
Abstract
Background
Adult height is independently related to ocular dimensions and shorter people have shorter globes and shallower anterior chambers. We investigated the relationship between adult height and angle dimensions to explore measuring height as a possible screening test for angle closure.
Methods
A population-based, cross-sectional survey of adult Chinese living in the Tanjong Pagar district, Singapore was conducted. Anterior chamber depth, gonioscopic angle width and height were assessed using standardized protocols.
Results
Data were available for 996 persons. Shorter people had shallower anterior chamber depth (2.35 mm for persons <144 cm vs2.72 mm for persons >170 cm, P=0.008) and smaller gonioscopic angles (22° for <144 cm vs30° for >170 cm, P=0.079). After controlling for age and gender, adult height was significantly related to anterior chamber depth (P=0.008) but not significantly related to gonioscopic angle width (P=0.079). Female sex and age ⩾50 years used together correctly identified 45/66 (68.2%) individuals with an occludable angle (sensitivity 68.2%, specificity 61.3%). Fewer people, 41/66 (62.1%), were correctly identified when height <160 cm was added to female sex and age 50 ⩾years (sensitivity was 62.1% and specificity was 64.7%).
Conclusions
Shorter adult height is significantly associated with a shallower anterior chamber depth, but the addition of height contributed little to demographics (age and gender) as the preliminary screening criteria to identify individuals at risk of an occludable angle.
Similar content being viewed by others

Introduction
Glaucoma is the leading irreversible cause of blindness worldwide.1 By 2010, it is estimated that primary angle closure glaucoma will account for nearly half of all glaucoma blindness.2 In the 1970s, the Inuit population of Greenland had the highest prevalence of glaucoma recorded, at 3.5% in the population aged 40 years and older.3 Intensive efforts to detect people at high risk or early established disease and offer prophylaxis and treatment has led to a reduction in the proportion of total blindness caused by angle-closure glaucoma from 64% in 1962 to 9% in 2003.4 In the context of a vast number of people at risk of glaucoma in Asia, it has been suggested that screening should be considered as a method of reducing the burden of glaucoma blindness in the region.5, 6 However, the feasibility of screening is primarily determined by the macroeconomics of healthcare within a particular country, and the microeconomics of delivery on a local level. Furthermore, the Jungner and Wilson precepts stipulate that, to justify screening, a disease should exist in an early, asymptomatic stage which is detectable using a safe, simple, non-invasive test.7 In this regard, there are well-recognized demographic risk factors which can help identify those at highest risk—Asian (specifically Chinese) ethnicity, female sex, and older persons.8 Anterior chamber biometry has also proven to be a useful method of identifying particular ocular characteristics associated with disease.9, 10, 11 However, this requires sophisticated, expensive equipment, which will not be widely available in the community settings in Asia. In a previous publication, we reported the association between physical height and ocular biometry in the Chinese population of Singapore.12 The fact that physically smaller people have shallower anterior chambers has led us to investigate the relationship between adult height and drainage angle dimensions, with a view to assess whether the measurement of adult height may be of additional value for the rapid assessment of risk from angle closure and its possible role as a surrogate for ocular biometry.
Materials and Methods
Study population
The Tanjong Pagar Survey was a population-based cross-sectional survey of ocular disorders among adult Chinese living in Singapore between October 1997 and August 1998. The population selection and methodology has previously been reported in detail.13 The Tanjong Pagar district encompasses areas with diverse social and economic backgrounds, therefore, it was regarded as representative of other regions in Singapore. A stratified, clustered, random sampling method selected 2000 (13.3%) of the 15 082 persons of the district identified by using the electoral register. From each of the four age strata, 500 persons were selected randomly—40–49, 50–59, 60–69, and 70–79. Of the 2000 persons initially selected, 1717 were finally eligible for the study because 46 had died, 235 had moved away, and 2 were excluded due to ill health. These individuals were invited to receive a thorough eye examination at the study clinic. An abbreviated home examination was conducted on non-respondents. Only the subjects examined at the clinic received a biometric examination (1090 subjects).
Procedures
The examination procedures followed a standardized protocol as previously published.13 Height was measured with the individual standing without shoes and recorded in centimetres. A slitlamp (model BQ900; Haag-Streit, Bern, Switzerland) was used to examine the anterior segment. Intraocular pressure (IOP) was measured using an applanation tonometre (Goldmann model; Haag-Streit). Three readings were taken and the median taken as the eye pressure. Gonioscopy was performed using a Goldmann-type 1-mirror lens (model 902; Haag Streit) at × 25 magnification with low ambient illumination. The iridotrabecular angle was graded in four quadrants using the Shaffer grading system. Measurements of axial length and anterior chamber depth (usACD) were obtained using a 10-MHz A-mode ultrasound machine (Compuscan; Storz, St Louis, MO, USA). The hard-tipped corneal contact ultrasound probe was mounted on a tonometre (Haag-Streit) set to the subject's intraocular pressure. The mean of 16 separate readings was recorded with the SD for each parameter.
Definitions
Age was defined as the age at the time of examination. The subjects were categorized into six different groups according to height in centimetres: <144, 145–149, 150–154, 155–159, 160–164, 165–169, and >170. An occludable angle was defined as one in which the pigmented or posterior trabecular meshwork could be seen for less than 90° of the angle circumference. The gonioscopic angle was defined as the mean grade (using the Shaffer grading system, in degrees) of four quadrants. Grade 0=0°, grade 1=0–10°, grade 2=10–20°, grade 3=20–30°, grade 4⩾40°.
True anterior chamber depth (true ACD) was defined as the distance between corneal endothelium and anterior lens capsule along the geometric axis of the globe. This was calculated by subtracting optical pachymetry central corneal thickness from optical pachymetry anterior chamber depth (corneal epithelium to anterior lens capsule). Ultrasound ACD was the measurement from the corneal epithelium to the anterior lens capsule. Optical ACD measurements were generally more accurate and reproducible; hence, these measurements were used to assess the relationship between height and anterior chamber depth and angle dimensions. Ultrasound ACD measurements can be more variable; however, ultrasound was more feasible for screening so these measurements were used to identify individuals with occludable angles.
Statistical analysis
The analyses were conducted using only the data from the right eyes of phakic subjects. Statistical analyses of the data were conducted using the statistical analytical software SPSS (Chicago, IL, USA). Results are expressed as means±SD. Univariate associations between age, sex, and height with different angle dimensions were calculated. Linear regressions were used to determine the effect of age, sex, and height (independent variables) on specific angle dimensions. Then multiple linear regression was used to evaluate the effect of height on specific angle dimensions while controlling for age and sex.
Results
Data were available for 996 people of whom 450 were men and 546 were women. Subjects were excluded if there were signs of secondary glaucoma, previous intraocular surgery or ocular findings consistent with the presence of secondary peripheral anterior synechiae (PAS) such as uveitis or trauma. The age range was 40–81 years (mean 58.2 years). There were 996 people with data for height, gonioscopy angle width, IOP, true and ultrasound ACD. The following data were missing: 4 for height, 52 for ultrasound ACD, 19 for true ACD, 3 for IOP, and 4 for RE mean gonioscopy score.
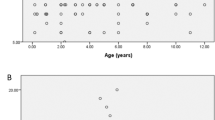
True ACD was shallower in shorter persons: from a mean of 2.35 mm for the <144 cm group to mean of 2.72 mm for the >170 cm group (Table 1; Figure 1a). Adult height was significantly correlated (r=0.283, P=0.008) with axial ACD. The mean gonioscopic angle width was smaller in shorter persons: from a mean of 22° for the <144 cm group to 30° for the >170 cm group (Table 1; Figure 1b). After controlling for age and sex, the relationship between height and gonioscopic angle width was not statistically significant (P=0.079). Mean IOP was inversely related to height: 15.8 mmHg for those <144 cm to 14.0 mmHg for the >170 cm group. Linear regression suggested a decrease in IOP of 0.39 mmHg per 10 cm increase in height (95% CI: 0.13, 0.65; P=0.004; Table 1).

Graph (a) shows significant increase in true anterior chamber depth (mm) with increasing height category P=0.008. Graph (b) shows increase in gonioscopic width (Shaffer grade) with increasing height category (P=0.079).
We examined the association between gonioscopically occludable angles and various demographic and morphometric indices, to assess the potential value of each of these as tools for detection of people at increased risk of angle closure. Of the 996 individuals (Table 2), 735 (73.8%) participants were ⩾50 years of age, 546 (54.8%) were women, and 582 (58.7%) people were of height <160 cm. There were 337 (33.8%) people with an ultrasound ACD of ⩽2.75 mm (equivalent to true ACD ⩽2.22 mm with CCT of 0.53). A total of 66/996 individuals had an occludable angle in the right eye. 62/66 (93.9%) were aged ⩾50 years, 47/66 (71.2%) were female, and 45/66 (68.2%) of these individuals were of height <160 cm. Of these 66 subjects, 51 (77.3%) had an ultrasound ACD ⩽2.75 mm (true ACD 2.22).
If female sex and age ⩾50 years were used as the first tier of selection criteria, we would correctly identify 45/66 (68.2%) people with an occludable angle (Table 2). Adding height <160 cm to the initial criteria, 41/66 (62.1%) people with an occludable angle were identified. In addition, by adding ultrasound ACD ⩽2.75 mm to the criteria, 36/66 (54.5%) people were identified.
The sensitivity and specificity values for the above combinations of criteria to identify individuals at risk of an occludable angle are indicated in Table 3. For the first set of criteria (test 1, age ⩾50 years and female sex) the sensitivity was 68.2% and the specificity was 61.3%. For the second set of criteria (test 2, where height <160 cm alone was used) the sensitivity was unchanged (68.2%) although the specificity was lower (42.7%). For the third set of criteria (test 3, age ⩾50 years, female sex, and height <160 cm) the sensitivity was 62.1% and the specificity was 64.7%. The ROC curves (for age, sex, and height) indicate that height would identify people with occludable angles better than chance; however, with not enough precision to justify its use as a screening tool (Figure 2a and b). PAS were identified in the right eyes of 45/996 people (Table 2). Of these 45, 39 (86.7%) were aged ⩾50 years old, 22 (48.9%) were of female sex, 26 (57.8%) were of height <160 cm, and 22 (48.9%) had an ultrasound ACD ⩽2.75 mm.

ROC curves for height alone (a) and for sex and age (b) showing that height would identify people with occludable angles better than chance, however, with not enough precision to justify its use as a screening tool.
Conclusion
It has long been hypothesized that height is significantly associated with differences in the dimensions of organs other than eyes. These associations may predispose persons with different heights to different anatomical risks of angle closure such as angle crowding. There have been few studies, however, that have investigated this relationship in detail. One study used magnetic resonance imaging to show that adult right ventricles volumes and linear dimensions were significantly correlated with height.14 A previous study by our group reported that adult height in a Chinese population was independently related to ocular dimensions even after controlling for age, sex, education, occupation, income, housing type, and weight, namely shorter people had shorter axial lengths and shallower anterior chambers.12 Our study now shows that decreasing adult height in the same population is significantly associated with a shallower ACD and not significantly with smaller gonioscopic angle width, after adjusting for age and sex. This may have been because gonioscopy examination is not as precisely measured as ACD. Alternatively, the results suggest that height is associated with shorter globe but not with angle crowding. It is possible, that over time height may be associated with changes in angle width with the onset of changes in lens dimensions and cataract development.
Our analysis shows that assessment of height for screening of angle closure makes no useful contribution. The initial selection criteria of female sex and age ⩾50 years (test 1) used to identify individuals at risk of an occludable angle correctly identified 68.2% of the population already known to have an occludable angle. The specificity of test 1 was relatively modest at 61.3%, indicating a significant number of false negatives would arise if this test were applied. The sensitivity and specificity of test 3 when height of <160 cm was added to the initial criteria (age ⩾50 years and female sex) did not improve markedly (62.1 and 64.7%, respectively), suggesting that the use of height did not add great value to this screening test. Therefore, it further suggests that although decreasing adult height is significantly associated with a shallower ACD, measurement of height does not significantly contribute to the identification of individuals at risk of an occludable angle over age and gender.
Interestingly, the use of combining the measurement ACD with height, female sex and age ⩾50 years appeared to reduce the sensitivity of the test to correctly identify at-risk individuals—with only 54.5% of the population with an occludable angle correctly identified. This may have been because adult height was shown to be significantly associated with ACD and the use of both of these parameters may have partially cancelled each other out.
The main strength of this study is that it was a randomly sampled population-based survey thus avoiding the potential biases associated with studying highly selected specific population groups. However, there may have been a few limitations to the study. Firstly, we were unable to control for unmeasured potential confounders of associations of stature with angle dimensions. For example, we did not have data on socio-economic factors during childhood, family histories of height, or documentation of near-work activities all of which may have been important. Nevertheless, we did control for proxies of socio-economic status such as education and income.
Secondly, there may have been some selection bias. Although the overall participation rate in the survey was 71.8%, complete data for this part of the analysis was only available for 49.6%. In our previous report, despite the random selection process the younger subjects in this survey turned out to be younger, taller, and heavier; have higher levels of education; were more likely to be professionals or be office workers and live in better housings with higher incomes than the older subjects. We believe that the Singapore population is experiencing a significant shift in socio-economic structure before independence in 1965, which has resulted in markedly higher standards of living and a shift in indices of ocular health and structure. Therefore, it would be important to consider the effects of these differences in socio-economic backgrounds on our findings. Thirdly, the data was cross-sectional with all the parameters measured at one time point. It is uncertain how the findings of this study might apply to populations of different ethnicity. We did not incorporate the refractive state of individuals into our analysis because our previous study did not find a relationship between adult height and refraction.
In conclusion, our findings indicate that shorter adult height is significantly associated with a shallower ACD, but not gonioscopic angle width, once age and sex were adjusted for. We had hypothesized that this relationship may offer an inexpensive method of estimating the risk of angle-closure glaucoma in high-risk populations, especially in remote rural areas of non-industrialized Asian nations. However, although the use of demographics (age and sex) as preliminary screening criteria to identify individuals at risk of an occludable angle seems to perform relatively well, the addition of height to demographics contributes little to the screening test. Thus, age and sex could easily form the basis of a rapid assessment programme to target these individuals to reduce the prevalence of this potentially blinding disease.
References
Resnikoff S, Pascolini D, Etya’ale D, Kocur I, Pararajasegaram P, Pokharel GP et al. Global data on visual impairment in the year 2002. Bull World Health Organization 2004; 82: 844–851.
Quigley HA, Broman AT . The number of persons with glaucoma worldwide in 2010 and 2020. Br J Ophthalmol 2006; 90: 262–267.
Alsbirk PH . Anterior chamber depth and primary angle-closure glaucoma. I. An epidemiologic study in Greenland Eskimos. Acta Ophthalmol 1975; 53: 89–104.
Johnson GJ, Foster PJ . Can we prevent angle-closure glaucoma? Eye 2005; 19: 1119–1124.
Foster PJ, Johnson GJ . Glaucoma in China: how big is the problem? Br J Ophthalmol 2001; 85: 1277–1282.
Nolan WP, Baasanhu J, Undraa A, Uranchimeg D, Ganzorig S, Johnson GJ . Screening for primary angle closure in Mongolia: a randomised controlled trial to determine whether screening and prophylactic treatment will reduce the incidence of primary angle closure glaucoma in an east Asian population. Br J Ophthalmol 2003; 87: 271–274.
Wilson JMG, Jungner G . Criteria for assessing the viability, effectiveness and appropriateness of a screening programme. 34. World Health Organization Public Health paper, Geneva, 1968.
Yip JL, Foster PJ . Ethnic differences in primary angle-closure glaucoma. Curr Opin Ophthalmol 2006; 17: 175–180.
Devereux JG, Foster PJ, Baasanhu J, Uranchimeg D, Lee PS, Erdenbeleig T et al. Anterior chamber depth measurement as a screening tool for primary angle-closure glaucoma in an East Asian population. Arch Ophthalmol 2000; 118: 257–263.
Foster PJ, Devereux JG, Alsbirk PH, Lee PS, Uranchimeg D, Machin D et al. Detection of gonioscopically occludable angles and primary angle closure glaucoma by estimation of limbal chamber depth in Asians: modified grading scheme. Br J Ophthalmol 2000; 84: 186–192.
Nolan WP, Aung T, Machin D, Khaw PT, Johnson GJ, Seah SK et al. Detection of narrow angles and established angle closure in Chinese residents of Singapore: potential screening tests. Am J Ophthalmol 2006; 141: 896–901.
Wong TY, Foster PJ, Johnson GJ, Klein BE, Seah SKL . The relationship between ocular dimensions and refraction with adult stature: the Tanjong Pagar Survey. Invest Ophthalmol Vis Sci 2001; 42: 1237–1242.
Foster PJ, Oen FT, Machin DS, Ng TP, Devereux JG, Johnson GJ et al. The prevalence of glaucoma in Chinese residents of Singapore. A cross-sectional population survey in Tanjong Pagar district. Arch Ophthalmol 2000; 118: 1105–1111.
Tandri H, Daya SK, Nasir K, Bomma C, Lima JAC, Calkins H et al. Normal reference values for the adult right ventricle with magnetic resonance imaging. Am J Cardiol 2006; 98: 1660–1664.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Chang, L., Aung, T., Low, S. et al. Is measurement of adult height useful in screening for primary angle closure?. Eye 23, 1775–1780 (2009). https://doi.org/10.1038/eye.2008.375
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/eye.2008.375
