
Abstract
Compelling evidence demonstrates chromosome 8q24 as a prostate cancer susceptibility locus. Multiple variants within three adjacent regions at 8q24 have recently been identified to impact the risk of prostate cancer. Yet, the role of these variants in more advanced disease has not been rigorously assessed. To examine the relationship between 8q24 variants and advanced disease, we tested 10 previously associated 8q24 variants in a case–control study of advanced prostate cancer (N=1012). Of these ten 8q24 variants, six were associated with the risk of advanced prostate cancer (P=0.001–0.038). Three of these variants (rs10090154-region 1, rs16901979-region 2, and rs6983267-region 3), each variant residing in one of the three previously reported 8q24 regions, could account for our 8q24 effects on advanced disease. A meta-analysis across 10 studies including our results of four 8q24 variants (rs1442295 and DG8S737-region 1, rs16901979-region 2, and rs6983267-region 3) and prostate cancer risk demonstrated strong associations across a wide array of study designs and populations. Our findings provide the first confirmation that the three 8q24 regions independently influence the risk of prostate cancer and, in particular, advanced disease.
Similar content being viewed by others


Introduction
Multiple independent studies have demonstrated compelling evidence that genetic variation at chromosome 8q24 influences the risk of prostate cancer.1, 2, 3, 4, 5, 6, 7, 8, 9 The 8q24 risk locus was first identified by a genome-wide linkage study of Icelandic families and follow-up association studies, and two variants, DG8S737 and rs1447295, were most significantly associated with prostate cancer risk.1 Next, a genome-wide admixture scan of African Americans identified the same region at 8q24 to be associated with disease and determined that the variant(s) responsible for the admixture signal had yet to be identified.2 Three subsequent studies, including two genome-wide association studies of prostate cancer3, 4 and a fine-mapping study of the 8q24 locus,5 simultaneously reported multiple independent regions at 8q24 to impact the risk of prostate cancer. All three studies strongly replicated the original results (defined as region 1, 126.54–128.62 Mb), and identified two adjacent regions (defined as region 2, 128.14–128.28 Mb; and region 3, 128.47–128.54 Mb) that harbored risk variants for prostate cancer.3, 4, 5 A total of seven variants were reported to capture the risk profile of the three 8q24 regions, with these variants accounting for the original admixture signal.5
Some studies have reported 8q24 variants to be associated with aggressive prostate cancer8, 9 and increased tumor grade,1, 5, 8 although these findings are yet to be confirmed. Distinguishing the genetic variants that increase the risk of more advanced disease is important for improving regimens for screening, diagnosis, and the treatment of prostate cancer. Here, we present the results of a case–control study of ten 8q24 variants and advanced prostate cancer. In addition to studying more advanced disease, we provide the first simultaneous replication of an association between three independent regions at 8q24 and prostate cancer. Finally, we conducted a meta-analysis of published reports to summarize the genetic effects of the 8q24 variants on prostate cancer risk.
Methods
Our study was comprised of 506 advanced prostate cancer cases and 506 age-, ethnicity-, and medical institution-matched controls. Advanced prostate cancer cases were defined as having a Gleason score ≥7, TNM stage >T2c, or PSA >10 ng/ml. Among this case–control study, 82% percent were European Americans and 18% were African Americans. Study subjects were recruited from major medical institutions in Cleveland, OH and the Henry Ford Health System in Detroit, MI. Institutional review board approval was obtained from all participating institutions. A detailed description of this study population is given elsewhere.10, 11
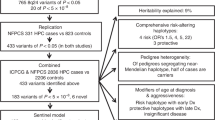
We selected the eight primary variants across the 8q24 locus that were previously associated with prostate cancer risk (128.1–128.6 Mb)3, 4, 5 and included two additional variants that were strongly associated with risk in region 2 (rs10505482 and rs1551512).5 Of the 10 variants, 3 were located in region 1 (rs10090154, rs1447295, and DG8S737), 5 were located in region 2 (rs10505482, rs16901979, rs1551512, rs6983561, and rs13254738), and 2 were located in region 3 (rs7000448 and rs6983267) (Figure 1). SNP genotyping was conducted by the 5′ nuclease Taqman allelic discrimination assay using predesigned primers/probes and read on a 7900HT Sequence Detection System (Applied Biosystems, Foster City, CA, USA). Microsatellite genotyping of the DG8S737 marker was performed using the primers specified by Admundadottir et al.1 The forward primer was synthesized with a 6-FAM end label. PCR products were separated on a 3730xl DNA Analyzer, and alleles assigned using GeneMapper software (Applied Biosystems). All variants were in Hardy–Weinberg equilibrium among controls for each ethnic group (P>0.05). The genotyping concordance rate was >99.9% for each variant.

Chromosome 8 and 8q24 locus. Vertical black lines depict the ten 8q24 variants genotyped in our case–control study of advanced prostate cancer. Horizontal black bars indicate region 1 (126.54–128.62 Mb), region 2 (128.14–128.28 Mb), and region 3 (128.47–128.54 Mb) of the 8q24 locus.
Odds ratios (ORs) and 95% confidence intervals (CIs) were estimated by unconditional logistic regression to examine the association between chromosome 8q24 variants and prostate cancer risk. We tested for heterogeneity of SNP effects across racial/ethnic groups by including an interaction term between SNP and racial/ethnic group in a multivariate model. Following the approach of Haiman et al,5 we conducted a stepwise logistic regression analysis to evaluate which combination of variants could account for our model of 8q24 effects on advanced prostate cancer risk (α criteria=0.10 for inclusion and exclusion). All OR estimates were adjusted for age and medical institution and also for racial/ethnic group in any analysis that combined groups. In addition, OR estimates in each 8q24 region were further adjusted for other regional effects by including variants from other 8q24 regions. For variants in region 1, we adjusted for regions 2 and 3 by including rs16901979-region 2 and rs6983267-region 3. For variants in region 2, we adjusted for region 1 and 3 by including rs10090154-region 1 and rs6983267-region 3. For variants in region 3, we adjusted for region 1 and 2 by including rs10090154-region 1 and rs16901979-region 2.
We conducted a meta-analysis of four 8q24 variants (rs1447295 and DG8S737-region 1, rs16901979-region 2, and rs6983267-region 3) and prostate cancer risk across 10 studies from May 2006 to April 20071, 2, 3, 4, 5, 6, 7, 8, 9 including our results (Supplementary Table 2). These four variants were chosen because they have the most data available for each of the three 8q24 regions. We also conducted a meta-analysis for advanced prostate cancer from available data for the rs14472951, 6, 7, 9 and DG8S737 variants,1, 5, 8, 9 including our results. Allele-specific ORs were abstracted from published studies. For studies that did not report allele-specific ORs, we estimated their effects based on the reported minor allele frequencies and number of cases and controls. Tests for homogeneity across study populations were conducted using a Pearson χ2 goodness-of-fit test (P>0.05 was considered homogeneous).
Results
The distribution of allele frequencies for the ten 8q24 variants among European Americans and African Americans in our study was similar to previous reports (Supplementary Table 1).3, 4, 5 Associations between the ten 8q24 variants and advanced prostate cancer risk are presented in Table 1. We found no evidence of heterogeneity in effects across racial/ethnic groups (P≥0.05). In an analysis unadjusted for other 8q24 regional effects, 6 of the 10 variants were significantly associated with prostate cancer: 2 of 3 variants in region 1 (rs10090154, rs1447295); 3 of the 5 variants in region 2 (rs16901979, rs1551512, rs6983561); and 1 of 2 variants in region 3 (rs6983267) (P=0.001–0.038) (Table 1). A stepwise logistic regression analysis identified three SNPs (rs10090154, rs16901979, and rs6983267) that could account for our 8q24 effects on advanced prostate cancer risk. Interestingly, these three SNPs reside in each of the three 8q24 regions previously associated with prostate cancer risk: rs10090154-region 1, rs16901979-region 2, and rs6983267-region 3. With further adjustment for the genetic effects from other 8q24 regions, these three SNPs remained significantly associated with advanced prostate cancer (Table 1). For rs10090154-region 1, the T allele in comparison to the C allele was significantly associated with an increased risk of advanced disease (OR=1.42; 95% CI: 1.07–1.87; P=0.014). For rs16901979-region 2, the A allele in comparison to the C allele was similarly significantly associated with advanced disease (OR=1.55; 95 CI: 1.12–2.14; P=0.009). For rs6983267-region 3, the G allele in comparison to the T allele was significantly associated with advanced prostate cancer (OR=1.35; 95% CI: 1.12–1.63; P=0.002).
Associations between 8q24 variants and prostate cancer stratified by racial/ethnic group are presented in Table 2. Among European Americans, six of the ten 8q24 variants were significantly associated with advanced disease (rs10090154, rs1447295, rs6983267, rs16901979, rs1551512, rs6983561) and similar results were observed after adjusting for the genetic effects of other 8q24 regions. Among African Americans, patterns of associations were consistent with those observed among European Americans; and no statistically significant associations were observed after adjusting for other 8q24 regions. This is likely due to our limited power to detect modest effects in African American-specific analyses.
We conducted an analysis of covariance among cases to examine whether the ten 8q24 variants were associated with age at diagnosis of prostate cancer with adjustment for race and institution. None of the variants were associated with age at diagnosis (Ps>0.20). In addition, we tested for heterogeneity in 8q24 effects across age groups (<66 vs ≥66 years), and found evidence of heterogeneity (Ps≥0.35).
Meta-analyses
Meta-analyses of four 8q24 variants (rs1447295 and DG8S737-region 1, rs16901979-region 2, and rs6983267-region 3) are presented in Figure 2a–d. The total sample size ranged from 30 939 (15 625 cases/15 314 controls) across nine studies for rs1447295 to 17 447 (7808 cases/9639 controls) across three studies for rs16901979. All four 8q24 variants were significantly associated with prostate cancer risk in all groups combined and as well in stratified analysis of populations of European and African ancestry. For rs1447295-region 1, the allele-specific meta-analysis OR and 95% CI for the A allele vs the C allele were 1.42 and 1.40–1.44 for all prostate cancer (Figure 2a), and were 1.48 and 1.45–1.50 for advanced disease (data not shown). For DG8S737-8 vs all other alleles-region 1, the allele-specific meta-analysis OR and 95% CI were 1.54 and 1.50–1.58 for all prostate cancer (Figure 2b), and were 1.74 and 1.72–1.77 for advanced disease (data not shown). For rs16901979-region 2, the meta-analysis OR and 95% CI for the A allele vs the C allele were 1.52 and 1.49–1.54 (Figure 2c). For rs6983267-region 3, the meta-analysis OR and 95% CI for the G allele vs the T allele were 1.25 and 1.24–1.26 (Figure 2d). There was no evidence of heterogeneity across the different study panels for each of the four 8q24 variants (Ps>0.268).




Meta-analysis of 8q24 variants and prostate cancer. *Allele-specific odds ratio estimated by reported allele frequencies and case–control study numbers. †Wang et al9 sporadic prostate cancer results. (a) rs1447295-region 1 (A allele vs C allele) and prostate cancer across 24 study panels from nine studies. (b) DG8S737-region 1 (−8 allele vs all other alleles) and prostate cancer across 13 study panels from five studies. (c) rs16901979-region 2 (A allele vs C allele) and prostate cancer across 12 study panels from three studies. (d) rs6983267-region 3 (G allele vs T allele) and prostate cancer across 12 study panels from three studies.
Discussion
In our unique study population of men with advanced disease, 84% with a Gleason score ≥7 and 35% with tumor stage ≥T2, we found that genetic variants in the three regions across 8q24 independently predicted the risk of advanced prostate cancer. It is clinically important to identify men predisposed to such advanced forms of disease as these cancers have increased co-morbidities and mortalities.
This is also the first independent replication that the three regions at 8q24 are individually associated with prostate cancer risk. In previous work, region 1 (126.54–128.62 Mb) was identified by the original linkage and admixture studies;1 however, initial associations within this region could not fully account for the admixture signal among African Americans.2 Region 2 (128.14–128.28 Mb), approximately 350 kb upstream of region 1, identified by Gudmundsson et al3 and Haiman et al,5 harbored associations that could more fully account for the original admixture signal, displaying higher frequency risk alleles among African Americans than among individuals of European ancestry.3, 5 Region 3 (128.47–128.54 Mb), closely positioned between Region 1 and Region 2, was defined by a recombination hot-spot among European Americans by Yeager et al.4 Our study confirms the effects of these three adjacent 8q24 regions independently influencing advanced prostate cancer susceptibility. We identified three variants (rs10090154-region 1, rs16901979-region 2, and rs6983267-region 3) from each of the three regions that could account for our 8q24 effects on advanced prostate cancer. Having examined only 10 of the previously associated 8q24 variants, a limitation of our study is that we have not fully evaluated other correlated variants within each region that may also influence the risk of advanced disease.
Considering our results in the light of previous studies, an exhaustive fine-mapping study by Haiman et al5 followed up their initial admixture results2 by testing 2973 SNPs spanning over 6000 kb (1 SNP per 2.2 kb) in a multiethnic study of prostate cancer cases and controls. Seven variants (rs13254738, rs6983561, Broad11934905, rs6983267, rs7000448, DG8S737-8, rs10090154) were identified that captured the risk profile of the 8q24 locus. Of the seven variants, we examined all except the African American-specific SNP, Broad11934905, due to our limited power to assess African-American-specific effects. In our study, three of these variants (rs6983561, rs6983267, rs10090154) were significantly associated with increased prostate cancer risk; the remaining three variants (rs13254738, rs7000448, DG8S737-8) were not significantly associated with the disease. These findings, however, are consistent with the results of Haiman et al,5 as these variants were not significantly associated with risk among European Americans, yet they were significantly associated with prostate cancer among all five/racial ethnic groups combined The two genome-wide association studies of prostate cancer by Gudmundsson et al3 and Yeager et al4 highlighted three variants (rs69019793 and rs69832674 and rs78376884) that influence prostate cancer risk in addition to the originally identified rs1447295 variant. For rs6901979, we observed a similar increased risk of disease among European Americans as reported by Gudmundsson et al.3 For rs6983267, we observed a consistent increased risk of prostate cancer as reported by Yeager et al.4 We did not test rs7837688 because of its strong correlation (r2=0.814) with rs1447295. For rs1447295, consistent genetic effects were observed as previously reported by multiple groups.1, 2, 3, 4, 6, 7, 8
Our meta-analysis of four 8q24 variants in up to 15 625 prostate cancer cases and 15 314 controls demonstrated strong associations with prostate cancer risk across a wide array of study designs and populations. In addition, all four variants (rs1447295, DG8S737-8, rs16901979, and rs6983267) showed associations that remained statistically significant with a simple Bonferroni correction for four independent hypothesis tests (P<0.0125). In summary, allele-specific effects for these 8q24 variants ranged from a 1.25- to 1.53-fold increased risk of prostate cancer; we estimated the joint population attributable fractions for these variants, suggesting that if the risk alleles were absent in the population, a reduction of risk of 15 and 41% among individuals of European and African ancestry, respectively, would be expected.
The mechanism by which 8q24 variants affect prostate cancer susceptibility is currently not known. None of the variants reside within known genes, of which there are few across the regions of 8q24. Thus, resolving the underlying genetic effects will require innovative studies to determine whether these variants affect function of neighboring genes or genes on other chromosomes (trans-regulatory elements). In the light of our association with advanced disease, future studies should also investigate these variants in relation to the progression of prostate cancer. Gaining such knowledge will shed novel insight into our understanding of the biology of prostate cancer and disease susceptibility. In turn, a better understanding of disease etiology can lead to improved outcomes through a more personalized approach to treatment.
In conclusion, our study provides further strong evidence that multiple regions across chromosome 8q24 impact the risk of advanced prostate cancer.
References
Amundadottir LT, Sulem P, Gudmundsson J et al: A common variant associated with prostate cancer in European and African populations. Nat Genet 2006; 38: 652–658.
Freedman ML, Haiman CA, Patterson N et al: Admixture mapping identifies 8q24 as a prostate cancer risk locus in African–American men. Proc Natl Acad Sci USA 2006; 103: 14068–14073.
Gudmundsson J, Sulem P, Manolescu A et al: Genome-wide association study identifies a second prostate cancer susceptibility variant at 8q24. Nat Genet 2007; 39: 631–637.
Yeager M, Orr N, Hayes RB et al: Genome-wide association study of prostate cancer identifies a second risk locus at 8q24. Nat Genet 2007; 39: 645–649.
Haiman CA, Patterson N, Freedman ML et al: Multiple regions within 8q24 independently affect risk for prostate cancer. Nat Genet 2007; 39: 638–644.
Severi G, Hayes VM, Padilla EJ et al: The common variant rs1447295 on chromosome 8q24 and prostate cancer risk: results from an Australian population-based case–control study. Cancer Epidemiol Biomarkers Prev 2007; 16: 610–612.
Schumacher FR, Feigelson HS, Cox DG et al: A common 8q24 variant in prostate and breast cancer from a large nested case–control study. Cancer Res 2007; 67: 2951–2956.
Suuriniemi M, Agalliu I, Schaid DJ et al: Confirmation of a positive association between prostate cancer risk and a locus at chromosome 8q24. Cancer Epidemiol Biomarkers Prev 2007; 16: 809–814.
Wang L, McDonnell SK, Slusser JP et al: Two common chromosome 8q24 variants are associated with increased risk for prostate cancer. Cancer Res 2007; 67: 2944–2950.
Liu X, Plummer SJ, Nock NL, Casey G, Witte JS : Nonsteroidal antiinflammatory drugs and decreased risk of advanced prostate cancer: modification by lymphotoxin alpha. Am J Epidemiol 2006; 164: 984–989.
Cheng I, Plummer SJ, Casey G, Witte JS : Toll-like receptor 4 genetic variation and advanced prostate cancer risk. Cancer Epidemiol Biomarkers Prev 2007; 16: 352–355.
Acknowledgements
We are indebted to the participants of this study, who have contributed to a better understanding of the genetic contributions to prostate cancer susceptibility. IC is supported by National Institutes of Health R25T training grant (CA112355). This work was supported by the National Institutes of Health grants (CA88164, CA94211, and CA98683).
Author information
Authors and Affiliations
Corresponding author
Additional information
Supplementary Information accompanies the paper on European Journal of Human Genetics website (http://www.nature.com/ejhg)
Supplementary information
Rights and permissions
About this article
Cite this article
Cheng, I., Plummer, S., Jorgenson, E. et al. 8q24 and prostate cancer: association with advanced disease and meta-analysis. Eur J Hum Genet 16, 496–505 (2008). https://doi.org/10.1038/sj.ejhg.5201959
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ejhg.5201959
Keywords
This article is cited by
-
The PENGUIN approach to reconstruct protein interactions at enhancer-promoter regions and its application to prostate cancer
Nature Communications (2023)
-
PRState: Incorporating genetic ancestry in prostate cancer risk scores for men of African ancestry
BMC Cancer (2022)
-
Association of three 8q24 polymorphisms with prostate cancer susceptibility: evidence from a meta-analysis with 50,854 subjects
Scientific Reports (2015)
-
Genetic heterogeneity in Finnish hereditary prostate cancer using ordered subset analysis
European Journal of Human Genetics (2013)
-
Aspirin but not ibuprofen use is associated with reduced risk of prostate cancer: a PLCO Study
British Journal of Cancer (2012)
