
Abstract
The impact of the COVID-19 pandemic on clinically stable older patients with psychiatric disorders is unclear. This study examined the prevalence of depressive and anxiety symptoms, and their associations with quality of life (QOL) in clinically stable older patients with psychiatric disorders during the COVID-19 pandemic. This was a multicenter, cross-sectional study. Depressive and anxiety symptoms, insomnia, pain, and QOL were assessed with standardized instruments. A total of 1063 patients were included. The prevalence of depressive and anxiety symptoms, and combined depressive and anxiety symptoms were 62.3% (95%CI = 59.4–65.2%), 52.4% (95%CI = 49.3–55.4%), and 45.9% (95%CI = 42.9–48.9%), respectively. Patients with depressive and anxiety symptoms had significantly lower QOL than those without (P < 0.01). Binary logistic regression analyses revealed that having depressive symptoms was positively associated with more severe insomnia (OR = 1.29, P < 0.01) and pain (OR = 1.14, P < 0.01), and was negatively associated with other psychiatric diagnoses (except for major depressive disorder, schizophrenia, and organic mental disorder; OR = 0.50, P < 0.01), while having anxiety symptoms was positively associated with severe physical diseases (OR = 1.57, P = 0.02), poor adherence to treatment (OR = 1.50, P < 0.01), and more severe insomnia (OR = 1.15, P < 0.01) and pain (OR = 1.11, P < 0.01). Having combined depression and anxiety symptoms was positively associated with poor adherence to treatment (OR = 1.42, P = 0.02) and more severe insomnia (OR = 1.19, P < 0.01) and pain (OR = 1.15, P < 0.01), and was negatively associated with the diagnosis of schizophrenia (OR = 0.50, P = 0.04) and others (OR = 0.53, P < 0.01). Depressive and anxiety symptoms were common in clinically stable older patients with psychiatric disorders during the COVID-19 pandemic. Considering the negative impact of these symptoms on QOL, regular screening and appropriate treatment are recommended for this population.
Similar content being viewed by others
Introduction
As of late July 2020, the Coronavirus Disease 2019 (COVID-19) pandemic has caused ~1 million deaths out of >39 million confirmed cases1. Compared to other age groups, older adults are more vulnerable during the COVID-19 pandemic2. For instance, older patients with COVID-19 (>50 years) have considerably higher fatality rate3 and poorer treatment outcomes4,5, which could exacerbate fear and psychological distress due to COVID-19.
Of older adults, those with preexisting psychiatric disorders need greater attention due to the high risk of mental health problems during the COVID-19 pandemic6,7. To reduce the risk of disease transmission, some preventive measures, such as quarantine and travel restriction, could trigger or worsen mental health status in older persons with psychiatric problems7. For instance, clinically stable older patients with psychiatric disorders usually require long-term maintenance pharmacotherapy. Due to lack of primary mental health services in most areas of China, it is necessary for clinically stable patients to regularly attend psychiatric clinics in urban areas for follow up and medication prescriptions8,9. However, as a result of quarantine and travel restriction, patients had difficulties attending hospitals, which may trigger mental health problems, such as depression and anxiety. In addition, older psychiatric patients usually suffer from chronic physical diseases, such as cardiovascular diseases and metabolic disease, which also require long-term medical reviews. Limited access to health services could result in deterioration of their physical diseases and increase their risk of mental health problems.
Depressive and anxiety symptoms (depression and anxiety hereafter) are common mental health problems in older psychiatric patients10. These are frequent comorbidities11,12 that are associated with poor prognosis13, cognitive impairment14,15, physical distress16,17, and social disability12. Even though more attention should be given to depression and anxiety in older psychiatric patients during the COVID-19 pandemic, no relevant studies have been published to date.
A better understanding of the patterns of depression and anxiety is needed to develop appropriate preventive measures and effective treatments for older patients with psychiatric disorders during the COVID-19 pandemic. In addition, quality of life (QOL) is a comprehensive health outcome that reflects individuals’ subjective perception of their overall health status. However, the association of depression and anxiety with QOL in older patients with psychiatric disorders is not clear. Therefore, we conducted this study to examine the prevalence of depression and anxiety, and their associations with QOL among clinically stable older patients with psychiatric disorders during the COVID-19 pandemic. We hypothesized that depression and anxiety were common among clinically stable older patients with psychiatric disorders during the COVID-19 pandemic, and these would have a negative impact on patients’ QOL.
Methods
Study sites and participants
This was a cross-sectional study conducted between May 22 and July 15, 2020, in four major tertiary psychiatric hospitals in the eastern (Jiangsu province), southern (Fujian province), western (Gansu province), and northern (Beijing) China, which could represent a wide range of clinical settings in China. Older psychiatric patients receiving maintenance treatments in the outpatient departments of the four hospitals were consecutively invited to participate in the survey, if they met the following criteria: (1) diagnosed with psychiatric disorders according to the International Statistical Classification of Diseases and Related Health Problems, 10th Revision (ICD-10)18; (2) older adults aged 50 years and above19,20; and (3) clinically stable as assessed by their treating psychiatrists, and able to understand the purpose and procedures of the assessments. Following previous studies21,22, “clinically stable patients” were defined as those who had changes in their dose of psychotropic medications of <50% in the past 3 months. This definition was also consistent with the clinical practice in the participating hospitals. Older patients and their guardians (if available) who regularly attended the outpatient clinics for maintenance therapy in each participating hospital were invited by a research psychiatrist with the approval from their treating psychiatrists to participate in this study. After providing their written informed consent on site in the outpatient department of the participating hospitals, they subsequently completed the online assessment using their smartphone. The study protocol was approved by the ethical committees of the participating hospitals.
The sample size was calculated with the following formula23: N = (Zα2 × P × (1–P))/d2. The confidence level (Z) is equals to 1.96 at significance level of α = 0.05, P was the estimated proportion, and d is the tolerated margin of error and was calculated with 0.1 × P. A previous study has found that the prevalence of depression and anxiety were 27.9% and 31.6%, respectively, in the general population24. In order to achieve sufficient statistical power, we used P = 0.279 to calculate the sample size. Assuming 10% of patients who would refuse the invitation, 1000 patients were needed in this study.
Data collection and measurements
Due to the potential risk of transmission and logistical reasons during the COVID-19 pandemic, face-to-face interviews could not be performed. Following other studies25,26,27, data were collected using the WeChat-based “Questionnaire Star” program. The WeChat is a social communication program in smartphone with >1 billion users in China. As part of the process of receiving treatments at the participating hospitals, all patients (and/or their guardians) receiving maintenance treatments in the participating outpatient departments were WeChat users. For patients who had difficulties in use of smartphone, the research psychiatrists assisted them to complete the assessment using patients’ or their guardians’ smartphone.
The basic sociodemographic and clinical data (e.g., age, gender, education years, marital status, living area, and presence of severe physical diseases) were collected. Questions with a “yes/no” option were used to collect COVID-19-related data, i.e., “whether or not they were concerned about the COVID-19 pandemic-related information”, “whether or not they frequently used mass media for COVID-19-related information”, “whether or not they had difficulty accessing their psychiatrists during the COVID-19 pandemic”, “whether or not they were adherent to psychiatric treatment during the COVID-19 pandemic”, and “whether or not they had difficulty attending psychiatric hospitals due to the COVID-19 pandemic restrictions”.
Depression was evaluated using the validated Chinese version of the nine-item Patient Health Questionnaire (PHQ-9)28,29, which has been widely used in clinical research with a total score ranging from 0 to 2730. A PHQ-9 total score of ≥5 was considered as “having depression”, and ≥10 was considered as “having moderate to severe depression”31. The severity of anxiety was assessed using the generalized anxiety disorder (GAD-7)32,33, with the total score ranging from 0 to 21. A GAD-7 total score of ≥5 was considered as “having anxiety”, and ≥10 was considered as “having moderate to severe anxiety”32. Patients with both PHQ-9 total score of ≥5 and GAD-7 total score of ≥5 were considered as “having combined depression and anxiety”.
The severity of insomnia symptoms (insomnia hereafter) was assessed by the seven-item Insomnia Severity Index (ISI)34, which has been translated and validated in Chinese populations35. The ISI total score ranges from 0 to 28 with a higher total score indicating more severe insomnia. Those with an ISI total score ≥8 were considered “having insomnia symptoms”36. The severity of pain was evaluated using the “0–10” numeric rating scale on pain37,38, with “0” representing “no pain at all” and “10” representing “unbearable pain”39. The overall QOL was measured using the sum of the first two item scores of the World Health Organization Quality of Life-brief version (WHOQOL-BREF)40,41,42, with a higher score representing higher QOL.
Data analysis
Data were analyzed using the Statistic Package for Social Science (SPSS) version 24.0. The normality of continuous variables was tested, using the P–P plot. The demographic and clinical variables were compared between depression and no depression groups, between anxiety and no anxiety groups, and between combined anxiety and depression and no anxiety or depression groups, respectively. Specifically, χ2 test was used to compare categorical variables, while two independent samples t test and Mann–Whitney U test were used to compare normally and non-normally distributed continuous variables, respectively. The association between depression and anxiety were examined with Spearman’s rank-order correlation analysis.
Binary logistic regression analyses with the “enter” method were performed to examine the independent correlates of depression, anxiety, and comorbid anxiety and depression, respectively. All variables with significant group differences in univariate analyses were entered as independent variables, while depression, anxiety, and combined anxiety and depression were entered as the dependent variable separately. The independent associations of depression, anxiety, and comorbid anxiety and depression with QOL were examined using analysis of covariance (ANCOVA) after controlling for variables with significant group differences in univariate analyses. The significance level was set at P < 0.05 (two-tailed).
Results
Social-demographic and clinical characteristics
Altogether, 1068 patients were invited to participate in the survey during the predefined study period. Finally, 1063 met the eligibility criteria and were included, giving a response rate of 99.5%. The sociodemographic and clinical characteristics of the participants were presented in Table 1. The mean age of participants was 62.8 (standardized deviation (SD) = 9.4) years and 32.6% (n = 347) of the total sample were males.
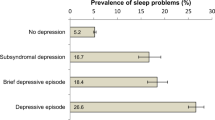
The prevalence of the overall depression (PHQ total score ≥5) was 62.3% (95%CI = 59.4–65.2%), while the prevalence of moderate to severe depression (PHQ total score ≥10) was 30.8% (95%CI = 28.0–33.6%). The mean total score of PHQ-9 was 7.75 (SD = 6.73). The prevalence of the overall anxiety (GAD-7 total score ≥5) was 52.4% (95%CI = 49.3–55.4%), while the prevalence of moderate to severe anxiety (GAD-7 total score ≥10) was 25.6% (95%CI = 23.0–28.3%). The mean total score of GAD-7 was 5.95 (SD = 5.76). Spearman’s rank-order correlation analysis revealed that depression and anxiety had a significant correlation (correlation coefficient = 0.73, P < 0.01). The prevalence of combined depression and anxiety was 45.9% (95%CI = 42.9–48.9%). The prevalence of insomnia (ISI total score ≥8) was 56.9% (95%CI = 53.9–59.9%).
Univariate analyses
Univariate analyses revealed that patients with depression were more likely to live in rural areas (P < 0.01), suffer from severe physical diseases (P = 0.03), and have lower education level (P = 0.02), poor treatment adherence (P < 0.01), and difficulty attending psychiatric hospitals (P < 0.01) during the COVID-19 pandemic, and suffer from more severe insomnia (P < 0.01) and pain (P < 0.01). The prevalence of depression was significantly different across different psychiatric diagnoses (P < 0.01) (Table 1).
Patients with anxiety were more likely to live in rural area (P < 0.01), suffer from severe physical diseases (P < 0.01), have poor treatment adherence (P < 0.01), and difficulty attending psychiatric hospitals (P = 0.01) during the COVID-19 pandemic, and have more severe insomnia (P < 0.01) and pain (P < 0.01). The prevalence of anxiety was significantly different across different psychiatric diagnoses (P < 0.01) (Table 1).
Patients with combined depression and anxiety were more likely to live in rural areas (P < 0.01), suffer from severe physical diseases (P < 0.01), have poor treatment adherence (P < 0.01), and difficulty attending psychiatric hospitals (P < 0.01) during the COVID-19 pandemic, and have more severe insomnia (P < 0.01) and pain (P < 0.01). The prevalence of combined depressive and anxiety symptoms was significantly different across different psychiatric diagnoses (P < 0.01) (Table 1).
Multivariate analyses
Table 2 presents the results of binary logistic regression analyses. Depression was positively associated with more severe insomnia (OR = 1.29, 95%CI = 1.24–1.34, P < 0.01) and pain (OR = 1.14, 95%CI = 1.03–1.25, P < 0.01), and was negatively associated with other psychiatric diagnoses (except for major depressive disorder, schizophrenia, and organic mental disorder; OR = 0.50, 95%CI = 0.35–0.71, P < 0.01). Anxiety was positively associated with severe physical diseases (OR = 1.57, 95%CI = 1.05–2.35, P = 0.02), poor adherence to treatment (OR = 1.50, 95%CI = 1.11–2.03, P < 0.01), and more severe insomnia (OR = 1.15, 95%CI = 1.12–1.18, P < 0.01) and pain (OR = 1.11, 95%CI = 1.02–1.20, P < 0.01). Combined depression and anxiety were positively associated with poor adherence to treatment (OR = 1.42, 95%CI = 1.03–1.95, P = 0.02), and more severe insomnia (OR = 1.19, 95%CI = 1.16–1.23, P < 0.01) and pain (OR = 1.15, 95%CI = 1.06–1.25, P < 0.01), and was negatively associated with schizophrenia (OR = 0.50, 95%CI = 0.26–0.97, P = 0.04) and other psychiatric diagnoses (except for major depressive disorder, schizophrenia, and organic mental disorder; OR = 0.53, 95%CI = 0.38–0.73, P < 0.01) (Table 2).
ANCOVA revealed that patients with depression had significantly lower overall QOL compared to those without depression (F(1, 1063) = 36.11, P < 0.01), while patients with anxiety had significantly lower overall QOL compared to those without anxiety (F(1, 1063) = 40.35, P < 0.01), and patients with combined depression and anxiety had significantly lower overall QOL compared to those without depression and anxiety (F(1, 1063) = 51.85, P < 0.01).
Discussion
This was the first study that examined depression and anxiety in clinically stable older patients with psychiatric disorders during a pandemic. The prevalence of depression (62.3%) and anxiety (52.4%) in this study were higher than the corresponding figures in adolescents (depression: 43.7%; anxiety: 37.4%)43 and in the general population (depression: 27.9%; anxiety: 31.6%%)24 in China, using the same measurements during the COVID-19 pandemic. This high prevalence of depression and anxiety in older psychiatric patients could be partly due to the fear of high mortality rate and poor prognosis in older people infected with COVID-193,4,5, which leads to considerable psychological distress in older population. Furthermore, many older psychiatric patients suffer from comorbid impaired cognitive function44,45,46,47, which may cause difficulties to understand and process COVID-19-related information, resulting in depression and anxiety48. In addition, the quarantine and travel restrictions during the COVID-19 pandemic did not only create barriers to access health services, but also cause disruptions to regular daily life and activities, all of which could increase the risk of depression and anxiety49.
In this study, comorbid depression and anxiety were not only common (45.9%, 95%CI = 42.9–48.9%) among participants, but also significantly correlated with each other, which is consistent with previous findings11,13,50. The association between depression and anxiety is bidirectional; anxiety can trigger depression51 and vice versa52. The co-occurrence of depression and anxiety may be related to alteration of activation and connectivity of ventral cingulate and amygdala, and the polymorphic variations in the serotonin receptor gene53,54.
Patients with depression and/or anxiety reported more severe insomnia. The association between insomnia and psychiatric disorders is complex. On the one hand, insomnia can increase the risk of psychiatric disorders, including depression and anxiety55,56. For instance, a meta-analysis found that insomnia is a major risk factor of depression (OR = 2.83, 95%CI = 1.55–5.17) and anxiety (OR = 3.23, 95%CI = 1.52–6.85)56. On the other hand, depression and anxiety can also contribute to the development of insomnia57,58. Comorbid insomnia and psychiatric disorders may share common pathophysiology, such as similar alterations of arousal states59 and levels of inflammatory markers60.
Depression and anxiety were associated with more severe pain in this study. Chronic pain (e.g., headache and musculoskeletal pain) is common in older population61, and has a negative impact on QOL, sleep quality, and social functioning62. Previous studies found that certain psychiatric disorders (e.g., depression and anxiety) and pain commonly coexisted63, with bidirectional associations64,65,66,67.
We found that anxiety and combined depression and anxiety was positively associated with poor treatment adherence, which is consistent with previous findings that patients with anxiety were more likely to discontinue their medication treatment due to side effects68, or their psychological interventions due to low motivation and poor therapeutic alliance69. The positive association between anxiety and comorbid severe physical diseases (e.g., cardiac vascular diseases, gastrointestinal diseases, and genitourinary disorders) could be due to relevant to various factors, including physical distress, medication-induced side effects, and treatment cost16,70,71,72. In this study, patients with schizophrenia and other psychiatric disorders, except for major depressive disorder and organic mental disorder, were less likely to have combined depressive and anxiety symptoms, while patients with other psychiatric disorders, except for major depressive disorder and organic mental disorder, were less likely to have depressive symptoms alone during the COVID-19 pandemic. However, it is noteworthy that there were only 73 schizophrenia patients and 63 patients with organic mental disorders; therefore, the associations between primary psychiatric diagnoses and psychiatric symptoms during the COVID-19 pandemic needs to be confirmed in future head-to-head comparative studies.
As expected, patients with depression and anxiety had lower QOL than those without. QOL is determined by the interaction between protective factors (e.g., better social support and higher financial level) and distressing factors (e.g., poor mental health and physical conditions)73. Depression and anxiety were associated with cognitive dysfunction14,15, physical distress16,17, and impaired social functioning12, which could lower patients’ QOL.
The strengths of this study included the large sample size, consecutive sampling, high participation rate, and multicenter study design. However, several limitations need to be addressed. First, this study only recruited clinically stable patients from outpatient departments, which could limit the generalization of the findings to those in acute illness phase. Second, due to the cross-sectional study design, the causal relationships between depression/anxiety and other variables could not be examined. Third, some factors associated with depression and anxiety, such as cognitive function15,74, and type and dose of psychotropic medications17, were not assessed in this study due to logistical reasons. Fourth, COVID-19-related information was assessed with self-reported standardized questions. The results of relevant objective measures would be more reliable, but they were not developed at the study time.
In conclusion, depression and anxiety were common in clinically stable older patients with psychiatric disorders. Considering the negative outcomes caused by depression and anxiety, regular screening, and effective treatment, such as appropriate pharmacotherapy and psychotherapy (e.g., cognitive behavior therapy)75,76, should be recommended for this population.
References
World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard https://covid19.who.int/ (2020).
Yang, Y. et al. Mental health services for older adults in China during the COVID-19 outbreak. Lancet Psychiatry 7, e19 (2020).
Pormohammad, A. et al. Clinical characteristics, laboratory findings, radiographic signs and outcomes of 61,742 patients with confirmed COVID-19 infection: a systematic review and meta-analysis. Micro. Pathog. 147, 104390 (2020).
Shahid, Z. et al. COVID-19 and older adults: what we know. J. Am. Geriatr. Soc. 68, 926–929 (2020).
Du, R.-H. et al. Predictors of mortality for patients with COVID-19 pneumonia caused by SARS-CoV-2: a prospective cohort study. Eur. Respir. J. 55, 2000524 (2020).
Hao, F. et al. Do psychiatric patients experience more psychiatric symptoms during COVID-19 pandemic and lockdown? A case-control study with service and research implications for immunopsychiatry. Brain Behav. Immun. 87, 100–106 (2020).
González-Blanco, L. et al. COVID-19 lockdown in people with severe mental disorders in Spain: do they have a specific psychological reaction compared with other mental disorders and healthy controls? Schizophr. Res. 223, 192–198 (2020).
Xiang, Y. T., Ng, C. H., Yu, X. & Wang, G. Rethinking progress and challenges of mental health care in China. World Psychiatry 17, 231 (2018).
Xiang, Y.-T., Yu, X., Sartorius, N., Ungvari, G. S. & Chiu, H. F. Mental health in China: challenges and progress. Lancet 380, 1715–1716 (2012).
Bendixen, A. B. & Engedal, K. Anxiety among older psychiatric patients: a hidden comorbidity? Aging Ment. Health 20, 1131–1138 (2016).
Beekman, A. T. et al. Anxiety and depression in later life: co-occurrence and communality of risk factors. Am. J. Psychiatry 157, 89–95 (2000).
Prina, A., Ferri, C., Guerra, M., Brayne, C. & Prince, M. Co-occurrence of anxiety and depression amongst older adults in low-and middle-income countries: findings from the 10/66 study. Psychol. Med 41, 2047 (2011).
Schoevers, R. A., Deeg, D. J. H., van Tilburg, W. & Beekman, A. T. F. Depression and generalized anxiety disorder: co-occurrence and longitudinal patterns in elderly patients. Am. J. Geriatr. Psychiatry 13, 31–39 (2005).
Gulpers, B. et al. Anxiety as a predictor for cognitive decline and dementia: a systematic review and meta-analysis. Am. J. Geriatr. Psychiatry 24, 823–842 (2016).
Wei, J. et al. Late-life depression and cognitive function among older adults in the U.S.: The National Health and Nutrition Examination Survey, 2011–2014. J. Psychiatr. Res. 111, 30–35 (2019).
Roy-Byrne, P. P. et al. Anxiety disorders and comorbid medical illness. Gen. Hosp. Psychiatry 30, 208–225 (2008).
Holvast, F. et al. Late-life depression and the association with multimorbidity and polypharmacy: a cross-sectional study. Fam. Pract. 34, 539–545 (2017).
World Health Organization. The ICD-10 Classification of Mental and Behavioural Disorders: Clinical Descriptions and Diagnostic Guidelines (World Health Organization, Geneva, 1992).
Avendano, M., Glymour, M., Banks, J. & Mackenbach, J. Health disadvantage in US adults aged 50 to 74 years: a comparison of the health of rich and poor Americans with that of Europeans. Am. J. Public Health 99, 540–548 (2009).
Dong, M. et al. Antipsychotic polypharmacy in older adult asian patients with schizophrenia: research on Asian psychotropic prescription pattern. J. Geriatr. Psychiatry Neurol. 32, 304–311 (2019).
Xiang, Y.-T. et al. Clinical and social determinants of psychotropic drug prescription for schizophrenia outpatients in China. Prog. Neuropsychopharmacol. Biol. Psychiatry 31, 756–760 (2007).
Lobana, A., Mattoo, S. K., Basu, D. & Gupta, N. Quality of life in schizophrenia in India: comparison of three approaches. Acta Psychiatr. Scandinavica 104, 51–55 (2001).
Hajian-Tilaki, K. Sample size estimation in epidemiologic studies. Casp. J. Intern. Med. 2, 289 (2011).
Shi, L. et al. Prevalence of and risk factors associated with mental health symptoms among the general population in China during the Coronavirus Disease 2019 Pandemic. JAMA Netw. Open 3, e2014053–e2014053 (2020).
Bo, H. X. et al. Posttraumatic stress symptoms and attitude toward crisis mental health services among clinically stable patients with COVID-19 in China. Psychol. Med. 27, 1–2 (2020).
Luo, H., Lie, Y. & Prinzen, F. W. Surveillance of COVID-19 in the general population using an online questionnaire: report from 18,161 respondents in China. JMIR Public Health Surveill. 6, e18576 (2020).
Zhou, J., Liu, L., Xue, P., Yang, X. & Tang, X. Mental health response to the COVID-19 outbreak in China. Am. J. Psychiatry 177, 574–575 (2020).
Kroenke, K., Spitzer, R. L. & Williams, J. B. The PHQ‐9: validity of a brief depression severity measure. J. Gen. Intern. Med. 16, 606–613 (2001).
Chen, M., Sheng, L. & Qu, S. Diagnostic test of screening depressive disorder in general hospital with the Patient Health Questionnaire (in Chinese). Chin. Ment. Health 29, 241–245 (2015).
Wang, W. et al. Reliability and validity of the Chinese version of the Patient Health Questionnaire (PHQ-9) in the general population. Gen. Hosp. Psychiatry 36, 539–544 (2014).
Kroenke, K., Spitzer, R. L., Williams, J. B. & Löwe, B. The patient health questionnaire somatic, anxiety, and depressive symptom scales: a systematic review. Gen. Hosp. Psychiatry 32, 345–359 (2010).
Spitzer, R. L., Kroenke, K., Williams, J. B. & Löwe, B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch. Intern. Med. 166, 1092–1097 (2006).
He, X.-Y., Li, C.-B., Qian, J., Cui, H.-S. & Wu, W.-Y. Study on the reliability and validity of Generalized Anxiety Scale in general hospitals (in Chinese). Shanghai Arch. Psychiatry 22, 200–203 (2010).
Morin, C. M. Insomnia: Psychological Assessment and Management (Guilford Press, 1993).
Bai, C., Daihong, J., Chen, L., Liang, L. & Wang, C. Reliability and validity of Insomnia Severity Index in clinical insomnia patients (in Chinese). Chin. J. Practical Nurs. 34, 2182–2186 (2018).
Smith, M. T. & Wegener, S. T. Measures of sleep: the Insomnia Severity Index, Medical Outcomes Study (MOS) Sleep Scale, Pittsburgh Sleep Diary (PSD), and Pittsburgh Sleep Quality Index (PSQI). Arthritis Care Res. 49, S184–S196 (2003).
Wong, D. L. & Baker, C. M. Pain in children: comparison of assessment scales. Pediatr. Nurs. 14, 9–17 (1988).
Haefeli, M. & Elfering, A. Pain assessment. Eur. Spine J. 15, S17–S24 (2006).
Boonstra, A. M. et al. Cut-off points for mild, moderate, and severe pain on the numeric rating scale for pain in patients with chronic musculoskeletal pain: variability and influence of sex and catastrophizing. Front Psychol. 7, 1466–1466 (2016).
Harper, A., Power, M. & Grp, W. Development of the World Health Organization WHOQOL-BREF quality of life assessment. Psychol. Med. 28, 551–558 (1998).
Fang, J. Q. & Hao, Y. A. Reliability and validity for Chinese Version of WHO Quality of Life Scale (in Chinese). Chin. Ment. Health J. 13, 203–209 (1999).
Xia, P., Li, N., Hau, K.-T., Liu, C. & Lu, Y. Quality of life of Chinese urban community residents: a psychometric study of the mainland Chinese version of the WHOQOL-BREF. BMC Med. Res. Methodol. 12, 37 (2012).
Zhou, S.-J. et al. Prevalence and socio-demographic correlates of psychological health problems in Chinese adolescents during the outbreak of COVID-19. Eur. Child Adolesc. Psychiatry 29, 749–758 (2020).
Orhan, M. et al. The relationship between cognitive and social functioning in older patients with bipolar disorder. J. Affect Disord. 240, 177–182 (2018).
Shimada, H. et al. Depressive symptoms and cognitive performance in older adults. J. Psychiatr. Res 57, 149–156 (2014).
Murante, T. & Cohen, C. I. Cognitive functioning in older adults with schizophrenia. Focus (Am. Psychiatr. Publ.) 15, 26–34 (2017).
Zainal, N. Z., Kalita, P. & Herr, K. J. Cognitive dysfunction in Malaysian patients with major depressive disorder: a subgroup analysis of a multicountry, cross-sectional study. Asia Pac. Psychiatry 11, e12346 (2019).
Wang, H., Yu, E. & Tang, Y. Psychological Support and Counselling for Older Adults During the Outbreak of COVID-19[M] (Chinese Medical Multimedia Press, Beijing, 2020).
Chinese Society of Geriatric Psychiatry, Alzheimer’s Disease Chinese of Chinese Aging Well Association (CAWA/ADC), Psychogeriatric Interest Group of Chinese Society of Psychiatry, Geriatric Psychiatry Working Group of Chinese Psychiatrists Association & Aging Mental Health Committee of Chinese Association for Mental Health. Expert recommendations on mental health and psychosocial support for persons with cognitive disorders and their caregivers during the COVID-19 outbreak (in Chinese). Chin. J. Psychiatry 53, 89–94 (2020).
Kessler, R. C., Chiu, W. T., Demler, O. & Walters, E. E. Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication. Arch. Gen. Psychiatry 62, 617–627 (2005).
Hettema, J. M., Kuhn, J. W., Prescott, C. A. & Kendler, K. S. The impact of generalized anxiety disorder and stressful life events on risk for major depressive episodes. Psychol. Med. 36, 789–795 (2006).
Wetherell, J. L., Gatz, M. & Pedersen, N. L. A longitudinal analysis of anxiety and depressive symptoms. Psychol. Aging 16, 187 (2001).
Molina, E. et al. Polymorphic variation at the serotonin 1-A receptor gene is associated with comorbid depression and generalized anxiety. Psychiatr. Genet. 21, 195–201 (2011).
Etkin, A. & Schatzberg, A. F. Common abnormalities and disorder-specific compensation during implicit regulation of emotional processing in generalized anxiety and major depressive disorders. Am. J. Psychiatry 168, 968–978 (2011).
Jaussent, I. et al. Insomnia and daytime sleepiness are risk factors for depressive symptoms in the elderly. Sleep 34, 1103–1110 (2011).
Hertenstein, E. et al. Insomnia as a predictor of mental disorders: a systematic review and meta-analysis. Sleep. Med. Rev. 43, 96–105 (2019).
Sunderajan, P. et al. Insomnia in patients with depression: a STAR*D report. CNS Spectr. 15, 394–404 (2010).
Khan, I. W., Juyal, R., Shikha, D. & Gupta, R. Generalized anxiety disorder but not depression is associated with insomnia: a population based study. Sleep. Sci. 11, 166–173 (2018).
de Lecea, L., Carter, M. E. & Adamantidis, A. Shining light on wakefulness and arousal. Biol. Psychiatry 71, 1046–1052 (2012).
Krysta, K., Krzystanek, M., Bratek, A. & Krupka-Matuszczyk, I. Sleep and inflammatory markers in different psychiatric disorders. J. Neural Transm. 124, 179–186 (2017).
Fayaz, A., Croft, P., Langford, R., Donaldson, L. & Jones, G. Prevalence of chronic pain in the UK: a systematic review and meta-analysis of population studies. BMJ Open 6, e010364 (2016).
Henschke, N., Kamper, S. J. & Maher, C. G. The epidemiology and economic consequences of pain. Mayo Clin. Proc. 90, 139–147 (2015).
Velly, A. M. & Mohit, S. Epidemiology of pain and relation to psychiatric disorders. Prog. Neuropsychopharmacol. Biol. Psychiatry 87, 159–167 (2018).
Gerrits, M. M. J. G. et al. Impact of pain on the course of depressive and anxiety disorders. Pain 153, 429–436 (2012).
Gureje, O., Von Korff, M., Simon, G. E. & Gater, R. Persistent pain and well-being: a World Health Organization study in primary care. JAMA 280, 147–151 (1998).
Fillingim, R. B. et al. Psychological factors associated with development of TMD: the OPPERA prospective cohort study. J. Pain. 14, T75–T90 (2013).
Aggarwal, V. R., Macfarlane, G. J., Farragher, T. M. & McBeth, J. Risk factors for onset of chronic oro-facial pain–results of the North Cheshire oro-facial pain prospective population study. Pain 149, 354–359 (2010).
Lurie, I. & Levine, S. Z. Meta-analysis of dropout rates in SSRIs versus placebo in randomized clinical trials of PTSD. J. Nerv. Ment. Dis. 198, 116–124 (2010).
Taylor, S., Abramowitz, J. S. & McKay, D. Non-adherence and non-response in the treatment of anxiety disorders. J. Anxiety Disord. 26, 583–589 (2012).
Katon, W., Lin, E. H. & Kroenke, K. The association of depression and anxiety with medical symptom burden in patients with chronic medical illness. Gen. Hosp. Psychiatry 29, 147–155 (2007).
Härter, M. C., Conway, K. P. & Merikangas, K. R. Associations between anxiety disorders and physical illness. Eur. Arch. Psychiatry Clin. Neurosci. 253, 313–320 (2003).
Villarreal-Zegarra, D. & Bernabe-Ortiz, A. Association between arterial hypertension and depressive symptoms: results from population-based surveys in Peru. Asia Pac. Psychiatry 12, e12385 (2020).
Hatoum, H. T., Kong, S. X., Kania, C. M., Wong, J. M. & Mendelson, W. B. Insomnia, health-related quality of life and healthcare resource consumption. Pharmacoeconomics 14, 629–637 (1998).
Zainal, N. H. & Newman, M. G. Executive function and other cognitive deficits are distal risk factors of generalized anxiety disorder 9 years later. Psychol. Med. 48, 2045 (2018).
Ng, P., Tsun, A., Su, S. & Young, D. Cognitive behavioral intervention in the Chinese cultural context: a case report. Asia Pac. Psychiatry 5, 205–211 (2013).
Zhao, X. R. et al. Mindfulness-based cognitive therapy is associated with distinct resting-state neural patterns in patients with generalized anxiety disorder. Asia Pac. Psychiatry 11, e12368 (2019).
Acknowledgements
The study was supported by the National Science and Technology Major Project for investigational new drug (2018ZX09201-014), the Beijing Municipal Science and Technology Commission (No. Z181100001518005), the University of Macau (MYRG2019-00066-FHS), and the Suzhou Key Medical Center for Psychiatric Diseases (Szzx201509).
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Li, W., Zhao, N., Yan, X. et al. The prevalence of depressive and anxiety symptoms and their associations with quality of life among clinically stable older patients with psychiatric disorders during the COVID-19 pandemic. Transl Psychiatry 11, 75 (2021). https://doi.org/10.1038/s41398-021-01196-y
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41398-021-01196-y
This article is cited by
-
Lifestyles and Quality of Life of People with Mental Illness During the COVID-19 Pandemic
Community Mental Health Journal (2024)
-
Depression severity mediates stigma and quality of life in clinically stable people with schizophrenia in rural China
BMC Psychiatry (2023)
-
The mediating role of individual-level social capital among worries, mental health and subjective well-being among adults in Hong Kong during the COVID-19 pandemic
Current Psychology (2023)
-
The impact of COVID-19-related distress on levels of depression, anxiety and quality of life in psychogeriatric patients
European Archives of Psychiatry and Clinical Neuroscience (2022)
-
Mental health of older people in social isolation: the role of physical activity at home during the COVID-19 pandemic
Sport Sciences for Health (2022)
