
Abstract
Purpose
Comparative evaluation of ‘flap on’ and ‘flap off’ techniques of Epi-LASIK in low-to-moderate myopia.
Methods
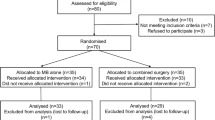
Sixteen eyes of eight consecutive patients with myopia ⩽6 D were selected for this prospective, randomized, comparative, interventional case series. Epi-LASIK surgery was performed in all eyes. In one eye of each patient, the epithelial flap was retained after excimer laser ablation (flap on). In the fellow eye, the epithelial flap was discarded (flap off) after ablation. Uncorrected visual acuity (UCVA), best spectacle-corrected visual acuity (BSCVA), spherical equivalent (SEQ), postoperative pain score, time to epithelization, and corneal haze were recorded on postoperative visits.
Results
The mean preoperative SEQ in the two groups was −3.61±1.32 D (flap on) and −3.49±1.86 D (flap off; P=0.752). The mean follow-up period was 8.5±4.9 months. The mean pain score was comparable on all postoperative days except the second postoperative day when the group with flap off had a lesser mean pain score (P=0.053).
Time for epithelial healing was 3.63±0.52 days in cases with flap off and 4.13±0.64 days in cases with flap on (P=0.113). Eyes with flap off had a better UCVA on the first postoperative day (0.19±0.11 logMAR) compared with eyes with flap on (0.41±0.28logMAR; P=0.032). There was no significant difference in UCVA, BSCVA, SEQ, contrast sensitivity, corneal haze, and higher order aberrations at any other postoperative visit.
Conclusions
There is no difference between flap on and flap off techniques of Epi-LASIK with regards to overall outcome of surgery.
Similar content being viewed by others


Introduction
There has been a renewed interest in surface ablation modalities like Epi-LASIK over the past few years to avoid LASIK-related complications, such as ectasia and dry eyes, and flap-related complications. Epi-LASIK aims to combine the advantages of both LASIK and PRK to provide a reproducible and predictable refractive surgical procedure. Though Epi-LASIK is a major advancement over PRK, some issues require further study. An area of ongoing debate is the role and use of the epithelial flap in Epi-LASIK surgery. Some surgeons have suggested that the epithelial flap should be removed after excimer laser ablation to improve the rate of visual recovery and postoperative discomfort. Other surgeons have suggested that the flap should be retained to reduce the development of corneal haze and postoperative pain.1, 2 This prospective randomized study was conducted to evaluate the effect of the epithelial flap on visual recovery, epithelial healing, and postoperative discomfort after Epi-LASIK surgery.
Materials and methods
Sixteen eyes of eight patients who presented to the cornea and refractive surgery services of our hospital for surgical refractive correction were enrolled for the study. All these were consecutive patients who had myopia of less than 6 D in both the eyes and had no contraindications for excimer laser refractive surgery. The study had the approval of the institutional review board and informed consent was obtained from the subjects.
Surgical technique, Epi-LASIK, was performed under topical anaesthesia using proparacaine 0.5% eye drops instilled twice over a period of 10 min. Epikeratome (Epi-K, Moria SA, Antony, France) was used for the creation of epithelial flap. Excimer laser ablation was performed using Bausch and Lomb Technolas 217Z (GmBh, Dornach, Germany). The epithelial flap was reposited back in one randomly selected eye of each patient and discarded in the contralateral eye. Bandage contact lens was put in both the eyes at the end of surgery.
Postoperative treatment included 0.5% of moxifloxacin hydrochloride ophthalmic solution three times a day, 1% of prednisolone acetate eye drop four times a day, and preservative-free artificial tears four times a day. The antibiotic was continued for a week and the steroids were gradually tapered over 1 month. The patients were followed up daily for 1 week or till complete healing of epithelial defect whichever was later. Further follow-up visits were planned at 1, 3, and 6 months and 1 year postoperatively.
On each visit during the first week, the parameters recorded were uncorrected visual acuity (UCVA) using logMAR ETDRS chart, size of epithelial defect, and pain score. The visual acuity was tested by a single unmasked observer. The patients were masked as to the nature of surgery in each eye. The pain score was subjectively graded by the patient according to the following questionnaire (pain score—grade 0=no discomfort or pain, grade 1=mild discomfort, grade 2=moderate burning pain, grade 3=burning pain requiring medication, and grade 4=severe constant or sharp pain).
After the first week postoperatively, the parameters recorded on each visit were UCVA, best spectacle-corrected visual acuity (BSCVA), refraction, videokeratography (VKG), and corneal haze. The corneal haze was graded on slit-lamp examination as grade 0=no haze, grade 1=trace seen only with broad beam illumination, grade 2=haze seen with direct illumination, grade 3=moderate haze slightly obscuring iris details, and grade 4=marked haze.3
Statistical analysis was performed using SPSS 10.0. Nonparametric tests (Mann–Whitney U-test) were used due to the small sample size.
Results
The mean age of the patients was 20.25±1.44 years (Table 1). The mean preoperative SEQ in the eyes group with flap on was −3.61±1.32 D (range: −1.5 to −5.88 D) and in the group with flap off was −3.49±1.86 D (range: −1.37 to −6 D) (P=0.752; Table 1). There were no intraoperative complications in any of the patients. Two patients were lost to follow-up after 1 month and 1 patient after 6 months. The remaining six patients completed a follow-up of 1 year.
On the first postoperative day, the mean pain score were similar in the two groups (P=0.698; Table 2). On the second postoperative day, the group with flap off had a lesser mean pain score compared with group with flap on (P=0.053; Table 2). The mean pain score gradually decreased to zero by postoperative day 4 in the group with flap off and day 5 in the group with flap on.
All the eyes had complete healing of epithelial defect within 5 days (range: 3–5 days). The mean epithelial healing time was slightly better in eyes with flap off (3.63±0.52 days compared to 4.13±0.64 days), but the difference was not statistically significant (P=0.113).
Comparison of visual acuity during the early postoperative period revealed a significantly better UCVA on the first postoperative day in eyes with flap off (0.19±0.11 logMAR (Snellen equivalent ∼20/32)) compared with eyes with flap on (0.41±0.28logMAR (Snellen equivalent ∼20/50; P=0.032; Table 3). After the first postoperative day, there was no significant difference in UCVA or BSCVA between the two groups till the end of the first week (Table 3). By the end of the first postoperative week, all eyes had attained the BSCVA of >20/40 and 81.25% (13 out of 16 eyes) had attained the BSCVA of ⩾20/20.
Comparison of the groups at the last visit revealed no significant differences between the flap on and the flap off groups for UCVA, BSCVA, and SEQ refractive errors, keratometry, contrast sensitivity, corneal haze, and higher order aberrations (Table 4). Two eyes in each group had central corneal haze of grade 2 at the last visit. Five eyes (three in flap off and two in flap on) had central corneal haze of grade 1 at the last visit.
Contrast sensitivity at low spatial frequencies of 1.5 (P=0.027) and 3 cpd (P=0.041) showed a statistically significant increase postoperatively compared with preoperative levels. Contrast sensitivity at higher spatial frequencies (6, 12 and 18 cpd) did not reveal significant change from preoperative levels.
Discussion
Newer surface ablation modalities, such as LASEK and Epi-LASIK, have been devised to prevent the side effects of PRK, such as postoperative pain, delayed visual recovery, and corneal haze.1, 2, 4, 5, 6 Histological analysis of the epithelial sheets obtained with epikeratome also shows viable epithelial cells with an intact basement membrane allowing it to be used as a viable bandage contact lens postoperatively.7, 8, 9, 10
It has been proposed that the presence of the flap reduces postoperative pain and development of corneal haze, though this has not been confirmed in clinical studies.11, 12 It has also been debated that the presence of epithelial cells in the flap may actually hinder the migratory phase of epithelial regeneration and delay the visual recovery. Discarding the epithelial flap is an alternative that has been suggested to hasten the rate of visual recovery. This prospective randomized study was designed to evaluate the role of epithelial flap in the rate of visual recovery, epithelial healing, severity of postoperative pain, and development of corneal haze in patients with low-to-moderate myopia.
The results indicate that the presence of epithelial flap does not significantly improve the postoperative course after Epi-LASIK surgery. On the first postoperative day, the eyes with flap on showed a poorer visual acuity compared with the eyes with flap off. This difference may be due to the presence of oedematous hazy epithelial sheet in the group with flap on compared with eyes without the flap. With regeneration of healthy epithelial cells in both the groups, this difference in visual acuity disappeared by the second postoperative day.
The presence of epithelial flap did not significantly improve the rate of epithelial healing. All the patients had complete healing by 3–5 days after surgery. The group with flap off showed a trend towards faster epithelial healing with mean time to complete epithelization of 3.63±0.52 days with flap off compared with 4.13±0.64 days with flap ‘on,’ though the difference was not statistically significant (P=0.113).
The subjective scoring of postoperative pain also showed a trend towards lesser pain in the flap off group compared with flap on. The flap off group had a lesser pain score on postoperative day 2 with borderline statistical significance. The mean score also reached zero a day earlier in eyes with flap off compared with flap on.
The development of corneal haze was also not affected by the presence of the flap. Nine of the sixteen eyes developed corneal haze, which was visually non-significant and similarly distributed between the two groups. The rate of corneal haze of 56% obtained in our study is higher than that reported by other authors. Katsanevaki et al4 reported no ‘significant’ corneal haze in any of their patient, whereas Gamaly et al5 reported a rate of 29% in their study. Though none of our patients developed visually significant corneal haze and all of them had only low-to-moderate myopia, it would be worthwhile to consider the use of prophylactic mitomycin-C in all patients undergoing surface ablation including Epi-LASIK. In the context of mitomycin-C, the use of flap on technique can have technical difficulties and this aspect requires further study.
Wang et al13 in a similar study have compared the flap off and flap on techniques in patients with moderate-to-high myopia. Similar to our results, they have also noted a better UCVA in the early postoperative period in the flap ‘off’ group along with a quicker epithelization. They also noted lower incidence of corneal haze in the flap ‘off’ group. The authors did not find any significant difference in postoperative pain intensity between the two groups. The study by Wang et al13 and our study both indicate the lack of any significant benefit of retaining the epithelial flap after Epi-LASIK.
Though our study was limited by its small sample size, it can be concluded that the presence of the epithelial flap does not significantly improve the epithelial healing and visual and refractive outcomes after Epi-LASIK in patients with low-to-moderate myopia. It would be worthwhile to undertake a study to compare flap off technique of Epi-LASIK with PRK. This will allow us to evaluate any benefits of epikeratome-assisted creation of epithelial flap compared with the mechanical or alcohol-assisted removal in PRK.
References
Pallikaris IG, Katsanevaki VJ, Kalyvianaki MI, Naoumidi II . Advances in subepithelial excimer refractive surgery techniques: Epi-LASIK. Curr Opin Ophthalmol 2003; 14: 207–212.
Matsumoto JC, Chu YS . Epi-LASIK update: overview of techniques and patient management. Int Ophthalmol Clin 2006; 46: 105–115.
Anderson NJ, Beran RF, Schneider TL . Epi-LASEK for the correction of myopia and myopic astigmatism. J Cataract Refract Surg 2002; 28: 1343–1347.
Katsanevaki VJ, Kalyvianaki MI, Kavroulaki DS, Pallikaris IG . One-year clinical results after epi-LASIK for myopia. Ophthalmology 2007; 114: 1111–1117.
Gamaly TO, El Danasoury A, El Maghraby A . A prospective, randomized, contralateral eye comparison of epithelial laser in situ keratomileusis and photorefractive keratectomy in eyes prone to haze. J Refract Surg 2007; 23: S1015–S1020.
Dai J, Chu R, Zhou X, Chen C, Qu X, Wang X . One-year outcomes of epi-LASIK for myopia. J Refract Surg 2006; 22: 589–595.
Dai J, Chu R, Zhou X, Chen C, Rao SK, Lam DS . Histopathological study of epithelial flaps in epi-LASIK. J Refract Surg 2007; 23: 637–638.
Tanioka H, Hieda O, Kawasaki S, Nakai Y, Kinoshita S . Assessment of epithelial integrity and cell viability in epithelial flaps prepared with the epi-LASIK procedure. J Cataract Refract Surg 2007; 33: 1195–1200.
Katsanevaki VJ, Naoumidi II, Kalyvianaki MI, Pallikaris G . Epi-LASIK: histological findings of separated epithelial sheets 24 h after treatment. J Refract Surg 2006; 22: 151–154.
Pallikaris IG, Naoumidi II, Kalyvianaki MI, Katsanevaki VJ . Epi-LASIK: comparative histological evaluation of mechanical and alcohol-assisted epithelial separation. J Cataract Refract Surg 2003; 29: 1496–1501.
O'Doherty M, Kirwan C, O'Keeffe M, O'Doherty J . Postoperative pain following epi-LASIK, LASEK, and PRK for myopia. J Refract Surg 2007; 23: 133–138.
Torres LF, Sancho C, Tan B, Padilla K, Schanzlin DJ, Chayet AS . Early postoperative pain following Epi-LASIK and photorefractive keratectomy: a prospective, comparative, bilateral study. J Refract Surg 2007; 23: 126–132.
Wang QM, Fu AC, Yu Y, Xu CC, Wang XX, Chen SH et al. Clinical investigation of off-flap epi-LASIK for moderate to high myopia. Invest Ophthalmol Vis Sci 2008; 49: 2390–2394.
Author information
Authors and Affiliations
Corresponding author
Additional information
This study was presented as a poster in the annual conference of the American Academy of Ophthalmology at New Orleans in November 2007
Rights and permissions
About this article
Cite this article
Sharma, N., Kaushal, S., Jhanji, V. et al. Comparative evaluation of ‘flap on’ and ‘flap off’ techniques of Epi-LASIK in low-to-moderate myopia. Eye 23, 1786–1789 (2009). https://doi.org/10.1038/eye.2008.367
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/eye.2008.367
Keywords
This article is cited by
-
Subjective pain, visual recovery and visual quality after LASIK, EpiLASIK (flap off) and APRK — a consecutive, non-randomized study
Graefe's Archive for Clinical and Experimental Ophthalmology (2013)
