
Key Points
-
Provides concise information on the functional anatomy of the edentulous lower impression.
-
The clinical and laboratory stages of the neutral zone impression are clearly and logically set out.
-
A list of competencies for the neutral zone impression are included.
Abstract
The neutral zone technique is an alternative approach for the construction of lower complete dentures. It is most effective for dentures where there is a highly atrophic ridge and a history of denture instability. The technique aims to construct a denture that is shaped by muscle function and is in harmony with the surrounding oral structures. The technique is by no means new but is a valuable one. This paper aims to provide clinicians with the knowledge to use the technique — a list of competencies is included.
Similar content being viewed by others


Introduction
The life expectancy of the British population is steadily increasing,1 which could lead to a rise in the number of complex complete denture cases. The treatment of these complex cases may need to move away from traditional denture construction. While the copy technique serves an excellent role, there is a need for an alternative approach when continued bone resorption has led to a progressively unsatisfactory denture or in cases where dentures have been lost. Dental implants may provide stabilisation of mandibular complete dentures for the atrophic mandible, however there may be situations when it is not possible to provide implants on the grounds of medical, surgical or costs factors. The neutral zone technique is an alternative approach for these complex cases. The technique is not new but is one that is valuable and yet not often practised.
The neutral zone has been defined as the area in the mouth where during function, the forces of the tongue pressing outwards are neutralised by the forces of the cheeks and lips pressing inwards.2 This definition is an over-simplification but serves to create a basic mental image of what a denture, constructed in the zone, is trying to achieve. It is impossible to construct a denture where the perfect, absolute equilibrium exists and no displacement occurs. The aim of the neutral zone is to construct a denture in muscle balance. That is a denture which is in harmony with its surroundings to provide optimum stability, retention and comfort.
The lower denture commonly presents the most difficulties with pain and looseness being the most common complaint.3 This is because the mandible atrophies at a greater rate than the maxilla and has less residual ridge for retention and support.4 The neutral zone technique is most effective for patients who have had numerous unstable, unretentive lower complete dentures. These patients usually have a highly atrophic mandible and there has been difficulty in positioning the teeth to produce a stable denture. The neutral zone approach has also been used for patients who have had a partial glossectomy, mandibular resections or motor nerve damage to the tongue — which have led to either atypical movement or an unfavourable denture bearing area.5
Background
Sir Wilfred Fish first described the influence of the polished surfaces on retention and stability in 1931.6 He also described how dentures should be constructed in the 'dead space', which later became know as the neutral zone.7 Since that time there have been a number of techniques described in the literature, which have attempted to provide a moulding of the neutral zone.8,9,10,11,12,13,14 These involved the use of a soft, mouldable material (usually wax or compound) being placed in the mouth with patients performing actions with their lips and tongues, the idea being to capture in greater detail the actions of the lips, cheeks and tongue. These actions determine the tooth position and the shape of the polished surfaces. The aim is to produce a denture moulded by muscle function that is in harmony with its surrounding structures and so enhancing stability and retention.
In the highly atrophic mandible muscular control over the denture is the main retentive and stabilising factor during function.10 A denture shaped by the neutral zone (NZ) technique will ensure that the muscular forces are working more effectively and in harmony.
The dentures will have other advantages:
-
Improved stability and retention
-
Posterior teeth will be correctly positioned allowing sufficient tongue space
-
Reduced food trapping adjacent to the molar teeth
-
Good aesthetics due to facial support.
Functional anatomy
Oral functions involve the unique interplay of the oral structures and muscles. Any interference with their movements, by a denture, would result in denture instability. The main displacing forces acting on a lower complete denture are the tongue, the lower lip and the modiolus. If the denture is placed in the zone that balances these displacing forces then the denture will be retained more effectively during function. If the denture strays outside the neutral zone it will be unstable during the activities of talking, swallowing and mastication. The NZ technique is used to minimise the displacing forces of the surrounding structures.
The major muscles involved are:
1. The buccinator
This muscle has a large role in determining the neutral zone. It extends anteriorly from the pterygomandibular raphe, from above the maxillary molars and below the mandibular molars to converge, with other muscles, at the modiolus. Some fibres pass through the modiolus to terminate in the orbicularis oris. The role of the buccinator during function is to position food on the occlusal surfaces of the teeth. This action is co-ordinated with the tongue to maintain the food in this position.
2. The modiolus
The modiolus is a strong knot of muscle that alters the position of the angle of the mouth. The main muscles that converge at the modiolus are the buccinator, orbicularis oris, zygomaticus major, and the levator and depressor anguli oris. Free movement of this knot of muscle must be ensured if the lower denture is to be stable. The modiolus determines the position of the premolar teeth and the shape of the polished surface in that region. This produces a narrowing of the denture so that the polished surface does not hinder the movements of the modiolus during function.
3. The orbicularis oris and the mentalis
In the highly atrophic, mandible positioning of the anterior teeth can be problematic. The movement and interaction of the lip and the tongue determines the position of the lower anterior teeth. If they are positioned too far labially the contraction of the lip will displace the denture posteriorly. The ridge can also resorb to such an extent that the mentalis muscle displaces the neutral zone lingually and anterior tooth position becomes even more vital for the success of the denture.15 The NZ technique provides the correct tooth position to allow for the balancing of these muscular forces during function.
4. The tongue
The tongue is a powerful group of muscles and it is in constant contact with the denture at rest and during function. During rest the two critical areas for the tongue are the anterior lingual flange and posterior to the molar teeth. The polished surfaces must be correctly shaped to allow for the tongue to lie unhindered in these areas. During function the position of the anterior and posterior teeth are critical. If the anterior or posterior teeth are set lingually the tongue will be cramped and the denture will be displaced during function. There must be sufficient tongue space to allow for movement. The occlusal plane is also important for stability. It should not be too high as to 'wall in' the tongue but should allow it to lie on the occlusal surface during rest.
Clinical technique
A timeline of the clinical technique is provided in Table 1.
Primary impressions and secondary impressions
The primary impressions are taken in a stock tray with a mucodisplacive material such as impression compound or a high viscosity alginate. The lower secondary impression is taken in a close-fitting special tray with a low viscosity mucostatic such as a zinc oxide eugenol (Fig. 1). The impression surface of the denture must be correctly extended to provide the maximum support from the underlying structures. The borders must be moulded to represent muscle activity, recording the functional depth and width of the sulcus.

Secondary impression with zinc oxide — eugenol
Jaw registration
The wax record rims are constructed on heat cured acrylic bases for increased stability, and assessed for extension, comfort and stability. Once the base plates have been assessed and modified, jaw registration can be carried out. The upper rim should be carved to provide support for the musculature labially and buccally. It is vitally important that the record rim is correctly trimmed to the full width of the sulcus; otherwise the correct width of the lower arch cannot be developed. After establishing the correct incisal level, occlusal planes and palatal contour — the lower rim is adjusted to the correct occlusal vertical dimension (OVD). The rims can now be registered in the retruded arc of closure. The laboratory can now articulate the rims on an average value articulator and construct the upper wax try-in and lower base plate.
Lower base plate construction
The wax is removed from the heat cured base plate and a superstructure is constructed. The superstructure has two functions: to provide even occlusal stops at the correct OVD and to provide support for the NZ impression material. Numerous designs have been proposed and the final decision is one of clinical preference. Favoured designs include self-cured pillars in the premolar regions with a short vertical fin between them or a light cured vertical fin along the centre of the base plate (Fig. 2). Whichever design is used it must be assessed in order that the structure does not deflect the cheeks, lip or tongue and that the desired OVD is maintained. The stops and fins can be modified with self-cured acrylic or greenstick tracing compound until the correct dimensions are produced.

Base plate with self-cure acrylic pillars and with a vertical fin
The neutral zone impression
The competency stages for the NZ impression are provided in Table 2.
Prior to taking the NZ impression the upper wax try-in is inserted. This will support the facial muscles and allow the tongue to be positioned on the teeth and palatal contours during function. The NZ impression requires a material that can be moulded by muscle activity. A high viscous mix of Viscogel (Dentsply, Weybridge, UK), which is a tissue conditioner, is advocated for the impression (Fig. 3). The mix is placed along the base plate and superstructure. The volume of the material should be controlled and kept to a minimum so that the sulci are not distorted. The material is mixed so that it can be manipulated by hand and positioned as an approximate rim on the lower base plate.

A tissue conditioner such as Viscogel is advocated for the technique
Before taking the impression the patient should be in a comfortable, upright position with the head supported. The plate is then rotated into the patient's mouth and they are asked to perform a series of actions designed to simulate physiological functioning. These actions will need to be rehearsed so that they are performed naturally and effectively.
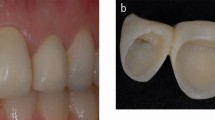
Suggested actions include asking the patient to: smile, grin, pout/purse lips, count from 60 to 70, talk aloud, pronounce the vowels, sip water, swallow, slightly protrude the tongue and lick the lips. These actions are repeated for 10 minutes until material has set. Figure 4a and 4b show a typical NZ impression with the characteristic shape produced by the oral musculature. The anterior labial surface shows proclination and the posterior part shows where the tongue has rested and moulded the rim.

An example of the neutral zone from the (a) lateral and (b) posterior view
Laboratory stage
A summary of the laboratory stages is provided in Table 3.
The technician will replace the NZ impression on the master model, cut locating grooves and place plaster or a silicone putty index around the impression (Fig. 5). The Viscogel impression is then removed from the base plate and the index replaced. The index will have preserved the space of the neutral zone. Wax can then be poured into the space giving an exact representation of the neutral zone. Teeth can then be set up exactly following the index. During the setting up of the teeth their position can be checked by putting the index together around the wax try-in (Figs 6a and 6b). The posterior teeth invariably have to be trimmed lingually in order that they are sufficiently narrow.

An example of a plaster index around the neutral zone impression

An example of a wax try-in with the plaster index (a) buccally and (b) lingually — note the locating grooves
Completion of the denture
Once the wax try-ins are deemed satisfactory the dentures may be processed and finished. Instructions must be given to the technician to polish the denture lightly so that the contours remain unaltered. On final insertion the dentures are fully inspected and a check record performed to eliminate any minor occlusal errors.16 The dentures should provide the patient with improved facial appearance, stability and retention during function — as they have been constructed in harmony with their surroundings.
Conclusion
The neutral zone is an alternative technique for the construction of lower complete dentures on highly atrophic ridges. It is especially useful in cases where dental implants are not possible and the copy technique would be inappropriate. The aim of the neutral zone is to construct a denture in muscle balance, as muscular control will be the main stabilising and retentive factor during function. The technique is relatively simple but there are increased chair time and laboratory costs.
References
Tinker A. Ageing in the United Kingdom — what does this mean for dentistry? Br Dent J 2003; 194: 369–372.
Beresin VE, Schiesser FJ. The neutral zone in complete and partial dentures p 15. C.V. Mosby Co., 1978.
Basker RM, Harrison A, Ralph JP. A survey of patients referred to restorative dentistry clinics. Br Dent J 1988; 164: 105–108.
Atwood DA. Post extraction changes in the adult mandible as illustrated by micrographs of midsagitall sections and serial cephalometric roentgenograms. J Prosthet Dent 1963; 13: 810–824.
Ohkubo C, Hanatani S, Hosoi T, Mizuno Y. Neutral zone approach for denture fabrication for a partial glossectomy patient: A clinical report. J Prosthet Dent 2000; 84: 390–393.
Fish EW. An analysis of the stabilising factors in full denture construction. Br Dent J 1931; 52: 559–570.
Fish EW. Using the muscles to stabilize the full lower denture. J Am Dent Assoc 1933; 20: 2163–2169.
Lott F, Levin B. Flange technique: an anatomic and physiologic approach to increased retention, function, comfort and appearance of dentures. J Prosthet Dent 1966; 16: 394–413.
Beresin VE, Schiesser FJ. The neutral zone In complete dentures. J Prosthet Dent 1976; 36: 356–367.
Fahmi FM. The position of the neutral zone in relation to the alveolar ridge. J Prosthet Dent 1992; 67: 805–809.
Fahmy FM, Kharat DU. A study of the importance of the neutral zone in complete dentures. J Prosthet Dent 1990; 64: 459–462.
Razek MKA, Abdalla F. Two-dimensional study of the neutral zone at different occlusal vertical heights. J Prosthet Dent 1981; 46: 484–489.
Heath R. A study of the morphology of the denture space. Dent Practit 1970; 21: 109–117.
Murphy WM. The neutral zone and the polished surfaces of full dentures. Dent Practit 1996; 16: 244–248.
Lammie GA. Aging changes in the complete lower dentures. J Prosthet Dent 1956; 36: 356–363.
Cabot L. The check record in NHS practice. Br Dent J 1992; 173: 105–106.
Author information
Authors and Affiliations
Corresponding author
Additional information
Refereed Paper
Rights and permissions
About this article
Cite this article
Gahan, M., Walmsley, A. The neutral zone impression revisited. Br Dent J 198, 269–272 (2005). https://doi.org/10.1038/sj.bdj.4812118
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.4812118
This article is cited by
-
Complicating factors in complete dentures: assessing case complexity
British Dental Journal (2021)
-
Patient Satisfaction With Complete Dentures Fabricated Using Two Neutral Zone Techniques: A Within-Subject Cross-Over Pilot Study
The Journal of Indian Prosthodontic Society (2014)
-
Improved stability
British Dental Journal (2005)
