
Abstract
Background/Objectives:
Weight management medications increase the likelihood that patients will achieve clinically meaningful improvements in cardiovascular, metabolic and other weight-related measures of health. However, the weight loss achieved with any weight management intervention can vary widely among individuals, and patients who do not respond to pharmacotherapy by achieving clinically meaningful weight loss should discontinue therapy. We characterized 1-year weight loss in the phase 3 clinical trial program of the weight management medication, naltrexone/bupropion 32/360 mg (NB), as well as the relationship between early weight loss and long-term weight loss, particularly with respect to participants who achieved the clinically recommended threshold of ⩾5% weight loss by Week 16.
Participants/Methods:
Data from participants from each of the four phase 3, randomized, placebo-controlled, 56-week clinical trials with NB were pooled (modified intent-to-treat population; NB N=2043, Placebo N=1319). This exploratory analysis examined the relationship between participant achievement of various weight loss thresholds early in treatment (at Week 8, 12 or 16) and the associated weight loss at Week 56 (Completers population; NB N=1310, Placebo N=763).
Results:
In the NB participants who completed 1 year of treatment, weight loss of at least 5% at Week 16 (n=873) was associated with least-squares mean weight loss of 11.7% at Week 56 and 85% of these participants had Week 56 weight loss of ⩾5%. Eighty percent (95% confidence interval: 78–82%) of the participants who would, and would not, achieve ⩾5% weight loss at Week 56 were correctly identified using the clinically recommended threshold of ⩾5% at Week 16. Safety and tolerability of NB was similar to previously published reports.
Conclusions:
Participants who meet the Week 16 threshold of ⩾5% weight loss are likely to maintain clinically significant weight loss after 1 year of treatment. Further evaluations are required to evaluate improvements in measures of cardiovascular and metabolic risk.
Similar content being viewed by others
Introduction
Lifestyle intervention is the foundation of weight loss and weight management, but additional treatment modalities are often required to produce adequate weight loss.1, 2 Weight management medications are appropriate treatment options for individuals who are overweight or obese and have been unable to achieve weight loss with lifestyle intervention alone. When combined with a reduced-calorie diet and increased physical activity, weight management medications can facilitate achievement and maintenance of clinically meaningful weight loss (that is, weight loss of at least 5%) and lead to corresponding improvements in cardiovascular and metabolic risk factors.3, 4 However, as with lifestyle intervention, not all patients respond to weight management medication with clinically meaningful weight loss, likely owing to individual variability in efficacy, tolerability, safety and patient persistence.4
Exposure to any medication carries some measure of risk; therefore, early identification of long-term treatment responders (patients likely to achieve clinically meaningful weight loss of at least 5% at 1 year) and non-responders (patients unlikely to achieve clinically meaningful weight loss) can mitigate unnecessary drug exposure in patients unlikely to experience weight loss. Weight loss in the first few months of initiating lifestyle intervention, as well as the first few months of the weight loss medications orlistat or sibutramine (withdrawn from the market in 2010), is associated with weight loss for up to 2 years.5, 6, 7 Thus, given the relationship between early and long-term weight loss, prescribing information for the weight management medications lorcaserin and phentermine/topiramate extended release (ER), both approved in the United States (US) in 2012, includes evaluation of patient weight loss after 12 weeks of therapy at full dose, and guidance for either drug discontinuation (lorcaserin), or possible dose escalation with subsequent treatment cessation if early weight loss thresholds are not reached (phentermine/topiramate ER).8, 9
Naltrexone ER 32 mg/bupropion ER 360 mg (NB) is a weight management agent approved (Contrave in the US (September 2014) and Mysimba in the European Union (March 2015)) as an adjunct to a reduced-calorie diet and increased physical activity in obese and overweight adults.10 In four randomized, controlled, phase 3 clinical trials, participants taking NB were approximately three to five times more likely to achieve clinically meaningful weight loss at Week 56 as participants taking placebo.11, 12, 13, 14 As with other recently approved weight loss medications,8, 9 the prescribing information for NB includes an evaluation of weight loss after treatment with the maintenance dose (32 mg naltrexone ER/ 360 mg bupropion ER) for 12 weeks, which, in conjunction with a 4-week dose-escalation period, means the assessment should occur approximately 16 weeks after initiation of treatment.10
The purpose of this investigation was to evaluate early weight loss with NB as a predictor of clinically meaningful long-term weight loss. Pooled, participant-level data from the phase 3 NB development program was used to evaluate early weight loss with NB as a predictor of achievement of long-term (Week 56) weight loss of ⩾5%.
Participants and methods
The phase 3 (COR) program
The Contrave Obesity Research (COR) program comprised four multicenter, randomized, double-blind, placebo-controlled phase 3 clinical trials designed to evaluate the efficacy and safety of NB over a 56-week period (Table 1). The COR clinical trials were conducted between March 2007 and June 2009 and the data have been published previously.11, 12, 13, 14 Participants were 18–65 years old with a body mass index (BMI) 30–45 kg m−2, or BMI 27–45 kg m−2 and dyslipidemia and/or controlled hypertension, except for the COR-DM clinical trial, which included participants with type 2 diabetes mellitus (DM, HbA1c from 7–10% and fasting blood glucose <270 mg dl−1), aged 18–70 years, and with a BMI 27–45 kg m−2.
Briefly, the COR-I clinical trial compared the efficacy and safety of placebo with two doses of NB: the approved 32 mg naltrexone ER/360 mg bupropion ER daily dose (NB), and a lower dose of 16 mg naltrexone ER/360 mg bupropion ER (NB16).11 The present analysis excluded participants randomized to the NB16 dose. The COR-II clinical trial also evaluated the efficacy and safety of the approved NB dose; however, if participants randomized to NB did not achieve or maintain at least 5% weight loss at any time from Week 28 to Week 44, they were re-randomized to either NB or 48 mg naltrexone ER/360 mg bupropion ER (NB48).12 Because there was no significant difference in weight change following re-randomization to NB48 versus NB, the analysis was based on observed values from these participants regardless of NB dose following re-randomization. COR-DM evaluated the approved NB dose for the treatment of overweight or obesity in participants with type 2 DM.14 In COR-I, COR-II and COR-DM, participants received information on standard lifestyle intervention periodically from personnel at the study sites, consisting of instructions to follow a hypocaloric diet (500 kcal per day deficit) and increase physical activity, as well as limited behavioral modification advice. The COR-BMOD clinical trial evaluated NB or placebo in combination with an intensive program of diet, exercise and behavior modification therapy (BMOD), which consisted of 28 sessions delivered to groups of 10–20 participants by registered dietitians, behavioral psychologists or exercise specialists.13
Assessments (including body weight measurement) were conducted at each visit (Day 1 and every 4 weeks). Baseline weight was considered the weight obtained prior to initiating study treatment on Day 1. The primary end points in COR-I, COR-BMOD and COR-DM were the percent change in weight from baseline to Week 56 and the percentage of participants achieving at least a 5% reduction in weight from baseline to Week 56. In COR-II, the primary end point was percent change in weight from baseline to Week 28 and percentage of participants achieving at least 5% reduction in weight from baseline to Week 28, although the clinical trial continued for 56 weeks. Efficacy analyses were performed on the modified intent-to-treat population (mITT, participants with a baseline and at least one post-baseline weight measurement while on study treatment with last-observation-carried-forward imputation of missing data; NB N=2043, Placebo N=1319) and Completers population (participants who had a baseline and Week 56 weight measurement while on study treatment; NB N=1310, Placebo N=763). Adverse event (AE) frequency was compared between NB and placebo for the completer analysis set. Detailed safety assessments were previously reported for each trial.11, 12, 13, 14
Data analyses
The purpose of this exploratory analysis was to examine, among participants who received NB, the relationship between achievement of various early (Weeks 8, 12 or 16) weight loss thresholds in the four phase 3 clinical trials and the associated weight loss at the end of the trials (Week 56).
For the evaluation of each early weight loss threshold, responders were defined as participants who lost at least 2, 3, 4 or 5% of baseline weight at Weeks 8, 12 or 16. Non-responders were defined as participants who either gained weight or who did not achieve the responder threshold of 2, 3, 4 or 5% weight loss at a given time point. No imputation was used for early weight loss threshold values, and participants without an observed weight loss value at a given early threshold were considered non-responders for that analysis. These weight loss response thresholds were chosen based on current guidelines for use of the weight management medications8, 9, 15 and evidence that 5% weight loss is associated with clinically meaningful improvements in cardiovascular and metabolic risk factors.16, 17, 18
For analyses examining the relationship between participant achievement of these various early treatment weight loss thresholds and the associated weight loss at Week 56, only data from the Week 56 Completers population were used (that is, those participants that were on study treatment at Week 56). There were some participants in the Completers population who did not have a Week 56 weight assessment. In those rare instances, the percent change in weight loss at Week 56 was imputed using LOCF methodology.
Week 56 weight loss and weight loss by visit were calculated for each of the early responder and non-responder thresholds, along with the proportion of responders and non-responders who achieved at least 5, 10 and 15% weight loss at Week 56. Week 56 weight loss for the combined phase 3 mITT and Completers populations was calculated using general linear models (analysis of covariance) that included factors for treatment and study and baseline weight as a covariate.
For the categorical outcome variables, descriptive statistics included number and percentage of participants for each category. For the continuous outcome variables, descriptive statistics included number of participants (n), mean, standard deviation (s.d.), and standard error (s.e.). For comparison of categorical outcome variables, either a chi-squared test or a logistic regression model was used with treatment, study and baseline body weight as covariates. Exact (Clopper-Pearson) confidence intervals (CIs) are used for calculating the 95% CIs for proportions. All statistical analyses were performed using SAS software (Version 9.1 or higher, SAS Institute Inc., Cary, NC, USA).
Results
Evaluation of weight loss with NB compared with placebo in the phase 3 clinical trials
Baseline demographics and characteristics of participants who completed the phase 3 clinical trials were similar for placebo and NB treatment groups (Table 2). Weight loss by visit in the combined phase 3 clinical trials was greater for participants who completed the study (NB=1310, placebo=763) than for the mITT primary analysis population (NB=2043, placebo=1319, Figure 1a). Week 56 least-squares mean weight loss for the combined phase 3 mITT population was 7.0% (s.e. 0.2%) for the NB group and 2.3% (s.e. 0.2%) in the placebo group (P<0.001). NB completers lost 8.8% (s.e. 0.2%) of baseline body weight and placebo completers lost 3.1% (s.e. 0.3%) over 56 weeks (P<0.001). In both the mITT and completer analysis populations, a greater number of NB-treated participants achieved at least 5% weight loss at Week 56 compared with placebo (Figure 1b).

Weight loss in the phase 3 clinical trials. Weight loss by visit (a; least-squares (LS) mean+s.e.) and proportion of participants with ⩾5% weight loss at Week 56 (b) in the mITT and Completer populations.
Assessment of early weight loss thresholds in NB-treated completers for the identification of Week 56 responders
In general, greater initial weight loss with NB in clinical trial completers (that is, mean weight loss achieved at any given early responder evaluation threshold) was associated with greater mean weight loss at Week 56 (see Supplementary Table 1, which presents the proportion of NB completers who achieved (responders) or did not achieve (non-responders) weight loss thresholds of 2, 3, 4 and 5% at Weeks 8, 12 and 16, and the Week 56 weight loss observed in each group). Because all participants in the NB phase 3 clinical trials were allowed to continue study treatment regardless of their early weight loss, these clinical data also allow for an assessment of a range of early weight loss thresholds to correctly predict 5% responder status at Week 56 (Table 3). NB is initiated with a 4-week dose-escalation period; therefore, the threshold of ⩾5% weight loss at Week 16 was chosen as the threshold most representative of the evaluation recommended in the prescribing information (that is, assessment for ⩾5% weight loss after 12 weeks of therapy with maintenance dose).
In Table 3, participants who either achieved an early threshold and went on to achieve 5% weight loss at 1 year or those who failed the early threshold and did not achieve 5% weight loss at 1 year, are both considered ‘correctly identified’ and combined into a single group as a measure of prediction accuracy. Data are presented separately for those who would have stayed on drug for 1 year and not achieved 5% weight loss at 1 year (‘unjustified exposure’), and those who did not achieve the early threshold but did achieve the long-term 5% weight loss goal (‘missed opportunity’).
The clinically recommended threshold of ⩾5% at Week 16 correctly identified 80% (95% CI: 78–82%) of the participants who would, and would not, achieve ⩾5% weight loss at Week 56. The 20% of participants who would not have been correctly identified using this criterion were divided nearly equally among those who would have been inappropriately removed from treatment due to insufficient weight loss at Week 16 (that is, despite ultimately achieving ⩾5% at Week 56; n=125) and those who would have inappropriately continued study treatment for 1 year (that is, participants who achieved the ⩾5% at Week 16 threshold but did not achieve ⩾5% weight loss at Week 56; n=132). Of note, nearly all participants re-randomized to received either NB32 or NB48 owing to insufficient early weight loss in the COR-II trial also did not achieve at least 5% weight loss at Week 56 (95% and 97%, respectively). Thus, even if all participants who received NB48 were defined conservatively as Week 56 non-responders, the correctly identified proportion with Week 16 ⩾5% remained identical at 80%.
The COR clinical trials included diverse cohorts of patient types and background therapies, which will influence weight loss. Yet, when evaluating the early responder thresholds in only participants with type 2 diabetes (COR-DM), in only participants without type 2 diabetes receiving intensive behavioral modification therapy (COR-BMOD) and in only participants without type 2 diabetes receiving standard lifestyle therapy (COR-I/COR-II), a similar pattern emerged in which the ⩾5% at Week 16 threshold appeared to offer the best overall prediction for each clinical trial and participant type (Supplementary Table 2).
Week 56 weight loss in completers who achieved 5% weight loss at Week 16
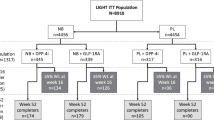
We evaluated attainment of the clinical recommendation for 5% weight loss at Week 16 in the clinical trial program, as well as the weight loss in early responders who completed 56 weeks of treatment (that is, those expected to continue treatment with NB in clinical practice). A greater proportion of NB-treated participants achieved weight loss of at least 5% at Week 16 compared with placebo (Figure 2a; 51% (n=1038) of NB participants and 19% (n=254) of placebo participants in the mITT population). Moreover, 87% (903/1038) of these NB-treated responder participants continued treatment for 1 year, while 13% (135/1038) did not. For comparison, 81% (206/254) of the placebo-treated responder participants continued treatment for 1 year, while 19% (48/254) did not. These NB responder/completer participants exhibited an least-squares mean Week 56 weight loss of 11.7%, with 85%, 57% and 32% achieving at least 5%, 10% and 15% weight loss, respectively, at Week 56 (Figures 2b and c), which was consistently greater than that observed in placebo participants who exhibited at least 5% weight loss after 16 weeks. Furthermore, weight loss in placebo reached an apparent nadir at Week 26, while no clear nadir was identified over the 56-week period in responder participants who received NB (Figure 2b). Individual Week 56 weight change for all responder/completers is shown in Figure 2d. Of NB responder/completers, 85% (95% CI: 82–87%; 741/873) of NB-treated patients who had 5% weight loss at Week 16 also had 5% weight loss at Week 56. As a conservative sensitivity analysis, if it were assumed that the 13% of NB-treated participants who were Week 16 responders, but did not complete the study, were all included in the analysis as participants who did not maintain 5% at 1 year, then 71% (95% CI: 69–74%; 741/1038) would be the estimate of participants who had 5% weight loss at Week 16 and also had 5% weight loss at Week 56. For comparison, a similar conservative sensitivity analysis with the placebo-treated participants estimates that 56% (95% CI: 50–62%; 142/254) of placebo participants who had 5% weight loss at Week 16 and also had 5% weight loss at Week 56.

Achievement of the clinically recommended ⩾5% weight loss at Week 16 and associated Week 56 weight loss. (a) Proportion of participants with ⩾5% weight loss at Week 16 in the mITT population. (b) Weight loss by visit (least-squares (LS) mean+s.e.), and (c) proportion of participants with categorical weight loss at Week 56 in the Week 16 ⩾5% responder/completer population. (d) Week 56 weight change for each participant in the Week 16 ⩾5% responder/completer population.
The pattern of 56-week weight loss for the NB Week 16 ⩾5% weight loss responders was similar across the phase 3 trials (Supplementary Figure 1). In general, responders in the COR-BMOD clinical trial, which included an intensive lifestyle intervention, exhibited greater mean Week 56 weight loss than responders in the COR-I/COR-II clinical trials, and NB responders in the COR-DM clinical trial, which included only participants with type 2 diabetes, exhibited less weight loss. Despite these mean differences in weight loss across trials, the ⩾5% at Week 16 weight loss threshold was similarly predictive of ⩾5% weight loss at Week 56 (Supplementary Table 2).
Week 56 weight loss in NB-treated completers who did not achieve 5% weight loss at Week 16
Least-squares mean percent change in weight at 1 year in NB-treated participants who did not achieve the 5% threshold at 16 weeks was 2.65% (s.e. 0.25; n=437). Also, 10% of NB-treated completers did not achieve a 5% weight loss at 16 weeks, but subsequently achieved a 5% weight loss at 1 year (Table 3. ‘Responder removed from treatment’), which represents 30% of the NB Week 16 non-responder population.
Safety
Adverse events in NB- and placebo-treated Week 56 completers (Table 4) were similar to the previously published reports of the Safety population in each of the four clinical trials.11, 12, 13, 14 In NB-treated clinical trial completers, nausea, constipation and headache were the most frequently reported AEs with greater incidence than placebo.
Among NB participants who had lost ⩾5% at Week 16, the most frequent (⩾10% incidence with NB) AEs observed during the trials were: nausea (29.2%), constipation (28.8%), headache (16.7%), upper respiratory tract infection (11.5%) and dry mouth (10.8%). In Week 16 non-responders on NB, the most frequent AEs observed across the clinical trials were nausea (28.2%), constipation (18.2%) and headache (16.6%). Consistent with previously published reports, AEs with NB were transient; the incidence of AEs was lower after the Week 16 assessment.11, 12, 13, 14
Discussion
In this combined analysis of the phase 3 COR program, weight loss in the first 4 months of NB treatment was associated with greater weight loss at 1 year for all evaluated early thresholds. Specifically, weight loss of at least 5% at Week 16 in participants randomized to NB was associated with mean weight loss of approximately 12% at Week 56; 85% of these participants had a Week 56 weight loss of at least 5%, and 57% achieved ⩾10% weight loss. These data support the clinical recommendation in the prescribing information for NB, which requires assessment for 5% weight loss after 12 weeks of treatment with the maintenance dose of NB (that is, at Week 16).
Because participants in the phase 3 clinical trials were allowed to continue study treatment for 1 year regardless of early weight loss, the effectiveness of an early threshold in identifying Week 56 5% responders and non-responders could be evaluated with this phase 3 clinical data. A number of early assessments were evaluated as indicators of achievement of 5% weight loss at Week 56, and in general, most of the lower thresholds and earlier thresholds would have allowed a larger number of non-responders to continue treatment for 1 year, or would have removed a greater number of responders with little improvement in the ability to remove non-responders from treatment. Thus, the clinically recommended threshold of 5% weight loss at Week 16 was accurate in 80% (95% CI: 78–82%) of cases, with misclassifications evenly divided between inaccurate predictions of failure and inaccurate predictions of success. While the proportion Week 56 ⩾5% weight loss responders who were correctly identified with the Week 16 ⩾4% and ⩾5% thresholds were similar, the ⩾4% threshold suggested a greater tendency to allow long-term non-responders to continue treatment. The threshold prior to Week 16 that most closely approximated the performance of the clinically recommended threshold was ⩾4% weight loss at Week 12.
This is the first combined analysis of weight loss in the four COR clinical trials. Consistent with reports of each of the clinical trials,11, 12, 13, 14 participants who received NB treatment had greater weight loss compared with placebo. Importantly, over 2.5 times as many participants achieved the clinical recommendation of ⩾5% weight loss after Week 16 in the phase 3 COR trials with NB versus placebo (Figure 1b), and almost 90% of participants who achieved this early threshold continued NB treatment for the duration of the clinical trial. The magnitude of weight loss observed in these NB responders at 1 year has been associated with significant reductions in cardiovascular and metabolic risk,18, 19, 20 improvements in other weight-related measures such as sleep apnea,21 urinary incontinence22 and quality of life,23 and can prevent or delay the development of diabetes.24 Individual participant weight loss at Week 56 varied greatly around mean weight loss within the combined group of all NB responders (as depicted in Figure 2d), and a similar pattern was observed separately within each trial type (Supplementary Figure 1, right panel). This may be important information for physicians and patients when discussing patient expectations about weight loss.
The phase 3 COR clinical trials incorporated a diverse population that was broadly representative of the general obese population. Differences in patient type (with or without type 2 DM) and background lifestyle therapy (standard vs intensive) are known to influence the effectiveness of pharmacotherapy and were examined in discrete clinical trials. Week 56 mean weight loss among NB-treated participants who had ⩾5% weight loss at Week 16 varied by clinical trial type (Supplementary Figure 1; left panel); however, the ability of the Week 16 ⩾5% weight loss criteria to predict a 5% weight loss at Week 56 is consistent in participants across each of the four COR clinical trials. It is important to note that the observations discussed above regarding the performance of various early weight loss thresholds in the integrated phase 3 clinical trial analysis also hold true when looking only at participants with type 2 diabetes or participants who received intense behavior modification therapy (Supplementary Table 2). Thus, in clinical practice, overweight/obese patients who achieve at least 5% weight loss by Week 16, including those affected by type 2 diabetes, would be expected to experience improvements in cardiovascular and metabolic risk factors.
This analysis was conducted to predict the experience with NB in clinical practice. To this end, we excluded results in participants who received a lower dose of NB (NB16) that was evaluated in the COR-I clinical trial but was not approved for weight management therapy.10, 11 Compared with NB, NB16 resulted in lower mean weight loss at Week 56 and a smaller proportion of participants achieving clinically significant weight loss of at least 5% at Week 56, despite a similar safety and tolerability profile. Conversely, a higher dose of NB (NB48), which was evaluated in the latter half of COR-II in non-responders, was included in the analysis even though it is not approved for weight management because NB48 produces similar weight loss and has a safety and tolerability profile that is similar to NB.10, 12 A limitation of this analysis is that participants in these trials were not required to demonstrate 5% weight loss at Week 16 (or any of the alternative weight loss early thresholds) to continue treatment and as such, participant behavior around these thresholds may differ in real world use. Finally, long-term data from the placebo-treated participants who were early responders are not presented in the manuscript because the valid placebo-controlled comparison is the achievement of the early weight loss threshold (Figure 2a), a threshold that was achieved by approximately two and a half times the proportion of participants compared with placebo group. The relatively low proportion of participants who were on placebo and achieved substantial early weight loss with the background lifestyle modification exhibited, as would be expected, substantial weight loss over the long term (−8.8% (s.e. 0.52) at 1 year).
Conclusion
Early identification of patients who are unlikely to achieve clinically meaningful weight loss with a weight management medication reduces the risk of unnecessary exposure. The NB prescribing information recommends an evaluation after 12 weeks of maintenance therapy (approximately 16 weeks after initiation of dosing), using 5% weight loss as a threshold for continuing treatment. This is the first analysis of the COR phase 3 clinical trials to assess the relationship between early (Week 16) and long-term (Week 56) weight loss for NB, and to evaluate the effectiveness of the early responder threshold in identifying patients who will achieve clinically significant weight loss at Week 56. This analysis demonstrated that the majority of NB participants achieved this early threshold, and of the participants who achieved this threshold, nearly 90% continued treatment for 1 year and achieved a mean weight loss of nearly 12%.
References
Jensen MD, Ryan DH, Apovian CM, Ard JD, Comuzzie AG, Donato KA et al. 2013 AHA/ACC/TOS Guideline for the management of overweight and obesity in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and The Obesity Society. Circulation 2014; 129 (suppl 2): S102–S138.
Wadden TA, Volger S, Tsai AG, Sarwer DB, Berkowitz RI, Diewald LK et al. Managing obesity in primary care practice: an overview with perspective from the POWER-UP study. Int J Obes 2013; 37 (Suppl 1): S3–11.
Kim GW, Lin JE, Blomain ES, Waldman SA . Antiobesity pharmacotherapy: new drugs and emerging targets. Clin Pharmacol Ther 2014; 95: 53–66.
Yanovski SZ, Yanovski JA . Long-term drug treatment for obesity: a systematic and clinical review. JAMA 2014; 311: 74–86.
Unick JL, Hogan PE, Neiberg RH, Cheskin LJ, Dutton GR, Evans-Hudnall G et al. Evaluation of early weight loss thresholds for identifying nonresponders to an intensive lifestyle intervention. Obesity 2014; 22: 1608–1616.
Rissanen A, Lean M, Rossner S, Segal KR, Sjostrom L . Predictive value of early weight loss in obesity management with orlistat: an evidence-based assessment of prescribing guidelines. Int J Obes Relat Metab Disord 2003; 27: 103–109.
Finer N, Ryan DH, Renz CL, Hewkin AC . Prediction of response to sibutramine therapy in obese non-diabetic and diabetic patients. Diabetes Obes Metab 2006; 8: 206–213.
Prescribing Information: Belviq (lorcaserin hydrochloride) tablets. In: Eisai Inc., 2013.
Prescribing Information: Qsymia (phentermine and topiramate extended-release) capsule. In: Vivus, Inc., 2014.
Prescribing Information: Contrave (naltrexone HCl and bupropion HCl) Extended-release Tablets. In: Takeda Pharmaceuticals America, Inc., 2014.
Greenway FL, Fujioka K, Plodkowski RA, Mudaliar S, Guttadauria M, Erickson J et al. Effect of naltrexone plus bupropion on weight loss in overweight and obese adults (COR-I): a multicentre, randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2010; 376: 595–605.
Apovian CM, Aronne L, Rubino D, Still C, Wyatt H, Burns C et al. A randomized, phase 3 trial of naltrexone SR/bupropion SR on weight and obesity-related risk factors (COR-II). Obesity 2013; 21: 935–943.
Wadden TA, Foreyt JP, Foster GD, Hill JO, Klein S, O'Neil PM et al. Weight loss with naltrexone SR/bupropion SR combination therapy as an adjunct to behavior modification: the COR-BMOD trial. Obesity 2011; 19: 110–120.
Hollander P, Gupta AK, Plodkowski R, Greenway F, Bays H, Burns C et al. Effects of naltrexone sustained-release/bupropion sustained-release combination therapy on body weight and glycemic parameters in overweight and obese patients with type 2 diabetes. Diabetes Care 2013; 36: 4022–4029.
Colman E, Golden J, Roberts M, Egan A, Weaver J, Rosebraugh C . The FDA's assessment of two drugs for chronic weight management. N Engl J Med 2012; 367: 1577–1579.
Magkos F, Fraterrigo G, Yoshino J, Luecking C, Kirbach K, Kelly SC et al. Effects of moderate and subsequent progressive weight loss on metabolic function and adipose tissue biology in humans with obesity. Cell Metab 2016; 23: 591–601.
Moyer VA . US Preventive Services Task Force. Screening for and management of obesity in adults: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med 2012; 157: 373–378.
Fujioka K . Benefits of moderate weight loss in patients with type 2 diabetes. Diabetes Obes Metab 2010; 12: 186–194.
American College of Cardiology/American Heart Association Task Force on Practice Guidelines, Obesity Expert Panel, 2013. Expert panel report: Guidelines (2013) for the management of overweight and obesity in adults. Obesity 2014; 22 (Suppl 2): S41–S410.
Look Ahead Research Group, Pi-Sunyer X, Blackburn G, Brancati FL, Bray GA, Bright R et al. Reduction in weight and cardiovascular disease risk factors in individuals with type 2 diabetes: one-year results of the look AHEAD trial. Diabetes Care 2007; 30: 1374–1383.
Foster GD, Sanders MH, Millman R, Zammit G, Borradaile KE, Newman AB et al. Obstructive sleep apnea among obese patients with type 2 diabetes. Diabetes Care 2009; 32: 1017–1019.
Phelan S, Kanaya AM, Subak LL, Hogan PE, Espeland MA, Wing RR et al. Weight loss prevents urinary incontinence in women with type 2 diabetes: results from the Look AHEAD trial. J Urol 2012; 187: 939–944.
Williamson DA, Rejeski J, Lang W, Van Dorsten B, Fabricatore AN, Toledo K et al. Impact of a weight management program on health-related quality of life in overweight adults with type 2 diabetes. Arch Intern Med 2009; 169: 163–171.
Diabetes Prevention Program Research G, Knowler WC, Fowler SE, Hamman RF, Christophi CA, Hoffman HJ et al. 10-year follow-up of diabetes incidence and weight loss in the Diabetes Prevention Program Outcomes Study. Lancet 2009; 374: 1677–1686.
Acknowledgements
Medical writing assistance was provided by Sonja Billes, PhD.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
Clinical trials funded by: Orexigen Therapeutics, Inc., La Jolla, CA. The manuscript was supported by Orexigen and Takeda Pharmaceuticals International, Inc., Deerfield, IL. Ken Fujioka: Research grants from: Orexigen, Novo Nordisk, Enteromedics, Eisai, Takeda, and Weight Watchers. Consultant for: Novo Nordisk, Enteromedics, Zafgen, Eisai, Nazura, Takeda, and Isis. Speakers Bureau for: Abbott, NPS, Eisai, and Takeda. Patrick O'Neil: Research funding from: Orexigen, Weight Watchers, Novo Nordisk. Advisory Board for: Orexigen and Novo Nordisk. Honoraria from: Vivus, Eisai, Novo Nordisk, Medscape. Raymond Plodkowski: Research funding from: Orexigen, and Speakers Bureau for Takeda. Brandon Walsh: Employee and stockholder, Orexigen. Kye Gilder: Employee and stockholder, Orexigen. Frank Greenway: Consultant for: Basic Research, Eisai, General Nutrition Corporation, Neothetics, Obalon Therapeutics, Pam labs, Takeda, and Techenterprises. Scientific Advisory Board for: Baronova, Jenny Craig/Curves, Novo Nordisk, Orexigen, and Zafgen. Licensed patents with: Neuroquest. Stock options with Neothetics, and stock with OriginBiomed.
Additional information
Supplementary Information accompanies this paper on International Journal of Obesity website
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Fujioka, K., Plodkowski, R., O'Neil, P. et al. The relationship between early weight loss and weight loss at 1 year with naltrexone ER/bupropion ER combination therapy. Int J Obes 40, 1369–1375 (2016). https://doi.org/10.1038/ijo.2016.67
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/ijo.2016.67
This article is cited by
-
Individualised prescription of medications for treatment of obesity in adults
Reviews in Endocrine and Metabolic Disorders (2023)
-
RETRACTED ARTICLE: The best drug supplement for obesity treatment: a systematic review and network meta-analysis
Diabetology & Metabolic Syndrome (2021)
-
Mesolimbic opioid-dopamine interaction is disrupted in obesity but recovered by weight loss following bariatric surgery
Translational Psychiatry (2021)
-
Psychiatric adverse events and effects on mood with prolonged-release naltrexone/bupropion combination therapy: a pooled analysis
International Journal of Obesity (2019)
-
Issues in Measuring and Interpreting Human Appetite (Satiety/Satiation) and Its Contribution to Obesity
Current Obesity Reports (2019)

{kind=link}