
Abstract
Lead is neurotoxic at very low dose and there is a need to better characterize the impact of domestic sources of lead on the biological exposure of young children. A cross-sectional survey evaluated the contribution of drinking water, house dust and paint to blood lead levels (BLLs) of young children living in old boroughs of Montréal (Canada). Three hundred and six children aged 1 to 5 years and currently drinking tap water participated in the study. For each participant, residential lead was measured in kitchen tap water, floor dust, windowsill dust and house paint and a venous blood sample was analyzed. Multivariate logistic regression was used to evaluate the association between elevated BLL in the children (≥ 75th percentile) and indoor lead contamination by means of odds ratios (OR) using 95% confidence intervals (CI). There was an association between BLL ≥75th percentile (1.78 μg/dL) and water lead when the mean water concentration was >3.3 μg/L: adjusted OR=4.7 (95% CI: 2.1–10.2). Windowsill dust loading >14.1 μg/ft2 was also associated with BLL ≥1.78 μg/dL: adjusted OR=3.2 (95% CI: 1.3–7.8). Despite relatively low BLLs, tap water and house dust lead contribute to an increase of BLLs in exposed young children.
Similar content being viewed by others

Introduction
Lead is a known toxicant that can have health effects at very low levels, and young children are particularly vulnerable to its deleterious effects. Evidence of subtle neurotoxic effects at blood lead levels below 10 μg/dL have been reported.1, 2 Despite important actions to remove lead sources (such as leaded gasoline and lead soldering) from the general environment, lead exposure continues to be an important issue. Indoor sources of lead are still present in children’s surrounding environment and might contribute to low levels of exposure. This is particularly the case for sources such as house dust, paint or drinking water.3, 4
Lead service lines (pipes) and lead containing materials are well-known sources of drinking water contamination.5 However, the impact of low levels of lead contamination in drinking water has been rarely studied. Recently, two studies conducted in the Washington DC area6, 7 described the impact of lead service lines on BLLs of young children. However, because of limitations concerning the evaluation of children’s water exposure, their results could not precisely quantify the impact of lead from drinking water on BLLs.
Lead in paint and house dust remains an important source of lead exposure. In the United States, the contribution of old paint as a source of lead exposure for young children is well documented.8 Some cases of lead poisoning from paint have been described in Canada9 but no population study has yet evaluated the impact of lead-based paint on young children in a non point-source area. In the US, the importance of low-level house dust on BLLs of young children has been well demonstrated in an analysis of NHANES data.10 The importance of lead-based paint as a key cause for elevated indoor dust lead concentration was described in a recent nationally representative study of house dust in urban homes across Canada.11
As a number of sources are likely to be present simultaneously in the home environment, particularly in old houses, it is important to evaluate them at the same depth, in order to quantify their individual contributions. In fact, most of the studies done on the impact of these sources on BLLs of children have only considered one source6, 7, 10 or have evaluated one source in greater depth than the others.12
In 2005, moderate concentrations of lead were reported in tap water of Montréal households connected with lead service lines (LSLs).13, 14 The resulting potential increase of BLLs of young children was then estimated using the US EPA IEUBK model by the Montréal Public Health Department (MPHD) and found to be lower than the current Québec BLL notification level of 10 μg/dL.14 Since no case of lead poisoning related to drinking water was reported in the area and considering that many families were still using tap water for young children (despite advice from the MPHD to do the contrary), this site appeared highly suitable to quantify the impact of tap water exposure on BLLs and compare it to other lead sources.
The objective of this study was therefore to evaluate the impact of drinking water and other household sources of lead such as house dust and paint, on the BLLs of children aged 1–5 years and living in households where LSLs may still be present.
Materials and methods
General Methodology
This cross-sectional study simultaneously evaluated the BLLs and home indoor environment of young children (1 to 5 years of age) living in four boroughs of Montréal, selected for the possible presence of lead pipes and older houses. The study was carried out between September 2009 and March 2010.15 The ethics committees of the Center hospitalier universitaire de Québec and Health Canada approved the protocol developed for this study. Parents of children participating in the study provided their written informed consent prior to their participation.
Recruitment and Participant Selection
Following exclusion of industrial areas, a randomly selected list of 9,500 families, with at least one child aged 1 to 5 years and living in the targeted boroughs, was obtained from the Québec government’s health database (Régie de l’Assurance Maladie du Québec). After excluding families living in buildings with more than 3 dwellings, an information letter and a consent form were sent to 3,800 families living in the targeted boroughs. Only one child per family was pre-selected. The participant’s parents were contacted by telephone to verify the child’s eligibility and their willingness to participate in the study. Families meeting the following criteria were classified as eligible (n=549): the selected child consumes tap water regularly, was born in Canada, and was living in that dwelling for at least one year; he or she does not spend more than 2 days per week outside of the home or suffer from severe disease; the family should speak either French or English and does not use a water filtration device. Detailed frequencies of eligibility parameters for included and excluded families for this study are described and enumerated in Supplementary Materials (Supplementary Tables S1 and S2).
Home Visit
A trained environmental technician and a pediatric nurse visited each home. Following the completion of the consent form by one of the parents, the technician conducted a house inspection, water and dust sampling, and paint evaluation. The nurse interviewed the parents about their work and hobbies, the child’s health and habits (including water consumption and pica behavior) and drew a venous blood sample from the child’s arm.
Blood Sample
Venous blood was sampled in a 6 mL Becton-Dickinson tube (BD-367863) pre-treated with Ethylenediaminetetraacetic acid (EDTA) anticoagulant and kept at 4 °C until laboratory analysis. Whole blood samples were analyzed for lead content by Inductively Coupled Plasma Mass Spectometry (ICP-MS), using the Perkin Elmer Elan-6000 at the laboratory of the Institut National de Santé Publique du Québec (INSPQ, Québec, Canada). The detection limit was 0.02 μg/dL and the quantification limit was 0.08 μg/dL. Internal quality control was conducted using three reference materials obtained from the INSPQ (External Quality Assessment Schemes) (1.87 μg/dL, 6.25 μg/dL and 30 μg/dL). Duplicates performed every 10 analyses had a mean correlation coefficient of 0.992.
Tap Water
A total of 5 one-liter samples of cold kitchen tap water were collected in pre-acidified containers. The first liter was sampled following a 5 min flush (5M1L) at typical flow (5 to 7 L/min). After a 30-min stagnation period, 4 consecutive liters (30M1L, 30M2L, 30M3L, 30M4L) were sampled. Participants were asked not to use any source of water within their homes during the period of stagnation. The tap aerator was kept on during all sampling.
Samples were held at approximately 4 °C until analysis. Water lead analyses were performed using ICP-MS with Single Ion Monitoring (SIM) by an accredited environmental laboratory (Maxxam). The analysis protocol used was similar to that outlined in US EPA Method 200.816 with a slight increase in holding time of the acidified sample (i.e. increased from 16 to 24-h to enhance dissolution of particulate lead). The detection limit for the method was 0.01 μg/L and the quantification limit was 0.015 μg/L. Quality control was regularly performed during the analysis period (blank, certified reference material, duplicate, and fortified blank). The correlation coefficient for duplicates was 0.999. Results obtained for fortified blanks were within the limits used by this laboratory.
Dust
Floor dust was sampled from a selected sampling zone in the center of the available floor space in three different rooms in the home: the child’s room, home entrance and another room specified by the parents as frequently used by the child. A one square foot on smooth surface was sampled with a disposable wet wipe (Ghost wipes, Delta Scientific, #SC4250) following a standardized method (ASTM E-1728-03).17 Dust on the windowsill in the child’s room was collected with a separate wet wipe and sampling surfaces were measured to express results in μg/ft2. Each wet wipe was placed individually in plastic tubes and kept at 4 °C until laboratory analysis. To assure the absence of external contamination, two different wipe controls were used for each sampling zone: (1) a control wet wipe (in one out of every two residences,) was manipulated outside the plastic tube but without wiping on a surface and, (2) a template sampling using the regular protocol (once a week) on the interior surface of a template.
Analyses of the lead dust wipes consisted of predigesting the wet wipe in a partially covered 50 mL tube with 2 mL of concentrated nitric acid at room temperature for 5 h. The digestion tube was then placed in a bath at 80 °C for 12 h. Afterwards, the tube was withdrawn from the bath, and when it reached room temperature, 1 mL hydrochloric acid was added and a total volume of 10 mL was achieved by adding deionised water. Analysis was done by ICP-MS (Elan-6000, Perkin Elmer, Massachusetts, USA). Calibration was performed using aqueous standards. The detection limit was 0.01 μg and the quantification limit 0.015 μg per sample.
Paint
The lead content of the interior painted surfaces of homes was evaluated with a hand-held X-ray fluorescence (XRF) analyzer (Niton XLp300, Elemental Controls, Mississauga, Ontario, Canada). Sampling procedure, adapted from the US Department of Housing and Urban Development (US HUD),18 consisted of taking two consecutive 30-second measurements, a few centimetres apart. Where lead content was equal to or greater than 0.5 mg/cm2, a third measurement was performed for confirmation. Where there were different paints in one room, more than one wall was sampled. At least five rooms were assessed according to the child’s use and/or the level of deterioration of painted surfaces (child’s room, kitchen, family room, hallway and one other room commonly used by the child). The calibration of the XRF analyzer was verified 3 times before each home measurement with a standard reference material (Niton XLp300 Performance Characteristic Sheet 2004).
Where wall paint chips were present on damaged surfaces or flooring, they were collected for laboratory analysis. Approximately 200 mg of paint chips were necessary for lead analysis. Samples were digested at room temperature for 2 h in a partially covered test tube containing 2 mL of concentrated nitric acid. Afterwards, samples were covered and placed in an oven at 110 °C for 18 hours. Analyses were performed using ICP-MS method (Elan-6000, Perkin Elmer). Certified standard reference material paint chips from the National Institute of Standards and Technology (NIST 1579A) and demineralized water reference material from Ultra Scientific (ICM 240) were used for calibration and quality control. The detection limit was 10 μg/g and the quantification limit was 30 μg/g.
Statistical Analyses
BLL was considered both as a continuous and a categorical variable. When treated as a continuous variable, BLL measures are summarized as a geometric mean (GM) since the distribution of measurements is close to lognormal. When treated in categories, an elevated BLL was defined as a BLL equal or greater than the 75th percentile of measurements from the 306 participating children (≥1.78 μg/dL). Environmental exposure variables were treated in tertiles, except for paint where a qualitative division was used according to the XRF evaluation and the lead content of paint chips collected. Participants with missing values for windowsill dust were excluded from the analysis concerning only windowsill dust. Otherwise, these participants were pooled in a fourth category of windowsill dust: the “missing” category (the first 3 categories being the tertiles of the variable).
Two types of univariate analyses were performed in order to select variables to include in the multivariate logistic regression model for BLLs above the 75th percentile (with all exposure variables treated in categories). First, the GM of BLLs was calculated for each exposure variable (drinking water, dust and paint) and adjustment variables (listed below). For dichotomous variables, Student’s t-test of the blood lead logarithm was used to compare the means; for variables with three categories or more an analysis of variance was used. The source of difference between means, when a statistical difference was observed, was determined using Scheffe’s test for multiple comparisons. Chi-square tests were performed to determine variables with a significant relationship with elevated BLLs (≥1.78 μg/dL).
Exposure variables, adjustment variables with P-value ≤0.15 in one of the univariate analysis, or variables known to influence BLLs were included in the full multivariate logistic regression model after testing for multicollinearity (diagnostic of multicollinearity for variables with Variance Inflation Factor >2.5)19 (See Supplementary Material, Table S3). The adjustment variables were then withdrawn from the full model if their withdrawal did not change the OR of the exposure variables by more than 10%.
Possible modifying effects of seasons (fall or winter) and daycare use on exposure variables were then tested, as well as the interaction between the exposure variables. A tested effect was kept in the model if its P-value was <0.05. The adjustment variables included in the final multivariate logistic regression model were: age, ethnicity (Caucasian or not), season, parents' highest education level (one parent with a university degree), daycare use, health issue (chronic disease), exposure to second hand smoke, possible parental lead exposure from occupation or hobbies, and tap water consumption per kg of body weight (food and beverage consumption as reported by the parents). No modifying effects were found significant in the logistic regression model. The adjusted results are presented in two different ways. First, the model was run separately for each exposure variable and with all the adjustment variables (adjusted OR). Second, the model was run with all the exposure variables and all the adjustment variables (adjusted+OR). In this second model, the dust variables were included only for the evaluation of the effect of water and paint exposures.
SAS software version 9 for Windows (Copyright (c) 2002-2008 by SAS Institute Inc., Cary, NC, USA) was used to perform the statistical analyses. The statistical significance level for the multivariate analysis was set at 0.05.
Results
Participation Rate
Of the 3,800 families contacted by letter, 2,661 were reached by phone to verify their eligibility. Of the 549 eligible families identified, 313 (57%) accepted the invitation to participate in the study. Only 306 families were included in the data analysis, since no blood sample could be collected for 6 children, and one child was absent from their dwelling for an entire month prior to the home visit.
Participant Characteristics
The majority of participants were classified as Caucasian (i.e. not included in a visible minority group as defined by Statistics Canada20) and spoke French at home (Table 1). Most families owned the residence investigated and were highly educated, with 73% having at least one parent with a university degree. Only 5% of children had a severe risky behavior for lead exposure, defined as scratching, licking or gnawing soldered surfaces or paint. Most children were healthy, except a few (6%) who had moderate chronic disease such as asthma (data not shown). Daycare service was used by 75% of participants. Finally, only a few parents were evaluated as being possibly exposed to lead during their work (8%) or hobbies (10%).
Environmental Source of Exposure
The GM concentration of lead in the kitchen tap water was 0.89 μg/L after 5 min flushing (Table 2). The arithmetic mean (AM) of the 5 tap water samples (our main exposure variable) was first calculated for each sampling event. The GM of all sampling events was then determined to be 1.60 μg/L. The GM for each of the stagnation (30 M) samples was calculated and the highest mean concentration of lead in tap water was observed in the first liter after 30 min of stagnation (1.91 μg/L). Concentrations of total lead exceeded 10 μg/L in only 5 residences after 5 min of flushing and in 37 households after 30 min stagnation (data not shown).
The GM lead loading was 0.85 μg/ft2 for floor dust (AM of 3 samples) and 7.14 μg/ft2 for lead in windowsill dust. A total of 9 floor dust samples and 4 windowsill dust samples exceeded for a total of 12 residences the current US EPA regulatory requirements21 of 40 μg/ft2 for floor dust and 250 μg/ft2 for windowsill dust. Between one and 11 paint chips were collected from each residence for 157 participants. The median concentration of lead in paint chips was 1,300 mg/kg. Forty-two residences (27%) had lead concentrations higher than the 5,000 mg/kg US HUD guideline for paint chips (data not shown). Also, 31% of the residences evaluated had painted structures with 2 or more XRF measurements exceeding the 1 mg/cm2 US HUD guideline. Of these houses, 3% had more than 4 different painted structures exceeding the 1 mg/cm2 criteria. There was a weak, but significant (P<0.05) correlation between floor dust and windowsill (r=0.272) and floor dust and paint (r=0.214), as shown in Supplementary Material, Table S4.
Blood Lead Levels
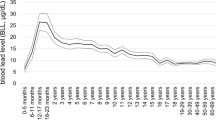
The GM concentration of BLLs for all children was 1.35 μg/dL (Table 3) and ranged from 0.37 μg/dL to 19.06 μg/dL. Only one child had a lead concentration above of the Québec notification level (10 μg/dL). Children classified in the non-Caucasian group had higher BLLs (1.53 μg/dL) compared to Caucasians (1.27 μg/dL), BLLs were higher in children of parents not holding a university diploma (1.52 μg/dL) compared to measurements of children where one or more parents had a university diploma (1.30 μg/dL). BLLs were higher in fall than in winter (1.50 μg/dL compared to 1.27 μg/dL) but no measurements were taken in either spring or summer. The differences in BLL concentrations between the above groups were statistically significant (P<0.05). Similar associations were found when considering children with elevated BLLs (Table 3).
Association of BLLs with Lead Indoor Contamination
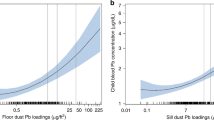
After adjusting for risk factors of elevated BLL, including ethnicity, season and water consumption, all four lead exposure variables were found to be associated with BLLs ≥75th percentile (Table 4). However, when the ORs were also adjusted for the other studied lead exposure variables (adjusted+), only the OR in the third tertiles of lead in tap water and lead in windowsill dust remained statistically significant: Adjusted+ OR for water=4.7, 95%CI: 2.1–10.2, and of windowsill dust (adjusted+ OR: 3.2, 95%CI: 1.3–7.8). A sensitivity analysis revealed that the relationship between water contamination and elevated BLLs was not different if we considered as the exposure variable: the 5 min flushed sample (OR=3.9; 95%CI: 1.8–8.6), the mean of the first and second liters after 30 min stagnation (OR=4.5; 95%CI: 2.0–10.0) or the mean of the third and fourth liters after stagnation (OR=3.7; 95%CI: 1.7–7.9) (See Supplementary Material, Supplementary Table S5). This relationship was similar after stratifying the participants by season of sampling but this was not the case for the other exposure variables where the relationship with elevated BLL was mostly present only during winter (See Supplementary Material, Supplementary Table S6). However, no significant statistical interactions were found between those variables and the season.
Discussion
Lead exposure in children remains an important issue. Given the reduction of lead exposure via external sources such as gasoline, the impact of indoor sources might be relatively more important nowadays. Our results appear to demonstrate that even with a very low background of lead exposure, and low contamination in the home environment, sources such as water and home dust can still have a detectable impact on the BLLs of young children.
Lead Indoor Contamination
Results obtained for fall and winter sampling showed low lead concentrations in kitchen tap water for the majority of participants, with a mean concentration of 1.60 μg/L which is well below the Québec standard of 10 μg/L and lower than water concentrations reported in earlier BLLs studies.6, 22 The lead loading of residential house dust was low but comparable to results from similar studies. In particular, the lead loading of house dust in our study was consistent with values recently reported in the large 2007-2008 NHANES database with mean lead loads in floor and windowsill dust of 0.52 and 7.64 μg/ft2 respectively.23 Our dust results are slightly higher than those found in another Canadian study reporting that 3 out of 222 houses located in Ontario had lead content of floor dust wipes exceeding the US EPA criteria21 of 40 μg/ft2 (compared to 9/306 in our study).24
Lead-based paint was frequently present in older houses (built in 1920–1949) in our study. In particular, about 27% of our participants were exposed to paint chips containing ≥5,000 mg/kg lead and 31% were living in houses with painted structures exceeding the US HUD criteria of 1 mg/cm2, as analyzed by XRF. These measured concentrations are similar to those reported in other North American studies25, 26 but higher than those observed by Lanphear et al.27 Lead paint contamination is a common source of indoor dust lead contamination which is supported in this study by a weak correlation between lead in paint and house dust (See Supplementary Material, Supplementary Table S4).
BLLs and their Relationship with Indoor Contamination
Blood lead levels found in the studied children were low and comparable to those reported recently in North America. For instance, in the 2007-2008 NHANES study, the geometric mean of the BLL of 817 children aged 1–5 years was estimated to be at 1.5 μg/dL,28 which compares with results from this study, and in particular to results from the fall period.
Despite the low levels of contamination, we report an impact of the indoor environment on BLLs of young children, which is especially significant for very moderate lead contamination in tap water (>3.27 μg/L) and windowsill dust (>14.14 μg/ft2). The relationship with water contamination was the most robust and remains significant when the different types of water samples were considered. The contribution of lead contamination in water to BLL has been studied previously, mostly in populations exposed to higher lead concentrations.5 In Washington, DC, Brown et al.7 assessed the impact of the presence of LSLs and of changes in the type of disinfectant used (chlorine vs chloramines) to the BLLs of young children between the years 1986 and 2006. They reported that children aged 0–3 years served by a LSL were more likely to be situated in the upper fourth quartile of BLLs, especially during peak lead release periods. Important differences hinder the direct comparison of our results with those from Brown et al.7 First and foremost, tap water and BLL samples were not paired at the individual level as in this study. Furthermore, tap water samples were collected using different protocols (greater stagnation time of 6 hours) which typically increases the lead concentration in analyzed water samples.
The impact of house dust moderately contaminated by lead was clearly demonstrated in this study for children living in homes with elevated dust lead loadings on window sills >14.14 μg/ft2 and to a lesser extend on floors (>1.22 μg/ft2). Our results are in agreement with those of the 1999-2004 NHANES data presented by Dixon et al.10 In the NHANES study, BLLs of children (at levels ≥5 μg/dl and 10 μg/dl) aged 1–2.5 years living in pre-1978 housing were associated with a dose-response with lead load of floor house dust ranging from about 0.5 μg/ft2 to about 40 μg/ft2.10 However, despite similarities between our study and the Dixon study, we should consider that the latter study used only one floor wipe sample which may have contributed to greater measurement uncertainty with respect to dust lead loading.
The impact of leaded paint (the presence of paint chips with lead load ≥5,000 mg/kg) on elevated BLLs was also demonstrated in this study, although this association did not remain statistically significant when considering other lead exposures from tap water and dust. However, possible over-adjustment is acknowledged due to the likely contribution of lead paint to floor dust. Leaded paint is still considered as a major source of lead poisoning in young children.9, 29 Other associations between leaded paint and elevated BLLs of young children have been observed in Chicago children,30 but not in the Rochester study.27
Limits
Despite its strengths (no point source of lead in the selected boroughs, indoor lead-targeted boroughs, systematic recruitment, in-depth evaluation of the major components of residential exposure and high quality control for data collection and laboratory measurements), our study has some limitations that should be discussed. In particular, due to its cross-sectional design, this study was not able to evaluate the precise environmental exposures which occurred in the months before obtaining a child’s blood sample. Since the half-life of BLL is about one month,31 the effect of the recent exposure history is particularly important. Seasonal variations relate to both environmental exposure to lead;32, 33 and to the tendency for BLLs to be higher in warmer period (e.g. summer).32, 34 This is partly reflected in this study by the higher BLLs observed during the fall season compared to winter. However, a Supplemental analysis demonstrated that, despite higher BLLs in the fall, the association between lead in tap water and elevated BLLs measured by the OR was quite stable in both studied seasons. However, this was not the case for the other studied exposures. We could not identify precisely the levels of home contamination that occurred during the summer season and its association with elevated BLLs. We also did not take into account the exposure that could occur outside the home as well as the direct or indirect effect of nutrition status.
Conclusion
The results of this study demonstrate that, despite relatively low contamination, all the lead exposure sources in the domestic environment that we have evaluated (water, dust, and paint) contribute to the elevation of BLLs in children of 1 to 5 years of age, living in targeted areas of Montréal. Dust and paint were well known contributors to lead poisoning in the past and their effect on BLLs of children is still present. Drinking water flowing through lead service lines is not a negligible source of exposure to lead and may be a persistent significant contributor to children’s BLL. Given the absence of a known health effects threshold for exposure to lead, studies on risk factors and drivers of exposure in groups of children with low exposure are still important to guide strategies for further reducing low-level exposures to lead.
Abbreviations
- AM:
-
Arithmetic mean
- BLL:
-
Blood Lead Level
- CI:
-
Confidence interval
- GM:
-
Geometric mean
- OR:
-
Odds ratio
- 5M1L:
-
First liter after 5 min flushing
- 30M1L:
-
First liter after 30 min stagnation
- 30M2L:
-
Second liter after 30 min stagnation
- 30M3L:
-
Third liter after 30 min stagnation
- 30M4L:
-
Fourth liter after 30 min stagnation
References
Lanphear BP, Hornung R, Khoury J, Yolton K, Baghurst P, Bellinger DC et al Low-level environmental lead exposure and children’s intellectual function: an international pooled analysis. Environ Health Perspect 2005; 113: 894–899.
Gilbert SG, Weiss B . A rationale for lowering the blood lead action level from 10 to 2 microgr/dL. Neurotoxicology 2006; 27: 693–701.
Ryan D, Levy B, Levy BS, Pollack S, Walker B . Protecting children from lead poisoning and building healthy communities. Am J Public Health 1999; 89: 822–824.
Lanphear BP, Hornung R, Ho M, Howard CR, Eberly S, Knauf K . Environmental lead exposure during early childhood. J Pediatr 2002; 140: 40–47.
Triantafyllidou S, Edwards M . Lead (Pb) in Tap Water and in Blood: Implications for Lead Exposure in the United States. Crit Rev Environ Sci Technol 2012; 42: 1297–1352.
Edwards M, Triantafyllidou S, Best D . Elevated blood lead in young children due to lead-contaminated drinking water: Washington, DC, 2001-2004. Environ Sci Technol 2009; 43: 1618–1623.
Brown MJ, Raymond J, Homa D, Kennedy C, Sinks T . Association between children’s blood lead levels, lead service lines, and water disinfection, Washington, DC, 1998-2006. Environ Res 2011; 111: 67–74.
Jacobs DE, Clickner RP, Zhou JY, Viet SM, Marker DA, Rogers JW et al The prevalence of lead-based paint hazards in US housing. Environ Health Perspect 2002; 110: A599–A606.
Lavoie PM, Bailey B . Lead poisoning from “lead-free” paint. CMAJ 2004; 170: 956.
Dixon SL, Gaitens JM, Jacobs DE, Strauss W, Nagaraja J, Pivetz T et al Exposure of US children to residential dust lead, 1999-2004: II. The contribution of lead-contaminated dust to children's blood lead levels. Environ Health Perspect 2009; 117: 468–474.
Rasmussen PE, Beauchemin S, Chénier M, Levesque C, MacLean LC, Marro L et al Canadian house dust study: lead bioaccessibility and speciation. Environ Sci Technol 2011; 45: 4959–4965.
Lanphear BP, Weitzman M, Winter NL, Eberly S, Yakir B, Tanner M et al Lead-contaminated house dust and urban children's blood lead levels. Am J Public Health 1996; 86: 1416–1421.
Cartier C, Laroche L, Deshommes E, Nour S, Richard G, Edwards M et al Investigating dissolved lead at the tap using various sampling protocols. J Am Water Works Assoc 2011; 103: 55–67.
Beausoleil M, Brodeur J . Le plomb dans l'eau potable sur l'île de Montréal. État de la situation et évaluation des risques à la santé. Direction de santé publique. Agence de la santé et des services sociaux de Montréal. 2007 Available http://publications.santemontreal.qc.ca/uploads/tx_asssmpublications/978-2-89494-620-6.pdf [last accessed 16 January 2012].
Levallois P, St-Laurent J, Gauvin D, Courteau M . Étude de l'impact de la contamination par le plomb de l'environnement résidentiel sur la plombémie des jeunes enfants. Report presented to Health Canada. Institut national de santé publique du Québec. 2011.
US EPA (US Environmental Protection Agency). Determination of trace elements in waters and wastes by inductively coupled plasma - mass spectrometry. Method 200.8. Revision 5.4. EMMC Version 1994.
ASTM. Standard practice for collection of settled dust Samples wipe sampling methods for subsequent lead determination, ASTM E-1728. -03. West Conshohocken, PA: ASTM International. 2003.
US HUD (US Department of Housing and Urban Development). Guidelines for the evaluation and control of lead-based paint hazards in housing. Office of Lead-Based Paint Abatement and Poisoning Prevention 1995 Available http://portal.hud.gov/hudportal/HUD?src=/program_offices/healthy_homes/lbp/hudguidelines [last accessed 20 January 2012].
Allison PD . Logistic Regression Using the SAS*System: Theory and Application. SAS Institute: Cary, NC. 1999.
Statistics Canada Ethnic origin and visible minorities, 2006 Census. Catalogue no. 97-562-GWE2006025. Release no. 7: April 2 2008 Available: http://www12.statcan.ca/census-recensement/2006/rt-td/eth-eng.cfm [accessed 20 September 2011].
US EPA (US Environmental Protection Agency) Lead: Identification of dangerous levels of lead; Finale rule, Federal register part III (40CFR part 745) 2001; 66: 1206–1240.
CDC (Centers for Disease Control and Prevention). Blood lead levels in residents of homes with elevated lead in tap water - District of Columbia. MMWR Morb Mortal Wkly Rep 2004; 53: 268–270.
Gaitens JM, Dixon SL, Jacobs DE, Nagaraja J, Strauss W, Wilson JW et al Exposure of US children to residential dust lead, 1999-2004: I. Housing and demographic factors. Environ Health Perspect 2009; 117: 461–467.
McDonald LT, Rasmussen PE, Chenier M, Levesque C . Extending wipe sampling methods to the elements other than lead. J Environ Monit 2011; 13: 377–383.
Scott RE . Residential Sources of Lead. Canada Mortgage and Housing Corporation, NH15-131/1995E 1995.
Stroop DM, Dietrich KN, Hunt AN, Suddendorf LR, Giangiacomo M . Lead-based paint health risk assessment in dependent children living in military housing. Public Health Rep 2002; 117: 446–452.
Lanphear BP, Burgoon DA, Rust SW, Eberly S, Galke W . Environmental exposures to lead and urban children's blood lead levels. Environ Res 1998; 76: 120–130.
CDC (Centers for Disease Control and Prevention). Fourth National Report on Human Exposure to Environmental Chemicals, Updated Tables. 2011. Available www.cdc.gov/exposurereport/pdf/Updated_Tables.pdf [accessed 15 October 2011].
O'Grady K . Perron Al. Reformulating Lead-Based Paint as a Problem in Canada. Am J Public Health 2011; 101: S176–S187.
Schwartz J, Levin R . The risk of lead toxicity in homes with lead paint hazard. Environ Res 1991; 54: 1–7.
ATSDR (Agency for Toxic Substances and Disease Registry). Toxicological profile for lead. Atlanta, GA: US Department of Health and Human Services, Public Health Service. 2007.
Yiin LM, Rhoads GG, Lioy PJ . Seasonal influences on childhood lead exposure. Environ Health Perspect 2000; 108: 177–182.
Petrosyan V, von Braun MC, Spalinger SM, von Lindern IH . Seasonal variations of lead concentration and loading rates in residential house dust in northern Idaho. J Hazard Mater 2006; 132: 68–79.
Haley VB, Talbot TO . Seasonality and trend in blood lead levels of New York State children. BMC Pediatr 2004; 4: 8.
Acknowledgements
This research was funded by the Chemicals Management Plan of Health Canada, the Canadian Water Network and the Ministère de la Santé et des Services sociaux du Québec. During the study, researchers of this project received recommendations from an advisory committee composed of: Marc Edwards, Professor at Virginia Tech University, Bruce Lanphear, Professor at Simon Fraser University, Howard Shapiro, Associate Medical Officer of Health at the City of Toronto, and Robert Tardif, Professor at Université de Montréal. We thank Annick Trudelle for the coordination of the field study, Natacha Fontaine-Seguin, Dominique Dubreuil, and Catherine Patoine-Bossé, environmental hygienists for the environmental evaluation. We also thank the nurses from Alternacare Inc., Alain Leblanc and Alain Beaudet from the INSPQ laboratory, and the participant families for their important collaboration which was essential to the success of this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
Supplementary Information accompanies the paper on the Journal of Exposure Science and Environmental Epidemiology website
Supplementary information
Rights and permissions
This work is licensed under the Creative Commons Attribution-NonCommercial-No Derivative Works 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/3.0/
About this article
Cite this article
Levallois, P., St-Laurent, J., Gauvin, D. et al. The impact of drinking water, indoor dust and paint on blood lead levels of children aged 1–5 years in Montréal (Québec, Canada). J Expo Sci Environ Epidemiol 24, 185–191 (2014). https://doi.org/10.1038/jes.2012.129
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/jes.2012.129
Keywords
This article is cited by
-
Repeated home drinking water sampling to improve detection of particulate lead spikes: a simulation study
Journal of Exposure Science & Environmental Epidemiology (2023)
-
A national survey of lead and other metal(loids) in residential drinking water in the United States
Journal of Exposure Science & Environmental Epidemiology (2023)
-
Lead contamination of public drinking water and academic achievements among children in Massachusetts: a panel study
BMC Public Health (2022)
-
Determinants of blood and saliva lead concentrations in adult gardeners on urban agricultural sites
Environmental Geochemistry and Health (2022)
-
A new screening index to better target low-level lead exposure in Atlanta, Georgia
Scientific Reports (2020)
