
Abstract
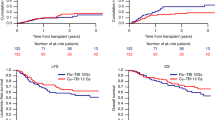
Allogeneic BMT for patients with acute myeloid leukemia (AML) is presently a reference therapy. The indications for this therapy mainly rely upon prognostic factors, and their importance is constantly reassessed. To examine the impact of time from diagnosis to transplant on survival and leukemia-free survival (LFS), we analyzed 109 patients from the database of the SFGM comprising patients who had all received an HLA-identical allogeneic BMT for a diagnosis of AML in first complete remission (CR1) between January 1987 and December 1992. All patients were conditioned with cyclophosphamide (CY) and total body irradiation (TBI) (CY-TBI), and methotrexate (MTX) + cyclosporin A (CsA) were used as graft-versus-host disease (GVHD) prophylaxis. Patient characteristics were: age = 33 ± 9, M/F = 64/45, white blood cell count (WBC) at diagnosis = 27 ± 42 × 109/l, FAB distribution: M1 and M2 = 55; M3 = 15, M4 and M5 = 33, M0, M6 and M7 = 6. Karyotyping was carried out for 64 patients: 32 had a normal karyotype, 16 had good prognosis abnormalities (t(8;21), t(15;17), inv 16) and 16 patients had other abnormalities. Eleven patients needed two courses of induction to achieve CR. Time between diagnosis and BMT was 120 (64–287) days. Forty-nine patients developed grade ⩾2 acute GVHD (actuarial probability = 46%). With a median follow-up of 50 months (27–100), the 5-year probabilities for transplant-related mortality (TRM), relapse, overall survival and LFS are respectively 25%, 26%, 59% and 55%. A multivariate analysis showed that survival is adversely influenced by three independent factors: time to transplant (>120 days vs ⩽120 days), acute GVHD (grade 2–4 vs grade 0–1) and age (>33 vs ⩽33). LFS is only influenced by the first two of these factors. The favorable impact of a shorter time from diagnosis to transplant should lead to performing the transplant as early as possible. Practically speaking, this means that when such therapy is chosen for a patient with CR1 AML, the search for an allogeneic donor should begin immediately and transplant be performed as soon as possible.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout
Similar content being viewed by others

Author information
Authors and Affiliations
Consortia
Rights and permissions
About this article
Cite this article
Jourdan, E., Maraninchi, D., Reiffers, J. et al. Early allogeneic transplantation favorably influences the outcome of adult patients suffering from acute myeloid leukemia. Bone Marrow Transplant 19, 875–881 (1997). https://doi.org/10.1038/sj.bmt.1700761
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1038/sj.bmt.1700761
Keywords
This article is cited by
-
Time to transplantation and pediatric acute myeloid leukemia outcomes
Bone Marrow Transplantation (2023)
-
A new time-dependent approach for assessment of the impact of invasive aspergillosis shows effect on short- but not on long-term survival of patients with AML or high-risk MDS
Bone Marrow Transplantation (2017)
-
Long-term disease-free survival after nonmyeloablative cyclophosphamide/fludarabine conditioning and related/unrelated allotransplantation for acute myeloid leukemia/myelodysplasia
Bone Marrow Transplantation (2010)
-
Early related or unrelated haematopoietic cell transplantation results in higher overall survival and leukaemia-free survival compared with conventional chemotherapy in high-risk acute myeloid leukaemia patients in first complete remission
Leukemia (2009)
-
Reduced intensity conditioning allows for up-front allogeneic hematopoietic stem cell transplantation after cytoreductive induction therapy in newly-diagnosed high-risk acute myeloid leukemia
Leukemia (2006)
