
Abstract
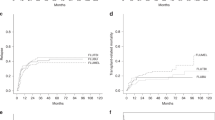
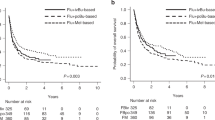
This was an Australasian Bone Marrow Transplant Recipient Registry (ABMTRR)-based retrospective study assessing the outcome of Fludarabine Melphalan (FluMel) reduced-intensity conditioning between 1998 and 2008. Median follow-up was 3.4 years. There were 344 patients with a median age of 54 years (18–68). In all, 234 patients had myeloid malignancies, with AML (n=166) being the commonest indication. There were 110 lymphoid patients with non-hodgkins lymphoma (NHL) (n=64) the main indication. TRM at day 100 was 14% with no significant difference between the groups. OS and disease-free survival (DFS) were similar between myeloid and lymphoid patients (57 and 50% at 3 years, respectively). There was no difference in cumulative incidence of relapse or GVHD between groups. Multivariate analysis revealed four significant adverse risk factors for DFS: donor other than HLA-identical sibling donor, not in remission at transplant, previous autologous transplant and recipient CMV positive. Chronic GVHD was associated with improved DFS in multivariate analysis predominantly due to a marked reduction in relapse (HR:0.44, P=0.003). This study confirms that FluMel provides durable and equivalent remissions in both myeloid and lymphoid malignancies. Disease stage and chronic GVHD remain important determinants of outcome for FluMel allografting.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout


Similar content being viewed by others

References
Copelan EA . Hematopoietic stem-cell transplantation. N Engl J Med 2006; 354: 1813–1826.
Khouri IF, Keating M, Korbling M, Przepiorka D, Anderlini P, O'Brien S et al. Transplant-lite: induction of graft-versus-malignancy using fludarabine-based nonablative chemotherapy and allogeneic blood progenitor-cell transplantation as treatment for lymphoid malignancies. J Clin Oncol 1998; 16: 2817–2824.
Aoudjhane M, Labopin M, Gorin NC, Shimoni A, Ruutu T, Kolb HJ et al. Comparative outcome of reduced intensity and myeloablative conditioning regimen in HLA identical sibling allogeneic haematopoietic stem cell transplantation for patients older than 50 years of age with acute myeloblastic leukaemia: a retrospective survey from the Acute Leukemia Working Party (ALWP) of the European group for Blood and Marrow Transplantation (EBMT). Leukemia 2005; 19: 2304–2312.
Dreger P, Brand R, Milligan D, Corradini P, Finke J, Lambertenghi Deliliers G et al. Reduced-intensity conditioning lowers treatment-related mortality of allogeneic stem cell transplantation for chronic lymphocytic leukemia: a population-matched analysis. Leukemia 2005; 19: 1029–1033.
Unrelated Donor Haematopoietic Stem Cell Transplants in Australia 2001–2010 A report from the Australasian Bone Marrow Transplant Recipients Registry November 2011.
Nivison-Smith I, Bradstock KF, Dodds AJ, Hawkins PA, Ma DD, Moore JJ et al. Hematopoietic stem cell transplantation in Australia and New Zealand, 1992–2004. Biol Blood Marrow Transplant 2007; 13: 905–912.
Ljungman P, Urbano-Ispizua A, Cavazzana-Calvo M, Demirer T, Dini G, Einsele H et al. Allogeneic and autologous transplantation for haematological diseases, solid tumours and immune disorders: definitions and current practice in Europe. Bone Marrow Transplant 2006; 37: 439–449.
Giralt S, Thall PF, Khouri I, Wang X, Braunschweig I, Ippolitti C et al. Melphalan and purine analog-containing preparative regimens: reduced-intensity conditioning for patients with hematologic malignancies undergoing allogeneic progenitor cell transplantation. Blood 2001; 97: 631–637.
Giralt S, Ballen K, Rizzo D, Bacigalupo A, Horowitz M, Pasquini M et al. Reduced-intensity conditioning regimen workshop: defining the dose spectrum. Report of a workshop convened by the center for international blood and marrow transplant research. Biol Blood Marrow Transplant 2009; 15: 367–369.
Przepiorka D, Weisdorf D, Martin P, Klingemann HG, Beatty P, Hows J et al. 1994, Consensus Conference on Acute GVHD Grading. Bone Marrow Transplant 1995; 15: 825–828.
Shulman HM, Sullivan KM, Weiden PL, McDonald GB, Striker GE, Sale GE et al. Chronic graft-versus-host syndrome in man. A long-term clinicopathologic study of 20 Seattle patients. Am J Med 1980; 69: 204–217.
Grimwade D, Walker H, Harrison G, Oliver F, Chatters S, Harrison CJ et al. The predictive value of hierarchical cytogenetic classification in older adults with acute myeloid leukemia (AML): analysis of 1065 patients entered into the United Kingdom Medical Research Council AML11 trial. Blood 2001; 98: 1312–1320.
Gooley TA, Leisenring W, Crowley J, Storer BE . Estimation of failure probabilities in the presence of competing risks: new representations of old estimators. Stat Med 1999; 18: 695–706.
Sarosy G, Leyland-Jones B, Soochan P, Cheson BD . The systemic administration of intravenous melphalan. J Clin Oncol 1988; 6: 1768–1782.
Delgado J, Thomson K, Russell N, Ewing J, Stewart W, Cook G et al. Results of alemtuzumab-based reduced-intensity allogeneic transplantation for chronic lymphocytic leukemia: a British Society of Blood and Marrow Transplantation Study. Blood 2006; 107: 1724–1730.
de Lima M, Champlin RE, Thall PF, Wang X, Martin TG 3rd, Cook JD et al. Phase I/II study of gemtuzumab ozogamicin added to fludarabine, melphalan and allogeneic hematopoietic stem cell transplantation for high-risk CD33 positive myeloid leukemias and myelodysplastic syndrome. Leukemia 2008; 22: 258–264.
Craddock C, Nagra S, Peniket A, Brookes C, Buckley L, Nikolousis E et al. Factors predicting long-term survival after T-cell depleted reduced intensity allogeneic stem cell transplantation for acute myeloid leukemia. Haematologica 2010; 95: 989–995.
Oran B, Giralt S, Saliba R, Hosing C, Popat U, Khouri I et al. Allogeneic hematopoietic stem cell transplantation for the treatment of high-risk acute myelogenous leukemia and myelodysplastic syndrome using reduced-intensity conditioning with fludarabine and melphalan. Biol Blood Marrow Transplant 2007; 13: 454–462.
Moore J, Nivison-Smith I, Goh K, Ma D, Bradstock K, Szer J et al. Equivalent survival for sibling and unrelated donor allogeneic stem cell transplantation for acute myelogenous leukemia. Biol Blood Marrow Transplant 2007; 13: 601–607.
Luger SM, Ringden O, Zhang MJ, Perez WS, Bishop MR, Bornhauser M et al. Similar outcomes using myeloablative vs reduced-intensity allogeneic transplant preparative regimens for AML or MDS. Bone Marrow Transplant 2012; 47: 203–211.
Delgado J, Pillai S, Benjamin R, Caballero D, Martino R, Nathwani A et al. The effect of in vivo T cell depletion with alemtuzumab on reduced-intensity allogeneic hematopoietic cell transplantation for chronic lymphocytic leukemia. Biol Blood Marrow Transplant 2008; 14: 1288–1297.
Morris E, Thomson K, Craddock C, Mahendra P, Milligan D, Cook G et al. Outcomes after alemtuzumab-containing reduced-intensity allogeneic transplantation regimen for relapsed and refractory non-Hodgkin lymphoma. Blood 2004; 104: 3865–3871.
Thomson KJ, Morris EC, Milligan D, Parker AN, Hunter AE, Cook G et al. T-cell-depleted reduced-intensity transplantation followed by donor leukocyte infusions to promote graft-versus-lymphoma activity results in excellent long-term survival in patients with multiply relapsed follicular lymphoma. J Clin Oncol 2010; 28: 3695–3700.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
Andrew Spencer has received research support from Celgene, Janssen and Novartis. The remaining authors declare no conflict of interest.
Additional information
This study has been presented in part at the HAA/APBMT meeting in Sydney, Australia in October 2011 and ASH, San Diego, USA, December 2011.
Author Contributions
AB, IN-S and JM designed the study, compiled the data, analysed the data, and wrote and approved the final manuscript. ESP, GK, AK, DR, BG, MH, SP, AS, KF, PC, LB, RD and RS compiled the data, and wrote and approved the final manuscript.
Rights and permissions
About this article
Cite this article
Bryant, A., Nivison-Smith, I., Pillai, E. et al. Fludarabine Melphalan reduced-intensity conditioning allotransplanation provides similar disease control in lymphoid and myeloid malignancies: analysis of 344 patients. Bone Marrow Transplant 49, 17–23 (2014). https://doi.org/10.1038/bmt.2013.142
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/bmt.2013.142
Keywords
This article is cited by
-
Prognostic impact of the AML ELN2022 risk classification in patients undergoing allogeneic stem cell transplantation
Blood Cancer Journal (2022)
-
Retrospective comparison of hematopoietic stem cell transplantation following reduced-intensity conditioning with fludarabine/low-dose melphalan plus 4 Gy TBI versus fludarabine/ busulfan plus 4 Gy TBI
International Journal of Hematology (2022)
-
Oral fludarabine is an effective and convenient alternative to intravenous fludarabine in fludarabine melphalan based reduced intensity conditioning regimens
Bone Marrow Transplantation (2020)
-
Curative potential of fludarabine, melphalan, and non-myeloablative dosage of busulfan in elderly patients with myeloid malignancy
International Journal of Hematology (2020)
-
A novel reduced intensity conditioning regimen for patients with high-risk hematological malignancies undergoing allogeneic stem cell transplantation
Bone Marrow Transplantation (2016)
