to ADT were mainly observational or retrospective in nature. The earliest information was from the J-Cap registry study, which showed that the incidence of cardiovascular events in ADT patients was similar to that of the general population10. Thereafter, several groups reported investigations regarding this topic, with some showing increased cardiovascular risk in patients managed with ADT11,12, while others suggesting otherwise13,14,15. Therefore, there is a need for further studies to assess the effect of ADT on prostate cancer patients, including the fundamental effect on body compositions, cardiovascular related metabolic changes and cardiovascular risks.
Methods
This was a prospective cohort study. The objective of this study is to assess the cardiovascular and metabolic effects of ADT in Chinese patients who were diagnosed to have PCa. The study was approved by the institutional ethics committee (Joint Chinese University of Hong Kong-New Territories East Cluster Clinical Research Ethics Committee) and conducted according to the principles of the Helsinki Declaration on human experimentation. Adult Chinese patients with histological diagnosis of PCa whom decided for long term ADT monotherapy were prospectively recruited for the study in our centre. ADT could be in the form of bilateral orchidectomy, luteinizing hormone-releasing hormone (LHRH) agonists or LHRH antagonist. Maximal androgen blockage was not our usual practice, additional short course of androgen receptor blocker was only used as flare prevention in some patients receiving LHRH agonist. Written informed consent was obtained from all subjects.
Additional age-matched Chinese patients with the diagnosis of PCa, who did not receive ADT treatment or other active treatment, were recruited as control arm. These patients were diagnosed to have localized disease and had undergone radical surgery or managed conservatively for their cancer. If the patient was not able to provide consent or comply with the follow-up arrangement, or if based on clinical judgement that the life expectancy of the patient was limited, the patient would be excluded from the study.
Study protocol
Written informed consent was obtained from all subjects. All patients then underwent a series of clinical, biochemical and vascular function assessment at baseline, followed by 6-monthly assessment for two years to determine their metabolic and cardiovascular status.
Clinical assessment
Anthropometric parameters including patients’ height, body weight, BMI, waist and hip circumference were measured. Waist circumference was measured at the level of umbilicus. Hip circumference was defined as the maximum circumference of the buttock. A skinfold caliper was used for the measurement of skinfold thickness for the estimation of the total amount of body fat. Four areas of the body, biceps (front side of the mid-upper arm), triceps (back side of the mid-upper arm), shoulder blade (just below the subscapular) and supra-iliac (just above the iliac crest) were measured. The sum of the four measurements was then used to estimate the body fat percentage using the Durnin and Womersley formula16. All the above measurements were performed when the patient stood relaxingly in a warm examination room with privacy. Blood pressure and pulse were measured twice with 5-min interval by an automated machine after resting for 5 min. During each follow-up, besides repeating these measurements, cardiovascular events of the patients were recorded.
Laboratory
Blood samples were collected from patients after overnight fasting for the measurements of sugar level, total triglycerides (TG), total cholesterol (TC), low density lipoprotein cholesterol (LDL-C), high density lipoprotein cholesterol (HDL-C) and complete blood picture (including haemoglobin level). Testosterone level was also measured to confirm the castration in patients receiving ADT.
Vascular function assessment
In this study, the central and peripheral arterial conditions were assessed by brachial-ankle pulse wave velocity (baPWV) and Ankle brachial index (ABI), respectively. Brachial-ankle pulse wave velocity is an approach to assess central arterial stiffness, which is well-recognized to be associated with cardiovascular disease17,18. The system involved four separate cuffs applied to the four limbs and automatic measurement of the blood pressure and pulse wave in the limbs. Combined with the information on body height, it will provide the baPWV of the measured individual. The faster the baPWV, the stiffer the central blood vessel, and higher cardiovascular risk.
Ankle brachial index (ABI) is an index for the assessment of vascular occlusion due to peripheral vascular disease. It is defined as the ratio of the blood pressure of the lower limb, as measured at the ankle, to the blood pressure of the upper limb, as measured at the upper arm (brachial artery). The lower the ratio, i.e. greater difference between the upper and lower limb, the more severe arterial occlusion by peripheral arterial disease.
In this study, both baPWV and ABI were assessed by the Vascular Profiler-1000 machine (Omron, Kyoto, Japan) using the oscillometric cuff technique. Patient was asked to rest in supine position in a quiet and warm environment for at least 10 min. The 4 measuring cuffs would be applied to both arms and ankles, respectively. The machine would then automatically measure the baPWV and ABI. After inputting the height of the patient, baPWV was calculated automatically between the ankle and brachial pulse waveform for both sides. The average of the two sides’ readings would be used for the assessment of baPWV of the subjects in our study.
Overall assessment
As many parameters were measured in our study, we used the Framingham Risk Score as the primary endpoint to assess the overall cardiovascular risk of the patients during the study period. The Framingham Risk Score is a gender-specific algorithm based on multiple cardiovascular risk factors including age, smoking status, blood pressure level, serum total cholesterol and HDL-cholesterol level for the estimation of the 10-year risk of developing cardiovascular disease19. We also applied the National Cholesterol Education Program (NCEP)/Adult Treatment Panel III (ATPIII) guidelines to assess whether the patients had increased risk of developing metabolic syndromes after ADT treatment20.
Statistical analysis
All data were reported as mean ± SD unless otherwise specified. Student’s t test and Fisher’s exact test were used for the comparison between ADT and control groups. Two-way mixed ANOVA was performed to evaluate if any change in the outcome variables is the result of the interaction between usage of ADT and time. All tests were two-sided, with significance set at 5%. Statistical analyses were performed by SPSS (Chicago, IL).
Take home message
Androgen deprivation therapy in advanced prostate cancer in Chinese are associated with increased cardiovascular and metabolic risks. Appropriate counselling and monitoring of these complications are essential.
Results
From July 2011 to January 2016, 36 patients with prostate cancer managed with primary ADT alone were recruited to the study. Amongst them, 20 patients had metastatic disease and the other 16 patients were diagnosed with locally advanced disease. The number of patients chose bilateral orchidectomy, LHRH agonist and LHRH antagonist as the initial ADT were 18, 11 and 7, respectively (Table 1). The choice of medical or surgical castration depended on patient preference and also financial implication, as the cost of medical castration was not reimbursed. Moreover, LHRH antagonist was only available in 2013 in our area and was mainly used in patients with high volume metastasis (for rapid testosterone suppression) and increased cardiovascular risk. Due to the frequent injection schedule (monthly) and higher cost for LHRH antagonist (degarelix), some patients initially started on LHRH antagonist changed to use 3-monthly LHRH agonist during their course of treatment. Another 24 patients with localized prostate cancer were also recruited as control for the study. Eighteen of them had radical prostatectomy performed while the other six were under watchful waiting or active surveillance. The average time between diagnosis and recruitment for the ADT arm and the control arm was 5.5 and 38.5 months, respectively.
The baseline characteristics and blood parameters of the patients were listed in Tables 2 and 3. The mean age of the whole group was 74.1 (range 52 to 90) years old, and there was no significant difference between the two groups. Most of the patients had baseline cardiovascular and metabolic diseases. The most common ones were hypertension, hyperlipidaemia and diabetes. About 10% of patients in each arm had a history of cerebrovascular diseases. Four patients (11.1%) in the ADT arm had a history of ischemic heart disease. However, there was no significant difference between the two groups for these medical problems. Similarly, there was no difference in the smoking status between the two groups. The baseline body weight, body height, body mass index (BMI), waist circumference, hip circumference, waist-hip ratio and body fat composition between the two groups were also similar. Fourteen patients (38.89%) in the ADT arm and seven patients (29.17%) in the control arm had metabolic syndrome (p = 0.439). The baseline Framingham risk score for the ADT group and control group were 0.42 and 0.40 respectively (p = 0.720). For vascular assessment, the baseline ankle-brachial index (ABI) for ADT and control group were 1.03 and 1.13 (p = 0.008). The baseline pulse wave velocity (PWV) for ADT and control group were 1766 cm/s and 1779 cm/s (p = 0.889).
There were two patients in the ADT group who withdrew from the study due to personal reasons. Ten ADT patients and one control patient died before 24 months. The causes of death in the ADT group included progression of prostate cancer (6, 16.67%), right cerebellar haemorrhage (1, 2.78%), sepsis (2, 5.56%), and brain stem glioma (1, 2.78%). One patient in the control arm died of ischemic stroke. In summary, there were 24 ADT patients and 23 control patients who completed the 2-year assessment for analysis. (Fig. 1).

Flowchart of patient follow-up information.
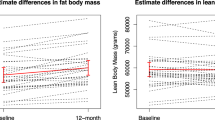
There was a significant interaction between usage of ADT and time in explaining BMI (F1, 44 = 5.87, p = 0.020), waist to hip ratio (F1, 45 = 5.99, p = 0.018) and body fat percentage (F1, 44 = 6.92, p = 0.012) (Table 3). The BMI for ADT group and control group changed from baseline 23.75 ± 3.08 and 23.15 ± 2.83 to 24.37 ± 2.97 and 22.90 ± 2.87, respectively. The waist to hip ratio for ADT group and control group changed from baseline 0.96 ± 0.06 and 0.95 ± 0.06 to 0.98 ± 0.06 and 0.93 ± 0.07 respectively. The body fat percentage for ADT group and control group changed from baseline 29.89 ± 5.49 and 28.32 ± 3.60 to 32.44 ± 3.65 and 28.12 ± 3.17 respectively. These changes suggested patients who received ADT had increased risk of central obesity.
There was a statistically significant interaction between usage of ADT and time in explaining high density lipoprotein (HDL) (Table 3). The HDL for ADT group and control group changed from baseline 1.53 ± 0.41 and 1.54 ± 0.39 to 1.26 ± 0.32 and 1.60 ± 0.43, respectively. On the other hand, there was no significant difference between the two groups in 24-month change in total cholesterol (F1, 43 = 0.07, p = 0.791), triglyceride (F1, 43 = 0.18, p = 0.673), low density lipoprotein (LDL) (F1, 43 = 0.08, p = 0.779), fasting blood glucose (F1, 43 < 0.01, p = 0.989) and glycosylated haemoglobin level (HbA1C) (F1, 32 = 0.49, p = 0.491). Meanwhile, patients in the ADT arm were 4.918 times more likely to have metabolic syndrome at 24 months compared to control group after adjusting for the baseline (CI 0.889, 27.193, p = 0.068).
The Framingham risk score for ADT group and control group changed from baseline of 41.74% ± 20.94% and 39.79% ± 19.86% to 47.24% ± 22.86% and 37.67% ± 19.93% respectively (Fig. 2a). The results showed that the change in Framingham risk score was significantly different for the two groups (F1, 43 = 6.04, p = 0.018).

Changes in (a) Framingham risk score and (b) pulse-wave velocity over time for the two groups. Study ADT group, Control control group.
Vascular assessment showed that there was a significant interaction between usage of ADT and time in explaining pulse wave velocity (PWV) (F1, 41 = 5.51, p = 0.024). The PWV for ADT group and control group changed from baseline 17.66 ± 4.30 and 17.79 ± 2.70 to 20.52 ± 6.34 and 18.21 ± 3.75, respectively (Fig. 2b). There was no significant difference between the two groups in 24-month change in systolic blood pressure (F1, 45 = 2.03, p = 0.161), diastolic blood pressure (F1, 45 = 2.17, p = 0.148) and ankle-brachial index (ABI) (F1, 42 = 0.28, p = 0.602).
There were three (8.33%) patients in the ADT group and one (4.17%) patient in the control group who developed ischemic stroke during the 2 year follow-up. Another 3 (8.33%) patients in the ADT group had new onset ischemic heart disease diagnosed during the study period. However, there was no statistically significant difference in ischemic cardiovascular events between the two groups (p = 0.330).
Discussion
In this prospective comparative study, prostate cancer patients who received ADT had a significant increase in body weight, body fat and central obesity than those without ADT. They also had increased chance of developing metabolic syndrome, higher Framingham risk score and increased pulse wave velocity at the end of 2-year follow-up. All these information points towards that ADT would increase cardiovascular risk and metabolic syndrome. It also led to increase in arterial stiffness and atherosclerosis.
Despite publications on multiple studies and meta-analyses, the effect of ADT on patients was still controversial. In general, meta-analysis of observational studies supported a positive relationship between increased cardiovascular risk and ADT, while the results from randomized studies were negative9. Hu et al. proposed that the reason for the conflicting outcomes might be related to the study designs9. For observational studies, there may be problems related to confounding factors, treatment adherence and outcome reporting bias. Similarly for randomized studies, underpower of studies, inadequate follow-up period, and selection bias, etc. might contribute to the negative findings. Nevertheless, there is a general consensus that there is an association between ADT usage and cardiovascular risk21.
While most of the observational studies on Caucasian population indicated that ADT would increase the cardiovascular risk of patients9,22, the results for Asians suggested otherwise. In several observational studies based on national insurance databases in different populations, the results did not show an increased cardiovascular risk in Asian patients receiving ADT13,14,15. The reason for this discrepancy was uncertain. It might be related to the study sample size, racial difference in response to ADT, the overall lower baseline cardiovascular risk of Asian population, and underdiagnosis of cardiovascular events, etc. Nevertheless, this observation reminded us to be cautious in applying findings from Caucasian studies to Asian population.
Therefore, we performed this study to try to bridge the current knowledge gap, the insufficient information about the effect of ADT on Asian population. We planned to overcome some of the pitfalls in previous studies, such as no control arm and short follow-up period3,4. While it would be unethical to randomize patients for ADT or not, we included a comparable control arm with prostate cancer patients who did not require ADT. We also included physical, blood and vascular assessments for our patients, with follow-up for up to two years, which was much longer than similar studies3,4. While we could continue for even longer follow-up, the dropout rate for ADT arm would be high due to the nature of underlying disease. Six patients in the ADT group developed ischemic cardiovascular events, compared to only one patient in the control group. However, due to the small sample size, this was not statistically significant. Nevertheless, our data suggested that there was a negative effect of ADT on cardiovascular risk and metabolic parameters in our population.
Development and progression of atherosclerosis is believed to be one of the underlying mechanisms related to the increase in cardiovascular risk in patients receiving ADT23. In a previous Caucasian study, the usage of ADT was shown to result in significant increase in pulse wave velocity after 3 months of therapy, which is a recognized indicator for major vessels stiffness, and in turn atherosclerotic changes4,24,25. However, in a report from Japanese group, there was no significant overall increase in pulse wave velocity after six months of ADT26. Our results provided the longest prospective data, up to two years, on the effect of ADT on pulse wave velocity, which further support the initial findings from Caucasian studies. The difference in the results between our study and Oka et al. could be due to study duration, assessment method, or patients’ background. Again, further studies to investigate this area are needed in order to have a better understanding of the situation.
The relative small sample size and single centre experience might limit the generalizability of our findings to other populations. As we aimed to have longer follow-up for our patients, we recruited mainly patients with relatively good performance status in the study. Unfortunately, despite careful selection, only roughly two-thirds of the patients with ADT could survive to the end of the two-year follow-up. Moreover, the repeated assessments had also made some patients hesitate to participate in our study. All these contributed to the slow recruitment rate of the study. In addition, some patients have used LHRH antagonist for treatment, which might have potential cardiovascular protective effect27, and hence might affecting the overall incidence of cardiovascular events. Therefore, the small sample size of our study might not be able to detect any significant difference in clinical cardiovascular events, including assessing the effect of different ADT approaches on the outcomes. Despite these, our results had showed convincing evidence of the metabolic and cardiovascular effects of ADT in our patients.
Currently, there are other studies in Asia that are trying to provide more information about the effect of ADT in prostate cancer patients. For example, the real-life evaluation of the effect of ADT in prostate cancer patients in Asia (READT Asia Study) (Clinical trials registration NCT03703778) is a multi-nation prospective study to assess the effect of ADT in prostate cancer patients. The initial result showed that there was a high prevalence of cardiovascular risk factors in Asian prostate cancer patients28. Hopefully the study will provide more information on the effects of ADT in Asian patients.
Nevertheless, the result of our study would support the incorporation of additional measures in managing patients treated with ADT to minimize the potential metabolic and cardiovascular harm to patients. The recommended ABCDE approach should be introduced to all patients29. These include awareness of the condition and patient education on diet, smoking and exercise, careful monitoring of blood pressure, blood sugar and lipid level for patients, appropriate patient referral to cardiological assessment and usage of pharmacological agents, including aspirin, for high risk patients. For patients with high cardiovascular risk, the usage of LHRH antagonist had shown to have less cardiovascular complications when compared to LHRH agonist27,30. All these measures would help to improve the overall standard of care and survival of patients. Currently, there are also studies exploring the use of novel alternate treatments for managing advanced prostate cancer31,32. However, most of the these treatments are still in investigational stage, and further studies are needed to assess their roles in clinical management, and also whether they could replace ADT as the primary therapy for patients.
References
Shore, N. D. et al. Optimizing the role of androgen deprivation therapy in advanced prostate cancer: challenges beyond the guidelines. Prostate 80, 527–544 (2020).
Damodaran, S., Kyriakopoulos, C. E. & Jarrard, D. F. Newly diagnosed metastatic prostate cancer: has the paradigm changed?. Urol. Clin. N. Am. 44, 611–621 (2017).
Smith, M. R. et al. Changes in body composition during androgen deprivation therapy for prostate cancer. J. Clin. Endocrinol. Metab. 87, 599–603 (2002).
Smith, J. C. et al. The effects of induced hypogonadism on arterial stiffness, body composition, and metabolic parameters in males with prostate cancer. J. Clin. Endocrinol. Metab. 86, 4261–4267 (2001).
Lu-Yao, G., Stukel, T. A. & Yao, S. L. Changing patterns in competing causes of death in men with prostate cancer: a population based study. J. Urol. 171, 2285–2290 (2004).
Keating, N. L., O’Malley, A. J. & Smith, M. R. Diabetes and cardiovascular disease during androgen deprivation therapy for prostate cancer. J. Clin. Oncol. 24, 4448–4456 (2006).
Nguyen, P. L. et al. Association of androgen deprivation therapy with cardiovascular death in patients with prostate cancer: a meta-analysis of randomized trials. JAMA 306, 2359–2366 (2011).
Levine, G. N. et al. Androgen-deprivation therapy in prostate cancer and cardiovascular risk. Circulation 121, 833–840 (2010).
Hu, J. R. et al. Cardiovascular effects of androgen deprivation therapy in prostate cancer: contemporary meta-analyses. Arterioscler. Thromb. Vasc. Biol. 40, e55–e64 (2020).
Akaza, H. Future prospects for luteinizing hormone-releasing hormone analogues in prostate cancer treatment. Pharmacology 85, 110–120 (2010).
Huang, G. et al. Androgen deprivation therapy and cardiovascular risk in Chinese patients with nonmetastatic carcinoma of prostate. J Oncol. https://doi.org/10.1155/2014/529468 (2014).
Teoh, J. Y. et al. Risk of acute myocardial infarction after androgen- deprivation therapy for prostate cancer in a Chinese population. BJU Int. 116, 382–387 (2015).
Wang, L. H. et al. No Increased risk of coronary heart disease for patients receiving androgen deprivation therapy for prostate cancer in Chinese/Taiwanese men. Andrology. 4, 128–132 (2016).
Shim, M. et al. The use of gonadotropin-releasing hormone agonist does not affect the development of cardiovascular disease in prostate cancer patients: a nationwide population-based cohort study. J. Korean Med. Sci. 35, e47. https://doi.org/10.3346/jkms.2020.35.e47 (2020).
Seong, J. M. et al. Gonadotropin-releasing hormone agonists, anti-androgens and the risk of cardio-cerebrovascular disease in prostate cancer patients: an Asian population-based observational study. J. Cancer. 11, 4015–4022 (2011).
Durnin, J. V. & Womersley, J. Body fat assessed from total body density and its estimation from skinfold thickness: measurements on 481 men and women aged from 16 to 72 years. Br. J. Nutr. 32, 77–97 (1974).
Munakata, M. Brachial-ankle pulse wave velocity in the measurement of arterial stiffness: recent evidence and clinical applications. Curr. Hypertens. Rev. 10, 49–57 (2014).
Sugarwara, J. et al. Brachial-ankle pulse wave velocity: an index of central arterial stiffness. J. Hum. Hypertens. 19, 401–406 (2005).
D’Agostino, R. B. Sr. et al. General cardiovascular risk profile for use in primary care: the Framingham Heart Study. Circulation 117, 743–753 (2008).
Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive summary of the third report of the national cholesterol education program (NCEP) expert panel on detection, evaluation, and treatment of high Blood cholesterol in adults (adult treatment panel III). JAMA. 285, 2486–2497 (2001).
Levine, G. N. et al. American Heart Association Council on Clinical Cardiology and Council on Epidemiology and Prevention, the American Cancer Society, and the American Urological Association. Androgen-deprivation therapy in prostate cancer and cardiovascular risk: a science advisory from the American Heart Association, American Cancer Society, and American Urological Association: endorsed by the American Society for Radiation Oncology. Circulation 121, 833–840 (2010).
Carneiro, A. et al. Cardiovascular events associated with androgen deprivation therapy in patients with prostate cancer: a systematic review and meta-analysis. World J. Urol. 33, 1281–1289 (2015).
Zareba, P., Duivenvoorden, W., Leong, D. P. & Pinthus, J. H. Androgen deprivation therapy and cardiovascular disease: what is the linking mechanism?. Ther. Adv. Urol. 8, 118–129 (2016).
Dockery, F., Bulpitt, C. J., Agarwal, S., Donaldson, M. & Rajkumar, C. Testosterone suppression in men with prostate cancer leads to an increase in arterial stiffness and hyperinsulinaemia. Clin. Sci. 104, 195–201 (2003).
Dockery, F., Bulpitt, C. J., Agarwal, S., Vernon, C. & Rajkumar, C. Effect of androgen suppression compared with androgen receptor blockade on arterial stiffness in men with prostate cancer. J. Androl. 30, 410–415 (2009).
Oka, R. et al. Effect of androgen deprivation therapy on arterial stiffness and serum lipid profile changes in patients with prostate cancer: a prospective study of initial 6-month follow-up. Int. J. Clin. Oncol. 21, 389–396 (2016).
Albertsen, P. C. et al. Cardiovascular morbidity associated with gonadotropin releasing hormone agonists and an antagonist. Eur. Urol. 65, 565–573 (2014).
Ng, C. F. et al. The real-life evaluation of the effect of androgen deprivation therapy (ADT) in prostate cancer patients in Asia study: the initial report of the usage of ADT pattern in Asia. Int. J. Urol. 26(S2), 22 (2019).
Bhatia, N. et al. Cardiovascular effects of androgen deprivation therapy for the treatment of prostate cancer: ABCDE steps to reduce cardiovascular disease in patients with prostate cancer. Circulation 133, 537–541 (2016).
Shore, N. D. et al. Hero study investigators oral relugolix for androgen-deprivation therapy in advanced prostate cancer. N. Engl. J. Med. 382, 2187–2196 (2020).
Abida, W. et al. Analysis of the prevalence of microsatellite instability in prostate cancer and response to immune checkpoint blockade. JAMA Oncol. 5, 471–478 (2019).
Donato, M. D. et al. Nerve growth factor induces proliferation and aggressiveness in prostate cancer cells. Cancers. 11, 784 (2019).
Author information
Authors and Affiliations
Contributions
C.F.N., P.K.F.C., C.H.Y. and J.Y.C.T. were responsible for the clinical care and acquisition of data of patients. B.S.Y.L. was responsible for data acquisition and S.C.H.L. was responsible for statistical analysis. C.F.N. conceived of the study, and participated in its design and coordination and helped to draft the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ng, Cf., Chiu, P.K.F., Yee, Ch. et al. Effect of androgen deprivation therapy on cardiovascular function in Chinese patients with advanced prostate cancer: a prospective cohort study. Sci Rep 10, 18060 (2020). https://doi.org/10.1038/s41598-020-75139-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-020-75139-w
This article is cited by
-
Cardiovascular risk of gonadotropin-releasing hormone antagonist versus agonist in men with prostate cancer: an observational study in Taiwan
Prostate Cancer and Prostatic Diseases (2023)
-
Risks of metabolic diseases and androgen deprivation therapy for prostate cancer in a Chinese population: a prospective multi-centre cohort study
International Urology and Nephrology (2022)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
