
Abstract
Epidemiologic surveillance has revealed decoupling of Coronavirus Disease 2019 (COVID-19) hospitalizations and deaths from case counts after emergence of the Omicron (B.1.1.529) severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) variant globally. However, assessment of the relative severity of Omicron variant infections presents challenges because of differential acquired immune protection against Omicron and prior variants and because longer-term changes have occurred in testing and healthcare practices. Here we show that Omicron variant infections were associated with substantially reduced risk of progression to severe clinical outcomes relative to time-matched Delta (B.1.617.2) variant infections within a large, integrated healthcare system in Southern California. Adjusted hazard ratios (aHRs) for any hospital admission, symptomatic hospital admission, intensive care unit admission, mechanical ventilation and death comparing individuals with Omicron versus Delta variant infection were 0.59 (95% confidence interval: 0.51–0.69), 0.59 (0.51–0.68), 0.50 (0.29–0.87), 0.36 (0.18–0.72) and 0.21 (0.10–0.44), respectively. This reduced severity could not be explained by differential history of prior infection among individuals with Omicron or Delta variant infection and was starkest among individuals not previously vaccinated against COVID-19 (aHR = 0.40 (0.33–0.49) for any hospital admission and 0.14 (0.07–0.28) for death). Infections with the Omicron BA.2 subvariant were not associated with differential risk of severe outcomes in comparison to BA.1/BA.1.1 subvariant infections. Lower risk of severe clinical outcomes among individuals with Omicron variant infection should inform public health response amid establishment of the Omicron variant as the dominant SARS-CoV-2 lineage globally.
Similar content being viewed by others
Main
After its first detection in Southern Africa, the Omicron (B.1.1.529) variant of SARS-CoV-2 was declared by the World Health Organization to be a variant of concern on 25 November 2021 (ref. 1). Rapid transmission of the Omicron variant fueled a fourth wave of SARS-CoV-2 infections in South Africa, during which daily diagnosed infections soon exceeded totals recorded during all previous periods in the country. After its initial detection in the United States on 1 December 2021 (ref. 2), the Omicron variant rapidly became the dominant circulating lineage, accounting for 95% of all SARS-CoV-2 infections diagnosed nationwide by the week ending 8 January 2022 (ref. 3). Similar patterns have unfolded globally, with the Omicron variant fueling a surge in newly diagnosed cases worldwide4. Across the United States, the estimated prevalence of infection-derived antibodies increased from 34% to 58% during the Omicron wave between December 2021 and February 2022 and from 44% to 75% among children aged 0–11 years5. Although BA.2-lineage Omicron infections have subsequently accounted for increased transmission in March and April 2022, increases in hospital admissions and deaths have not been commensurate with previous surges6.
Understanding the clinical spectrum of infections associated with novel SARS-CoV-2 variants is crucial to informing public health responses. Questions about the severity of Omicron variant infections arose soon after its emergence, as the Omicron genome harbored a constellation of mutations in the SARS-CoV-2 spike protein associated with altered cell entry as well as immune evasion7. Reduced neutralization of the Omicron variant has been reported in studies using plasma specimens from individuals with complete (two-dose or three-dose) mRNA vaccine series8 and from patients with prior SARS-CoV-2 infection9,10. Epidemiologic data from South Africa have suggested higher rates of Omicron variant infections among individuals with prior SARS-CoV-2 infection, as compared to observations with previous variants11, and early observational studies in multiple settings have suggested reduced effectiveness of COVID-19 vaccines against Omicron variant infection12,13,14. Notwithstanding these signs of reduced immune protection against the Omicron variant associated with prior natural infection or vaccination, increases in SARS-CoV-2 infections after emergence of the Omicron variant were not associated with increases in hospitalizations and deaths to the extent observed during previous waves15,16,17,18. Although reduced risk of hospitalization, intensive care unit (ICU) admission and death has been reported among individuals with Omicron variant infection in several large-scale studies linking case data across various nationwide surveillance platforms14,19,20, these studies have lacked detailed information about individual-level factors that may confound the relationship between infecting variant and risk of severe clinical outcomes. Understanding of the relative severity of disease associated with the BA.2 Omicron subvariant, which has become established in transmission despite widespread immunity from the initial Omicron wave, remains limited as well21,22.
Results
Study setting and variant dynamics
We sought to compare clinical outcomes among individuals with Omicron and Delta variant SARS-CoV-2 infections within the Kaiser Permanente of Southern California (KPSC) healthcare system. As an integrated healthcare organization serving 4.7 million individuals (~19% of the population of Southern California), KPSC provides comprehensive care to its members across virtual, outpatient, emergency department and inpatient settings. Healthcare delivery, including diagnoses, laboratory tests and results and prescriptions, are recorded in near real time via patient electronic health records (EHRs), and out-of-network care is captured through insurance claim reimbursements, enabling near-complete ascertainment of healthcare interactions for KPSC members.
Our primary analyses included all individuals first ascertained via outpatient SARS-CoV-2 reverse transcription polymerase chain reaction (RT–PCR) testing between 15 December 2021 and 17 January 2022, whose tests were processed using the TaqPath COVID-19 Combo Kit (Thermo Fisher Scientific) (Fig. 1; details on testing procedures are provided in the Methods). We selected these dates to define an analysis period with mixed circulation of the two variants; Omicron accounted for 99% of daily incident cases in the state of California by 17 January 2022. Previous evidence has indicated that the Δ69–70 amino acid deletion in the spike protein of Omicron variant specimens causes a failure in PCR probes targeting the S gene, whereas the Orf1ab and nucleocapsid (N) probes retain sensitivity; in contrast, S gene target failure (SGTF) is rare in Delta variant SARS-CoV-2 infections (Supplementary Table 1)20,23,24. Thus, we used SGTF as a proxy for Omicron versus Delta variant identification. Delta variant detections receded in late January as BA.2 Omicron subvariant infections began to account for an increasing proportion of all cases detected through February and March. We, therefore, also sought to investigate differences in risk of severe clinical outcomes among outpatient-detected individuals of BA.2 versus BA.1/BA.1.1 (BA.1*) Omicron subvariant infections over the period of 3 February to 17 March 2022, when reductions in Delta variant detection to <0.1% of incident cases made S gene detection a reliable proxy for BA.2 subvariant determination, consistent with observations in other settings21,22.

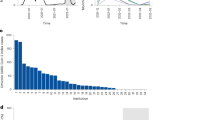
Plots illustrate total SARS-CoV-2 testing undertaken within the KPSC healthcare system across all clinical settings (a, along with the proportion of tests with positive results (inset)); total outpatient SARS-CoV-2 testing implemented using the ThermoFisher TaqPath COVID-19 Combo Kit assay along with the proportion of tests with SGTF identified (b; blue for SGTF detections and red for non-SGTF detections, with cases from 17 February to 17 March presented on an expanded scale for clarity (inset)); and new inpatient admissions of individuals with SARS-CoV-2 infection (c; pink for new detections on or after the admission date and green for individuals first ascertained by outpatient testing). Plotted data include 382,971 individuals diagnosed over the study period; of these, 375,642 were tested in outpatient settings, and 316,785 had samples processed using the TaqPath COVID-19 Combo Kit assay.
Characteristics of cases, by infecting variant
From 15 December 2021 to 17 January 2022, outpatient-diagnosed cases with Omicron variant infection (n = 222,688) were concentrated among adults aged 20–39 years and had lower odds of being either very young or very old in comparison to contemporaneously identified individuals with Delta variant infection (n = 23,305) (Table 1 and Supplementary Tables 2 and 3). Individuals with Omicron variant infection were also more often White and of non-Hispanic ethnicity; they lived in higher-income communities and tended to have lower prior-year rates of healthcare use across outpatient, emergency department and inpatient settings; and they had lower burden of chronic comorbid conditions, in comparison to individuals with Delta variant infection (Table 1 and Supplementary Table 2). These associations held in analyses adjusting for all measured demographic and clinical attributes of cases, which further included sex, current/former cigarette smoking, body mass index and documented prior SARS-CoV-2 infection and COVID-19 vaccination. Adjusted odds of a prior documented SARS-CoV-2 infection ≥90 days before individuals first tested positive during the study period were 1.75 (1.39–2.19)-fold higher among individuals with Omicron variant infection than among individuals with Delta variant infection. Additionally, individuals with Omicron variant infection tended to have received vaccine series associated with greater degrees of immune protection. For instance, adjusted odds of receipt of three or more mRNA vaccine doses were 2.60 (2.47–2.75)-fold higher among individuals with Omicron variant infection as compared to individuals with Delta variant infection, whereas adjusted odds of prior receipt of a single mRNA vaccine dose and a single Ad.26.COV2.S dose were only 1.38 (1.27–1.51)-fold and 1.56 (1.44–1.70)-fold higher among individuals with Omicron variant infection as compared to Delta variant infection, respectively (Supplementary Tables 2 and 4).
From 3 February to 17 March 2022, among individuals tested as outpatients, BA.2 Omicron subvariant cases (n = 1,905) did not differ from BA.1* subvariant cases (n = 12,756) in demographic or clinical attributes, with the exception that BA.1* detection was more concentrated among individuals aged 20–49 years than BA.2, which was comparatively more common among both children and older adults; additionally, individuals with BA.2 subvariant infection had higher rates of prior-year emergency department use than individuals infected with BA.1* lineages (Table 1 and Supplementary Table 5). Consistent differences in anti-SARS-CoV-2 immunity among individuals with BA.2 or BA.1* infection—based on number or timing of vaccine doses received or documented history of infection—were not apparent (Supplementary Table 6).
Risk of severe outcomes associated with infecting variant
After an outpatient diagnosis, cumulative 30-day risks of hospital admission, symptomatic hospital admission (defined as new inpatient admission ≤14 days after new-onset acute respiratory symptoms), ICU admission, onset of mechanical ventilation and death among individuals with Delta variant infection were 10.3, 9.7, 1.1, 0.7 and 0.7 per 1,000 individuals, respectively, for individuals testing positive between 15 December 2021 and 17 January 2022 (Fig. 2a–e). For individuals with Omicron variant infection over the same period of time, 30-day risks for the same outcomes were 4.5, 3.9, 0.2, 0.1 and 0.1 per 1,000 individuals. To understand whether these differences in risk could be explained by observed demographic, clinical and immunological characteristics of individuals with Delta and Omicron variant infection, we estimated adjusted hazards ratios (aHRs) for progression to each of these endpoints using Cox proportional hazards models, stratified on individuals’ testing dates to further account for potential changes in clinical or testing practices over time (Methods). Over the 30 days after an outpatient diagnosis, aHRs comparing progression to any hospital admission and symptomatic hospital admission among individuals with Omicron versus Delta variant infection were 0.59 (0.51–0.69) and 0.59 (0.51–0.68), respectively (Supplementary Table 7). These estimates should be interpreted as a weighted average of instantaneous aHRs comparing individuals testing positive for Omicron and Delta variant infections on the same date, over their full follow-up period25. For higher-acuity endpoints of ICU admission, mechanical ventilation and mortality, aHR estimates comparing Omicron to Delta variant cases over the 60 days after outpatient detection were 0.50 (0.29–0.87), 0.36 (0.18–0.72) and 0.21 (0.10–0.44), respectively.

Plots illustrate cumulative 30-day risk of severe clinical outcomes among individuals first ascertained in outpatient settings, stratified by SGTF status for infecting variant or subvariant. Panels in the top row compare individuals with Delta (non-SGTF; red) or Omicron (SGTF; blue) variant infections testing positive in an outpatient setting between 15 December 2021 and 17 January 2022, for endpoints of any hospital admission (a); symptomatic hospital admission (b); ICU admission (c); mechanical ventilation (d); and death (e). Panels in the bottom row compare individuals with BA.2 (non-SGTF; yellow) and BA.1* (SGTF; blue, comprising BA.1/BA.1.1/BA.1.1.529 lineages) subvariant Omicron infections diagnosed in an outpatient setting between 3 February and 17 March 2022, for endpoints of any hospital admission (f); symptomatic hospital admission (g); ICU admission (h); and death (i). Mechanical ventilation among BA.2 and BA.1* Omicron subvariant individuals is not included due to sparse observations. Shaded areas denote 95% confidence intervals around median estimates (center lines). Analyses include 23,305 individuals with Delta variant infection and 222,688 individuals with Omicron variant infection over the period of 15 December 2021 to 17 January 2022 and 1,905 individuals with BA.2 Omicron subvariant infection and 12,756 individuals with BA.1* Omicron subvariant infection over the period of 3 February to 17 March 2022. Confidence intervals were obtained via bootstrap resampling.
Similar estimates held in analyses that included individuals diagnosed on or after their hospital admission date (Supplementary Table 7) and in analyses restricted to individuals who were asymptomatic at the point of testing (Supplementary Table 8), among whom Omicron variant infection was also associated with modestly lower risk of subsequently reported symptoms onset (aHR = 0.88 (0.81–0.96) for individuals with Omicron versus Delta variant infection tested in outpatient settings, without symptoms at the point of testing). Estimates of the aHR were also consistent in analyses restricted to individuals with either complete data on measured covariates or those enrolled in KPSC health plans ≥1 year before their positive test date (Supplementary Table 9); moreover, our findings held within subgroups defined on the basis of individuals’ age, sex, presence of comorbidities and history of documented SARS-CoV-2 infection (Supplementary Table 10). Estimates of the adjusted relative risk (aRR) of hospital admission and symptomatic hospital admission (30-day) as well as ICU admission, mechanical ventilation and mortality (60-day) based on log-binomial regression closely resembled aHR estimates from Cox proportional hazards models in the primary analysis (aRR = 0.63 (0.55–0.72), 0.63 (0.55–0.72), 0.54 (0.31–0.94), 0.35 (0.17–0.71) and 0.20 (0.10–0.43) for the five endpoints, respectively; Supplementary Table 11). Findings of reduced risk of progression to hospital admission and symptomatic hospital admission further held within sensitivity analyses that additionally accounted for the possibility of differential prevalence of undiagnosed prior SARS-CoV-2 infection among individuals with Omicron or Delta variant infection who were or were not hospitalized and who were or were not vaccinated (Supplementary Figs. 1 and 2).
We did not identify evidence of differences in risk of severe outcomes associated with BA.2 or BA.1* Omicron subvariant infection among individuals diagnosed in outpatient settings over the period of 3 February to 17 March 2022 (Supplementary Table 12). Among individuals with BA.1* Omicron subvariant infection diagnosed over this period, 30-day risks of hospital admission, symptomatic hospital admission, ICU admission, mechanical ventilation and mortality were 13.3, 11.5, 0.4, 0.0 and 1.0 per 1,000 individuals, respectively (Fig. 2f–j). Among individuals with BA.2 infection, 30-day risks of the same outcomes were 14.7, 12.6, 0.5, 0.5 and 0.5, respectively, per 1,000 individuals.
Omicron and Delta variant severity by vaccination status
Coefficient estimates from Cox proportional hazards models suggested that equivalent numbers of vaccine doses were associated with greater reductions in risk of severe outcomes among individuals with Delta variant infection as compared to Omicron variant infection (for two mRNA doses ≤90 days before testing versus zero doses, aHR = 0.17 (0.12–0.24) among Delta variant cases and aHR = 0.51 (0.34–0.76) among Omicron variant cases; for three mRNA doses versus zero doses, aHR = 0.14 (0.08–0.24) among Delta variant cases and aHR = 0.43 (0.35–0.52) among Omicron variant cases; Supplementary Table 13), consistent with superior vaccine protection against disease progression involving the Delta variant. Because variant-specific differences in vaccine protection could, thus, confound the relationship between infecting variant and risk of severe clinical outcomes, we further undertook analyses of individuals with Delta and Omicron variant infection stratifying by prior vaccine exposure. For endpoints of hospital admission, symptomatic hospital admission, ICU admission, mechanical ventilation and mortality, aHR estimates were 0.40 (0.33–0.49), 0.40 (0.33–0.49), 0.34 (0.17–0.66), 0.24 (0.12–0.48) and 0.14 (0.07–0.28), respectively, among unvaccinated individuals with Omicron versus Delta variant infection (Fig. 3 and Supplementary Table 14). In contrast, variant-specific differences in risk of hospital admission or symptomatic hospital admission were not apparent among individuals who received three or more mRNA vaccine doses. Among individuals who had received two mRNA vaccine doses, variant-specific differences in risk of hospital admission or symptomatic hospital admission were likewise attenuated, with the smallest difference among individuals most recently vaccinated. We did not identify differences in risk of ICU admission and mechanical ventilation among vaccinated individuals with Omicron or Delta variant infection. However, among vaccinated individuals, Omicron infection remained associated with a lower risk of mortality than Delta infection (aHR = 0.25 (0.09–0.70)). Similar findings held in analyses that included individuals testing positive on the day of hospital admission (Supplementary Fig. 3).

Points and lines denote median estimates and accompanying 95% confidence intervals for the aHR of each endpoint, comparing individuals with Omicron versus Delta variant infection, in case strata defined by history of COVID-19 vaccination. Analyses are restricted to individuals diagnosed in outpatient settings by RT–PCR testing using the TaqPath COVID-19 Combo Kit; aHRs were estimated using Cox proportional hazards regression models, controlling for covariates listed in Supplementary Table 2 and stratifying on positive test date. Analyses include 23,305 individuals with Delta variant infection and 222,688 individuals with Omicron variant infection. Confidence intervals were obtained using Cox proportional hazards regression models. CI, confidence interval.
Changes over time among all cases
Because excluding individuals whose tests were not processed using the TaqPath COVID-19 Combo Kit could limit the generalizability of our primary analyses, we also assessed changes over the period of 1 November 2021 (before detection of the Omicron variant in the state of California) to 17 January 2022 in the risk for all individuals diagnosed in outpatient settings to progress to severe clinical outcomes. In analyses using Cox proportional hazards models, which allowed for zero, one or two changepoints in the relationship between testing date and risk of severe clinical outcomes26, we identified evidence for a reduction beginning 8–23 December 2021 in individuals’ risk of any hospital admission, symptomatic hospital admission, ICU admission and mortality among newly diagnosed individuals (Fig. 4a–e and Supplementary Table 15; changepoint models were not fitted to the mechanical ventilation endpoint due to sparse observations during the Delta-variant-dominated period). This timing encompasses the period of Omicron’s expansion in the study population, with 5% and 50% of individuals tested on TaqPath COVID-19 Combo Kit assays showing SGTF as of 10 and 17 December 2021, respectively.

Panels illustrate proportions of individuals experiencing each clinical outcome over the course of follow-up (30 days for endpoints of hospital admission (a) or symptomatic hospital admission (b); and 60 days for ICU admission (c), mechanical ventilation (d) and mortality (e)). Gray vertical lines in a–e denote 95% confidence intervals around proportions for each day based on bootstrap resampling; 7-day moving averages are plotted by red lines. Polygons at the bottom of a–e illustrate probability densities of changepoint timings (blue), whereas inset panels illustrate fitted slopes for aHR estimates for each endpoint as a function of testing date (red lines indicating median estimates, with pink shaded polygons delineating 95% confidence intervals, as generated by Cox proportional hazards models). Bottom panels illustrate the proportion of individuals tested in outpatient settings indicating symptoms onset on or before their testing date (f); mean time from symptoms onset to outpatient testing, among symptomatic individuals (g); and mean time from the testing date to hospital admission, among admitted individuals (h). Gray vertical lines in f–h denote 95% confidence intervals around proportions for each day based on bootstrap resampling; 7-day moving averages are plotted by red lines. Changes in the proportion of individuals ascertained in inpatient settings are plotted separately in Supplementary Fig. 4. Analyses include 316,038 outpatient-diagnosed individuals. CI, confidence interval.
Reductions in individuals’ risk of severe outcomes did not directly align with changes in clinical attributes of individuals testing positive in outpatient settings over this period, suggesting that shifting patterns of healthcare use and clinical practice could not fully account for the observed changes. The proportion of individuals reporting symptoms on or before their testing date held steadily in the range of 72.2–84.3% from 1 November 2021 to 17 January 2022 (Fig. 4f). Although the mean time from symptoms onset to testing (among symptomatic individuals) dipped transiently to 3.2 days between 19 and 22 December (as compared to 4.2 days in November and mid-January; Fig. 4g), time from testing to inpatient admission (among individuals ultimately requiring hospitalization) declined through the month of January, consistent with individuals seeking outpatient testing at a more advanced stage of their illness (Fig. 4h). Concurrently, the proportion of all SARS-CoV-2 infections detected in inpatient settings declined from 2.4% to 0.7% between 1 and 31 December 2021, although this proportion increased roughly ten-fold to 7.8% as of 7 March 2022 amid reductions in outpatient testing volume during 2022 (Supplementary Fig. 4).
Lengths of hospital stay
Duration of hospital stay among individuals whose illness met the severity threshold for hospital admission provides additional insight into differences in the clinical course of SARS-CoV-2 variants27,28. Among 208 individuals testing positive for Delta variant infection in outpatient settings and admitted to hospital over the period of 15 December 2021 to 17 January 2022, the proportions with hospital stays lasting ≤5 days, ≤10 days and ≤15 days were 66.2%, 84.5% and 89.4%, respectively, in comparison to 84.8%, 91.0% and 92.2% among 703 individuals with Omicron variant infection who were tested and admitted over the same period (Fig. 5a–f and Supplementary Table 16). Within this sample, 73.8% and 85.6% of admitted individuals with Delta and Omicron variant infections, respectively, were discharged home within ≤30 days, whereas 15.5% and 6.0% of admitted individuals with Delta and Omicron variant infections, respectively, were referred to other care settings or discharged against medical advice within the same timeframe. The 30-day probability of death or discharge to hospice after admission was 1.1% for individuals with Delta variant infection and 0.4% for individuals with Omicron variant infection. Using a Cox proportional hazards model stratified on individuals’ admission date and controlling for all observed demographic, clinical and immunological attributes of cases to compare time to completion of hospital stay (with any final disposition), the aHR comparing outpatient-diagnosed individuals with Omicron versus Delta variant infection was 1.24 (0.99–1.57; Supplementary Table 17). No differences in the duration of hospital stay or likelihoods of each discharge disposition were evident among outpatient-diagnosed individuals with BA.2 or BA.1* Omicron subvariant infection tested and admitted between 3 February and 17 March 2022 (Fig. 5g–k). The aHR for completion of hospital stay (with any final disposition) for outpatient-diagnosed individuals with BA.2 versus BA.1* Omicron subvariant infection was 0.95 (0.41–2.22; Supplementary Table 17).

Top panels illustrate times from hospital admission to discharge to home without skilled care (a), discharge to skilled care or against medical advice (b) and in-hospital death or discharge to hospice (c) among individuals testing positive in outpatient settings and subsequently admitted to hospital on or after the date of symptoms onset over the period from 15 December 2021 to 17 January 2022; lines and polygons indicate median estimates and 95% confidence intervals, respectively, based on bootstrap resampling for individuals with Delta (red) and Omicron (blue) variant infection. Below, panels illustrate histograms of the total length of stay for individuals with Delta variant infection (d) and Omicron variant infection (e) within this sample as well as distributions of the likelihood ratio for individuals with Delta versus Omicron infection to have hospital stays lasting >5 days, >10 days, >15 days and >20 days (f). The bottom set of panels illustrates times from admission to discharge to home (g) and discharge to skilled care or against medical advice (h), among individuals testing positive in outpatient settings and subsequently admitted to hospital on or after the date of symptoms onset over the period from 3 February to 17 March 2022; center lines and polygons indicate median estimates and 95% confidence intervals, respectively, based on bootstrap resampling for individuals with BA.2 (yellow) and BA.1* (blue) Omicron subvariant infection. Below, panels illustrate histograms of the total length of stay for individuals with BA.2 Omicron subvariant infection (i) and BA.1* Omicron subvariant infection (j) within this sample as well as distributions of the likelihood ratio for individuals with BA.2 versus. BA.1* Omicron subvariant infection to have hospital stays lasting >5 days, >10 days, >15 days and >20 days (k). Analyses include 208 individuals with Delta variant infection and 703 individuals with Omicron variant infection for the period of 15 December 2021 to 17 January 2022 and 23 individuals with BA.2 Omicron subvariant infection and 146 individuals with BA.1* Omicron subvariant infection for the period of 3 February to 17 March 2022. Confidence intervals were computed via bootstrap resampling.
Discussion
Among individuals followed from an outpatient SARS-CoV-2 diagnosis, infection with the Omicron variant was associated with substantially lower risk of progression to severe clinical outcomes, including hospital admission, symptomatic hospital admission, ICU admission, mechanical ventilation and mortality, in comparison to infection with the Delta variant. These differences in risk among individuals with Omicron versus Delta variant infection were consistent with reductions in the proportion of all SARS-CoV-2 cases that progressed to severe clinical outcomes during the period of Omicron variant emergence in the study population. Notably, differences in risk of severe outcomes associated with Omicron versus Delta variant infection were greatest among unvaccinated individuals. Whereas vaccination was associated with reductions in disease severity for individuals with both Omicron and Delta variant infections, the degree of vaccine-associated protection against progression to severe disease was greater among individuals with Delta variant infection. Owing to these combined effects of infecting variant and vaccination, risk of severe disease with either the Omicron or Delta variant was equivalent for individuals who had received three or more mRNA vaccine doses or who had recently received two mRNA vaccine doses. We also observed shorter durations of hospital stay after inpatient admission among individuals with Omicron as compared to Delta variant infection. Whereas admitted individuals with Omicron variant infection had higher likelihood than individuals with Delta variant infection of being discharged to home, those with Delta variant infection had higher probability of mortality and discharge to skilled care or against medical advice. We did not identify evidence of differences in severity for individuals with BA.2 and BA.1* Omicron subvariant infection, based on either their risk of severe clinical outcomes or their hospital length of stay and final disposition after inpatient admission, suggesting that the reduced severity of disease associated with the Omicron variant has persisted after emergence and establishment of the BA.2 subvariant.
Previous studies have estimated reductions in risk of hospital admission associated with Omicron variant infection across a range spanning 20–80%14,19,20,29,30,31,32. Variability in prior estimates from database linkage studies may owe, in part, to intra-study and inter-study differences in immunity, health status and healthcare-seeking behaviors among individuals across settings. As KPSC serves as a comprehensive healthcare provider to its members, and tracks out-of-network care provision for its members through insurance claim reimbursements, our study benefited from highly resolved EHRs as a basis for characterizing individuals’ clinical history. Similar detail may be lacking in other large-scale studies from throughout the pandemic, which have varyingly relied on administrative record linkage to identify comorbid conditions19, had access to such data only for admitted individuals based on in-hospital assessment or record linkage20,30,33 or have lacked data on individuals’ history of comorbidities and healthcare use entirely14,32,34,35. Despite these differences in specific design features and estimates across studies, consistency of the finding that Omicron variant infection is associated with reduced severity relative to Delta variant infection is noteworthy.
Several other aspects of our study helped to control for relevant potential differences in attributes of individuals with Delta and Omicron variant infection, which could otherwise confound comparisons of risk for severe clinical outcomes. Stratification of Cox proportional hazards models on individuals’ testing and admission dates, and inclusion of day-specific intercepts in logistic regression models, helped to correct for potential differences in attributes of individuals tested or admitted over time unrelated to the infecting variant. Restriction of primary analyses to individuals tested in outpatient settings enabled us to account for selection on healthcare-seeking behavior among individuals infected with either variant. This strategy further standardized the level of clinical severity associated with the hospital admission endpoint. After outpatient testing at KPSC throughout the study period, individuals considered to be at risk of severe illness, but not meeting admission criteria, were enrolled in a home-based monitoring program with daily clinical interaction and standardized criteria for emergency department referral and inpatient admission36. Thus, clinical severity at the point of admission among outpatient-diagnosed individuals may have been less variable than among individuals ascertained at the point of admission. Focusing primary analyses on outpatient-diagnosed individuals also helped to limit inclusion of hospitalizations attributable to causes other than COVID-19. As the incidence rate of all-cause hospital admissions is low, few hospitalizations attributable to factors other than COVID-19 would be expected to occur within the short period of time immediately after a positive outpatient test; in contrast, a substantial proportion of SARS-CoV-2 infections among hospitalized individuals may be detected simply due to entry screening at the point of admission for other causes37. Although it is a limitation that no routinely collected records provide a gold standard determination of whether SARS-CoV-2 infection was the cause of the decision to admit a patient to hospital, these factors (together with our consideration of one endpoint restricted to inpatient admissions occurring on or after the date of symptoms onset) limit the risk of misclassification of hospital admissions attributable to causes other than COVID-19 to a greater extent than has been possible in prior studies of Omicron as well as other SARS-CoV-2 variants11,14,16,19,20,30,31,35.
Unobserved prior infections are a potential source of bias when comparing risk of severe outcomes among individuals with Omicron or Delta variant infection38,39. Before the Omicron epidemic wave, roughly one in 2.5 infections in the state of California were estimated to have been caught by testing, indicating that individuals’ history of infection may be substantially underestimated in our study population40. Moreover, because convalescent sera from previously infected individuals has shown weaker neutralization activity against the Omicron variant as compared to Delta (and earlier) variants41,42, prevalence of unascertained prior infection among individuals with Omicron and Delta variant infections may be distinct. We nonetheless identified that findings of reduced severity of Omicron variant infections persisted within sensitivity analyses, allowing substantially greater-than-observed prevalence of prior infection among previously vaccinated individuals with Omicron variant infections who were not hospitalized—the stratum within which unobserved infections would contribute the greatest degree of bias for our primary estimates. In agreement with these findings, sensitivity analyses within prior studies using diverse statistical inference methods have suggested that differences in risk of severe clinical outcomes among individuals with Omicron and Delta variant infections cannot be explained by unobserved prior infections alone11,14. Furthermore, the unadjusted HR of hospital admission associated with Omicron variant detection among individuals in our study known to have experienced prior infection was 0.27 (0.03–2.44) after a positive outpatient test (Supplementary Table 10). Although analyses within this stratum are underpowered, the direction of association is telling as differential unobserved prior infection among individuals with Omicron and Delta variant infection could not account for risk of severe outcomes among these individuals.
There are several barriers to causal inference in this study. Because our analysis aims to compare disease severity among individuals after acquisition of Omicron or Delta variant infection, no real-world trial directly emulates the inferential design conditioning on acquisition of infection. Observed associations of infecting lineage with case attributes within our sample should not be considered to represent predictors of acquisition of a specific infecting SARS-CoV-2 lineage;43 risk factors for exposure to each variant and for infection, given exposure, are outside the scope of this study. Although statistical adjustment for differences in demographic, clinical and immunological aspects of cases supported efforts to define associations of each variant with risk of severe outcomes, given acquisition of infection, unobserved attributes of cases that predict both their infecting variant and risk of severe clinical outcomes remain of concern, as in all observational epidemiologic research44. Finally, although selecting individuals who sought outpatient tests ensures that our primary analysis encompasses individuals meeting a minimum threshold for healthcare-seeking behavior, further adjustment for this characteristic was limited to individuals’ prior-year frequency of healthcare use across outpatient, emergency department and inpatient settings. Notwithstanding these limitations, our findings of reduced severity in Omicron variant infections are consistent with numerous lines of experimental evidence not susceptible to similar sources of bias. Ex vivo studies demonstrate higher replication of the Omicron variant in explant cultures of human upper respiratory tract tissue as compared to cultures from the small airways of the lung45, whereas, in animal models, disease associated with the Omicron variant has been confined to the large airway46.
Although attenuation of disease severity in Omicron variant infections—which has held amid emergence of the BA.2 subvariant—is an encouraging finding, evidence of higher transmissibility of Omicron variant infections47 as well as immune evasion from prior infection and vaccination remain concerning. High rates of infection in the community have overwhelmed healthcare systems within the United States and other settings and have translated to high absolute numbers of hospitalizations and deaths even with lower severity of infections associated with the Omicron variant. Observations in settings with previously low prevalence of infection-derived immunity, such as Hong Kong48 and New Zealand49, underscore the risk for the Omicron variant to cause substantial burden of severe and fatal illness even if individuals tend to experience lower risk of severe clinical outcomes than with Delta variant infection. This observation is also consistent with the frequent occurrence of severe disease cases and deaths in clinically vulnerable populations, such as residents of long-term care facilities in the United States, United Kingdom and Italy, with ancestral (Wuhan) variant infections50. Our findings underscore the value of monitoring variant-specific infection severity alongside ongoing surveillance efforts aimed at tracking epidemiologic dynamics of novel variants to inform intervention deployment and healthcare capacity planning.
Methods
Ethics, setting and procedures
The study protocol was reviewed and approved by the KPSC Institutional Review Board for ethical compliance. A waiver of informed consent was obtained for this observational study as data were collected administratively in the course of routine clinical care delivery. A waiver for written Health Insurance Portability and Accountability Act authorization was obtained for research involving use of patient EHRs.
Care delivery and EHR data captured in the KPSC healthcare system have been described previously51. In brief, members of KPSC receive care through employer-provided, pre-paid or federally sponsored insurance plans and closely resemble the sociodemographic profile of the surrounding geographic area in terms of age, racial/ethnic composition and community characteristics52. Within-network care delivery encompassing diagnoses, laboratory tests and results and prescriptions is captured in real time through patient EHRs, whereas out-of-network care is captured through insurance reimbursements. COVID-19 vaccines were provided at no cost to KPSC members after emergency use authorization and were, therefore, captured in the EHR. Vaccinations administered outside KPSC were captured via the California Immunization Registry, to which providers are required to report all COVID-19 vaccine administrations within 24 hours.
PCR testing for SARS-CoV-2 occurred in a variety of clinical settings within KPSC during the study period. Most tests conducted in outpatient settings are submitted to regional laboratories, where more than 90% of samples are processed using the TaqPath COVID-19 Combo Kit. Samples collected in hospitals (including some tests conducted in emergency department settings) are processed using in-house tests, without SGTF readout. In total, 329,195 of 389,896 (84.4%) cases detected in outpatient settings from 1 November 2021 to 17 March 2022 had samples processed using the TaqPath COVID-19 Combo Kit. Attributes of outpatient cases processed using the TaqPath COVID-19 Combo Kit or other assays are presented in Supplementary Table 18. Analyses comparing individuals with Delta and Omicron variant infection were restricted to individuals testing positive between 15 December 2021 and 17 January 2022, encompassing the period during which both variants were detected at >1% prevalence statewide in California, and preceding emergence of the BA.2 Omicron subvariant as a likely cause of S gene detection53. Analyses comparing individuals with BA.2 and BA.1* Omicron subvariant infection were restricted to individuals testing positive between 3 February and 17 March 2022, after the emergence of BA.2 at ≥1% frequency among all individuals (while Delta accounted for <0.1%) and yielding ≥45 days of follow-up for all individuals before the final database lock.
To assess variant-specific differences in risk of progression to severe endpoints in a time-to-event framework, our primary analyses included all individuals diagnosed in outpatient settings with a positive PCR test processed on a TaqPath COVID-19 Combo Kit during the study period who were continuously enrolled in KPSC health plans through the relevant follow-up periods (detailed below) or until their death, whichever was earlier. Restricting to outpatient-diagnosed individuals aimed to address two potential sources of bias: (1) selecting on healthcare-seeking behavior to mitigate confounding that may occur with individuals who deferred testing to more severe stages of illness; and (2) limiting the inclusion of hospital admissions where SARS-CoV-2 infection was detected incidentally, for instance through entry screening. Because hospital admission is a rare event, the number of admissions attributable to factors other than COVID-19 in the time immediately after a positive SARS-CoV-2 test was expected to be low. To ensure that our analyses addressed newly acquired SARS-CoV-2 infections and not PCR-positive detections of remote infections, we excluded individuals with a prior positive SARS-CoV-2 testing result within ≤90 days before their first eligible positive result during the study period.
Analyses included all cases meeting the eligibility criteria defined above and did not use statistical methods to define pre-determined sample sizes. Individuals and healthcare providers did not have access to SGTF determinations in the clinical setting; however, investigators were not blinded to this information or to other case attributes and outcomes for analyses.
Outcome measures
As primary endpoints, we considered five markers of clinically severe illness: any hospital admission, hospital admission associated with new-onset acute respiratory symptoms, ICU admission, mechanical ventilation and mortality. Hospital admissions were considered to be COVID-19 related if they occurred from 7 days before to 30 days after the date of each patient’s positive SARS-CoV-2 RT–PCR test. We included ICU admissions, mechanical ventilation events and deaths occurring up to 60 days after the date of each positive test in the analysis (or up to 45 days after the positive test date for analyses of cases with BA.2 or BA.1* Omicron subvariant infection). Symptomatic hospital admissions were those with acute respiratory infection symptoms beginning on or ≤14 days before the admission date. We ascertained presence of symptoms and dates of symptoms onset via natural language processing of open-text EHR fields, including clinical notes and patient-provided questionnaire responses, which are submitted by all KPSC patients who seek SARS-CoV-2 testing regardless of test setting51. We considered new-onset respiratory symptoms after a positive test as a secondary endpoint for further exploratory analyses among individuals who were asymptomatic at the time of their original test.
Finally, for a duration-of-hospital-stay analysis, we recorded dates of discharge and discharge disposition, in-hospital mortality or censoring for all hospitalized patients. Analyses were restricted to individuals who were tested and admitted to hospital during the periods of 15 December 2021 to 17 January 2022 (for comparisons of individuals with Delta and Omicron variant infection) and 3 February to 17 March 2022 (for comparisons of individuals with BA.2 and BA.1* Omicron subvariant infection); inclusion of individuals diagnosed within these two periods ensured ≥60 days and ≥45 days of follow-up for all individuals from the point of admission. Duration-of-stay analyses included all eligible outpatient-diagnosed individuals from the primary analysis cohort whose samples were processed using the TaqPath COVID-19 Combo Kit and who experienced acute new-symptoms onset respiratory symptoms on or before their admission date.
Considerations for hospital admission
As routine data capture does not include a ‘gold standard’ indication as to whether COVID-19 or another factor served as the primary cause of physician decision to admit a patient, we caution that factors other than SARS-CoV-2 infection (or in conjunction with SARS-CoV-2 infection) may have contributed to hospital admission outcomes as well as ICU admission, use of mechanical ventilation and death, including among individuals with new-onset respiratory symptoms before their admission date, consistent with prior COVID-19 studies using hospital admission endpoints11,14,16,19,20,30,31,35. However, several measures implemented by KPSC to preserve hospital capacity during the COVID-19 pandemic may have lessened the capture of incidental admission events among outpatient-diagnosed individuals within our sample. Outpatient administration of remdesevir and monoclonal antibody therapies was prioritized so that access to treatment would not be grounds for admission. In addition, KPSC used a scoring system to standardize admission versus outpatient management decisions throughout the study period based on individuals’ clinical history and comorbidities (electrolyte disorders, cardiac arrhythmia, neurological disorders, weight loss disorders, congestive heart failure, coagulopathy and diabetes), body mass index, vital signs (oxygen saturation, respiratory rate, systolic blood pressure, fever and heart rate), age and sex36. Based on the resulting scores at the point of testing, individuals were recommended for one of three levels of care provision. Patients not recommended for inpatient admission were either sent home with a telemedicine follow-up from their primary care provider (lowest-risk patients) or enrolled in a home-based monitoring program, for which patients were provided a medical-grade pulse oximeter and thermometer and instructed to enter readings daily into a mobile application to alert physicians in the event of clinical deterioration. Standardized criteria were used for subsequent emergency room referral and hospital admission during subsequent follow-up.
Case attributes
Recorded characteristics of cases included age (defined for all analyses as bands of <1, 1–4, 5–9, 10–19, 20–29, 30–39, 40–49, 50–59, 60–69, 70–79 and ≥80 years), sex, race/ethnicity (White, Black, Hispanic of any race, Asian/Pacific Islander and other/mixed/unknown race), census tract-level median household income (defined on the log scale for all analyses); smoking status (current, former or never smoker); body mass index (underweight, normal weight, overweight and obese); Charlson comorbidity index (0, 1–2, 3–5 and ≥6); prior-year emergency department visits and inpatient admissions (each defined as 0, 1, 2 or ≥3 events); prior-year outpatient visits (0–4, 5–9, 10–14, 15–19, 20–29 or ≥30 events); documented prior SARS-CoV-2 infection; and history of COVID-19 vaccination (unvaccinated, Ad.26.COV2.S as one dose or with a booster and one, two or three mRNA vaccine doses, disaggregating two-dose recipients by time since receipt of the second dose as ≤90 days, 91–180 days or ≥181 days). We compared the distribution of these attributes among individuals with Delta and Omicron variant infection and among individuals with BA.2 or BA.1* Omicron subvariant infection, using logistic regression models defining intercepts for individuals’ testing date and multiple imputation for missing values (as described below in the description of the primary analysis).
Association of SGTF with risk of severe clinical outcomes
Within the primary analysis population, we compared times from the first positive test to each outcome event among patients who tested positive for SARS-CoV-2 by RT–PCR, with and without SGTF. We censored observations at 30 days for hospital admission and symptomatic hospital admission and at 60 days for ICU admission, mechanical ventilation and death (or at 45 days for these endpoints among individuals included in the BA.2/BA.1* analyses). We used Cox proportional hazards models to estimate the aHR for each endpoint associated with SGTF, adjusting for all available demographic and clinical covariates according to the definitions provided above. We defined strata for individuals’ testing date to account for potential secular changes in testing and healthcare practices over the study period, noting that testing dates were jittered at random by 0 days, +1 days or −1 days to preserve anonymity of protected health information; lengths of time to event or censoring were preserved for analysis integrity. We additionally fit models allowing for interactions of SGTF sample status with individuals’ vaccination history to assess variation in the estimated association of SGTF with vaccination status, as described in the primary results above.
Sensitivity analyses
We repeated analyses of the symptomatic hospital admission endpoint within subgroups defined by patient age, sex, Charlson comorbidity index and history of documented SARS-CoV-2 infection and vaccination, controlling for all other risk factors via covariate adjustment. We also conducted secondary analyses including all patients whose tests were processed using the TaqPath COVID-19 Combo Kit, regardless of diagnosis setting. In these analyses, times to events were recorded as 0.5 days for patients experiencing study endpoints on or before the date of their test. These sensitivity analyses aimed to address any bias that could result from exclusion of individuals who progressed rapidly to clinically severe illness; results are presented in Supplementary Table 7 and Supplementary Fig. 3. We also conducted subgroup analyses within the sample of individuals who did not experience symptoms onset on or before their testing date. As a greater likelihood of symptoms among individuals infected with either of the two variants could obscure differences in variant-associated clinical severity (that is, selecting on a differential subset of cases with the otherwise less-severe variant), these analyses aimed to capture a broader spectrum of the clinical course by monitoring individuals from a point preceding symptoms onset. Results are presented in Supplementary Table 8. We summarize symptoms prevalence at the point of presentation to various care settings in Supplementary Table 19 and present attributes of individuals who were tested in outpatient settings with and without symptoms in Supplementary Table 20. Finally, in conjunction with our time-to-event analyses, we estimated aRRs for each clinical outcome using log-binomial regression models defining, as outcomes, any hospital admission or symptomatic hospital admission within 30 days of individuals’ testing date and any ICU admission, mechanical ventilation or mortality within 60 days of individuals’ testing date. Such analyses controlled for all covariates included in Cox proportional hazards models used in the primary analyses and defined intercepts for testing date. Results comparing aHR and aRR estimates are presented in Supplementary Table 11.
We conducted multiple (m = 5) imputation of missing covariate values and pooled results obtained with each imputed dataset via Rubin’s rules54 for our primary analyses (Supplementary Table 21). To verify that our analysis results were not sensitive to the results of imputation, we compared aHR estimates for the association of Omicron versus Delta variant infection with risk of severe outcomes from the primary analysis to results from analyses subset to cases with complete information on all measured characteristics (n = 221,325, 67.3% of the sample) and to results from analyses subset to individuals with ≥1 year of enrollment in KPSC health plans before their diagnosis date (n = 283,453, 86.1% of the sample), among whom fewer observations were missing (Supplementary Table 9). To further demonstrate that missing data did not substantially affect analysis results, we also present estimates of the association of each imputed variable with the outcome of symptomatic hospital admission across the same three analysis strategies in Supplementary Table 22, again identifying similar estimates of association in the primary analysis, in the complete-case analysis and in the analysis subset to individuals with ≥1 year of enrollment in KPSC health plans.
Bias analysis addressing unrecorded prior infection
It has been proposed elsewhere that differential observed severity between Omicron and Delta infections may reflect that Omicron infections occur more commonly among individuals with (often unobserved) prior infection who, thus, are protected by that prior infection against severe outcomes7. We simulated analysis results under scenarios of differential prevalence of unobserved prior infection across case strata to determine whether our findings of reduced severity among individuals with Omicron variant infection could be explained by this circumstance. We defined strata based on the joint distribution of infecting variant i (in recognition of reduced protection against Omicron variant infection conferred by naturally acquired immunity from prior variants41,42), outcome of hospital admission or symptomatic hospital admission j (considering that prior infection would be expected to reduce risk of these outcomes11,55, even if such protection differed by variant) and receipt of any COVID-19 vaccine doses k (assuming that reduced severity of infections acquired after vaccination could lead to reduced likelihood of testing and detection56,57). Here, defining strata based on Omicron variant infection and hospital admission status allowed us to assess how unobserved prior infections could directly affect the primary association of interest to this study. Allowing for an enhanced likelihood that prior infections among vaccinated individuals went unobserved was of interest due to the higher prevalence of prior vaccination among individuals with Omicron variant infection and the possibility that the likelihood of detection of prior infection in a vaccinated individual could be reduced due to the lower severity of post-vaccination infections and relaxed requirements for SARS-CoV-2 testing as a condition for entry into workplaces and indoor public spaces among vaccinated individuals in California in 2021 (per the observed data, prevalence of documented prior infection was 0.80% and 0.38% among individuals who received zero COVID-19 vaccine doses and ≥1 COVID-19 vaccine doses, respectively). Thus, unobserved infections among vaccinated individuals constituted an additional mechanism by which naturally acquired immunity, if present, could be differentially unaccounted for in association with individuals’ infecting variant7.
Defining \(\rho _{ijk}\) as the observed prevalence of prior infection within any stratum, and θ as a multiplier conveying the proportion of infections that would be expected to go unobserved in the stratum of unvaccinated cases with Delta variant infection admitted to hospital, the probability of unobserved prior infection within the i, j, kth stratum was \(\rho _{ijk}(\theta \phi _i\sigma _j\omega _k - 1)\) for values of \(\theta = (1,\,2,\,3,\,4,\,5)\), \(\phi _i = (1,\,2,\,3)\), \(\sigma _j = (1,\,2,\,3)\) and \(\omega _k = (1,\,2,\,3)\). Within each imputed dataset, we assigned prior infection to additional individuals who did not have known prior infection at random according to the probabilities \(\rho _{ijk}(\theta \phi _i\sigma _j\omega _k - 1)\), given their observed outcome and characteristics, and repeated the primary analysis approach using stratified Cox proportional hazards models to estimate the aHR of hospital admission and symptomatic hospital admission outcomes associated with Omicron variant detection. Estimates of the resulting aHR for outcomes of any hospital admission and symptomatic hospital admission are plotted in Supplementary Figs. 1 and 2, respectively.
Period-based analysis
To address concerns about possible bias in our primary analysis that was limited to individuals tested using the TaqPath COVID-19 Combo Kit, we further sought to verify whether the reduced risk of severe clinical outcomes among individuals with Omicron variant infection in the primary analysis was reflected by changes in severe outcomes from Delta-predominant to Omicron-predominant periods. Among all individuals ascertained in outpatient settings (without restriction to individuals tested using TaqPath COVID-19 Combo Kit assays) over the period of 1 November 2021 to 17 January 2022, we estimated aHRs relating the risk of severe clinical endpoints to individuals’ testing date by fitting Cox proportional hazards models. As the goal of these analyses was to relate changes in risk of severe clinical outcomes to timing of the emergence of the Omicron variant in the study population, testing dates were defined as covariates rather than as model strata, as detailed below.
Models were defined allowing for up to two changepoints in the slope of associations between testing date and risk of clinical endpoints, with changepoints defined at all dates in the study period between 15 November 2021 and 10 January 2022. Model formulations with zero, one and two changepoints specified conditional hazards of each outcome given each individual’s observed covariates and testing date, \(\lambda \left( {t{{{\mathrm{|}}}}X_i,\,\tau _i} \right)\), according to
and
respectively. Here, τi defines the testing date; \({{{\mathrm{I}}}}\left( {\tau _i > \theta _k} \right)\) serves an indicator that the testing date occurred after a changepoint in the slope at time θk; and \(X_i^T\alpha\) is the product of all other covariates and their respective regression coefficients. We fit models defining changepoints at each day (or combination of days) through the time series and used the Bayesian information criterion to define model weights:26,58
for a given model m from the state space of all candidate models, \({{{\mathcal{M}}}}\). Posterior model weights divided wm by the number of models fitted with the same number of changepoints, thereby assigning equal prior probability to scenarios with zero, one or two changepoints. We defined testing-date-specific hazards and date-specific changepoint probabilities by sampling models according to their posterior weights. As the sporadic occurrence of mechanical ventilation during the early study period hindered estimation of slopes in risk of this outcome, analyses addressed endpoints of hospital admission, symptomatic hospital admission, ICU admission and death only.
Hospital duration of stay analysis
For admitted individuals diagnosed in outpatient settings with Delta or Omicron variant infection (from 15 December 2021 to 17 January 2022) and BA.2 or BA.1* Omicron subvariant infection (from 3 February to 17 March 2022), we compared times from individuals’ admission date to each of three possible outcomes: discharge home (without skilled care), discharge to any skilled care setting (comprising skilled nursing facilities, residential care facilities, rehabilitation facilities, other acute inpatient hospitals or home with skilled care providers) or to home against medical advice and in-hospital death or discharge to hospice. To compare overall rates of exit from the hospital by infecting lineage, we additionally fit Cox proportional hazards models estimating the aHR of hospital exit (with any final disposition) associated with SGTF status, defining strata on admission date to adjust for any changes in clinical practice over time and controlling for all covariates included in the primary analysis.
Software
We conducted all analyses using R (version 4.0.3, R Foundation for Statistical Computing). We used the survival59 package for time-to-event analyses and the Amelia II60 package for multiple imputation.
Reporting summary
Further information on research design is available in the Nature Research Reporting Summary linked to this article.
Data availability
Individual-level data reported in this study are not publicly shared. Upon reasonable request and subject to review, KPSC may provide the de-identified data that support the findings of this study. De-identified data may be shared upon approval of an analysis proposal and a signed data access agreement. Individuals wanting to access data should contact the KPSC Institutional Review Board at IRB.KPSC@kp.org to enter into a data access agreement.
Code availability
Analysis code is available at https://github.com/joelewnard/omicronSeverity
References
World Health Organization. Update on Omicron variant. https://www.who.int/news/item/28-11-2021-update-on-omicron (2021).
US Centers for Disease Control and Prevention. First confirmed case of Omicron variant detected in the United States. https://www.cdc.gov/media/releases/2021/s1201-omicron-variant.htm (2021).
US Centers for Disease Control and Prevention. COVID-19 Data Tracker: variant proportions. https://covid.cdc.gov/covid-data-tracker/#variant-proportions (2022).
Taylor, L. Covid-19: Omicron drives weekly record high in global infections. BMJ 376, o66 (2022).
Clarke, K. E. N. et al. Seroprevalence of infection-induced SARS-CoV-2 antibodies—United States, September, 2021-February, 2022. MMWR Morb. Mortal. Wkly Rep 71, 606–608 (2022).
US Centers for Disease Control and Prevention. COVID-19 Data Tracker: trends in number of COVID-19 cases and deaths in the US reported to CDC, by state/territory. https://covid.cdc.gov/covid-data-tracker/#trends_dailycases
Matthew, M. et al. Structural basis of SARS-CoV-2 Omicron immune evasion and receptor engagement. Science 375, 864–868 (2022).
Nemet, I. et al. Third BNT162b2 vaccination neutralization of SARS-CoV-2 Omicron infection. N. Engl. J. Med. 386, 492–494 (2022).
Schmidt, F. et al. Plasma neutralization of the SARS-CoV-2 Omicron variant. N. Engl. J. Med. 386, 599–601 (2022).
Altarawneh, H. N. et al. Protection against the Omicron variant from previous SARS-CoV-2 infection. N. Engl. J. Med. 386, 1288–1290 (2022).
Pulliam, J. R. C. et al. Increased risk of SARS-CoV-2 reinfection associated with emergence of Omicron in South Africa. Science 376, eabn4947 (2022).
Tseng, H. F. et al. Effectiveness of mRNA-1273 against SARS-CoV-2 Omicron and Delta variants. Nat. Med. 28, 1063–1071 (2022).
Tartof, S. Y. et al. Durability of BNT162b2 vaccine against hospital and emergency department admissions due to the Omicron and Delta variants in a large health system in the USA: a test-negative case–control study. Lancet Respir. Med https://doi.org/10.1016/S2213-2600(22)00101-1 (2022).
Nyberg, T. et al. Comparative analysis of the risks of hospitalisation and death associated with SARS-CoV-2 Omicron (B.1.1.529) and Delta (B.1.617.2) variants in England: a cohort study. Lancet 399, 1303–1312 (2022).
Pearson, C. A. B. et al. Bounding the levels of transmissibility and immune evasion of the Omicron variant in South Africa. Preprint at https://www.medrxiv.org/content/10.1101/2021.12.19.21268038v1 (2021).
Iuliano, A. D. et al. Trends in disease severity and health care utilization during the early Omicron variant period compared with previous SARS-CoV-2 high transmission periods—United States, December 2020–January 2022. MMWR Morb. Mortal. Wkly Rep. 71, 146–152 (2022).
Public Health England. SARS-CoV-2 variants of concern and variants under investigation in England—Technical briefing: update on hospitalisation and vaccine effectiveness for Omicron VOC-21NOV-01 (B.1.1.529). https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1045619/Technical-Briefing-31-Dec-2021-Omicron_severity_update.pdf (2021).
Madhi, S. A. et al. Population immunity and COVID-19 severity with Omicron variant in South Africa. N. Engl. J. Med. 386, 1314–1326 (2022).
Bager, P. et al. Reduced risk of hospitalisation associated with infection with SARS-CoV-2 Omicron variant versus Delta variant in Denmark: an observational cohort study. Lancert Infect. Dis. https://doi.org/10.1016/S1473-3099(22)00154-2 (2022).
Wolter, N. et al. Early assessment of the clinical severity of the SARS-CoV-2 omicron variant in South Africa: a data linkage study. Lancet 399, 437–446 (2022).
Qassim, S. H. et al. Effects of BA.1/BA.2 subvariant, vaccination, and prior infection on infectiousness of SARS-CoV-2 Omicron infections. Preprint at https://www.medrxiv.org/content/10.1101/2022.03.02.22271771v1 (2022).
Wolter, N., Jassat, W., DATCOV-Gen author group, von Gottberg, A. & Cohen, C. Clinical severity of Omicron sub-lineage BA.2 compared to BA.1 in South Africa. Preprint at https://www.medrxiv.org/content/10.1101/2022.02.17.22271030v1 (2022).
Lesley, S. et al. Track Omicron’s spread with molecular data. Science 374, 1454–1455 (2021).
Andrews, N. et al. Covid-19 vaccine effectiveness against the Omicron (B.1.1.529) variant. N. Engl. J. Med. 386, 1532–1546 (2022).
Stensrud, M. J. & Hernán, M. A. Why test for proportional hazards? JAMA 323, 1401–1402 (2020).
Kürüm, E. et al. Bayesian model averaging with change points to assess the impact of vaccination and public health interventions. Epidemiology 28, 889–897 (2017).
Strålin, K. et al. Impact of the Alpha VOC on disease severity in SARS-CoV-2-positive adults in Sweden. J. Infect. 84, e3–e5 (2022).
Garvey, M. I. et al. Observations of SARS-CoV-2 variant of concern B.1.1.7 at the UK’s largest hospital trust. J. Infect. 83, e21–e23 (2021).
Sheikh, A. et al. Severity of Omicron variant of concern and effectiveness of vaccine boosters against symptomatic disease in Scotland (EAVE II): a national cohort study with nested test-negative design. Lancet Infect. Dis. https://doi.org/10.1016/S1473-3099(22)00141-4 (2022).
Lauring, A. S. et al. Clinical severity of, and effectiveness of mRNA vaccines against, Covid-19 from Omicron, Delta, and Alpha SARS-CoV-2 variants in the United States: prospective observational study. BMJ 376, e069761 (2022).
Ulloa, A. C., Buchan, S. A., Daneman, N. & Brown, K. A. Estimates of SARS-CoV-2 Omicron variant severity in Ontario, Canada. JAMA 327, 1286–1288 (2022).
Peralta-Santos, A. et al. Omicron (BA.1) SARS-CoV-2 variant is associated with reduced risk of hospitalization and length of stay compared with Delta (B.1.617.2). Preprint at https://www.medrxiv.org/content/10.1101/2022.01.20.22269406v1 (2022).
Laxminarayan, R. et al. SARS-CoV-2 infection and mortality during the first epidemic wave in Madurai, south India: a prospective, active surveillance study. Lancet Infect. Dis. 21, 1665–1676 (2021).
Davies, N. G. et al. Increased mortality in community-tested cases of SARS-CoV-2 lineage B.1.1.7. Nature 593, 270–274 (2021).
Davies, N. G. et al. Estimated transmissibility and impact of SARS-CoV-2 lineage B.1.1.7 in England. Science 372, eabg3055 (2021).
Huynh, D. N. et al. Description and early results of the Kaiser Permanente Southern California COVID-19 home monitoring program. Perm. J. 25, 20.281 (2021).
Klann, J. G. et al. Distinguishing admissions specifically for COVID-19 from incidental SARS-CoV-2 admissions: a national retrospective EHR study. Preprint at https://www.medrxiv.org/content/10.1101/2022.02.10.22270728v1 (2022).
Sigal, A., Milo, R. & Jassat, W. Estimating disease severity of Omicron and Delta SARS-CoV-2 infections. Nat. Rev. Immunol. 22, 267–269 (2022).
Bhattacharyya, R. P. & Hanage, W. P. Challenges in inferring intrinsic severity of the SARS-CoV-2 Omicron variant. N. Engl. J. Med. 386, e14 (2022).
Lamba, K. et al. SARS-CoV-2 cumulative incidence and period seroprevalence: results from a statewide population-based serosurvey in California. Open Forum Infect. Dis. 8, ofab379 (2021).
Carreño, J. M. et al. Activity of convalescent and vaccine serum against SARS-CoV-2 Omicron. Nature 602, 682–688 (2022).
Rössler, A., Riepler, L., Bante, D., von Laer, D. & Kimpel, J. SARS-CoV-2 Omicron variant neutralization in serum from vaccinated and convalescent persons. N. Engl. J. Med. 386, 698–700 (2022).
Griffith, G. J. et al. Collider bias undermines our understanding of COVID-19 disease risk and severity. Nat. Commun. 11, 5749 (2020).
Vandenbroucke, J. P., Broadbent, A. & Pearce, N. Causality and causal inference in epidemiology: the need for a pluralistic approach. Int. J. Epidemiol. 45, 1776–1786 (2016).
Hui, K. P. Y. et al. SARS-CoV-2 Omicron variant replication in human bronchus and lung ex vivo. Nature 603, 715–720 (2022).
Abdelnabi, R. et al. The Omicron (B.1.1.529) SARS-CoV-2 variant of concern does not readily infect Syrian hamsters. Antivir. Res 198, 105253 (2022).
Gozzi, N. et al. Preliminary modeling estimates of the relative transmissibility and immune escape of the Omicron SARS-CoV-2 variant of concern in South Africa. Preprint at https://www.medrxiv.org/content/10.1101/2022.01.04.22268721v1 (2022).
Smith, D. J. et al. COVID-19 mortality and vaccine coverage—Hong Kong. MMWR Morb. Mortal. Wkly Rep. 71, 545–548 (2022).
Statistics New Zealand. COVID-19 data portal. https://www.stats.govt.nz/experimental/covid-19-data-portal
The COVID Tracking Project. Long-term-care COVID tracker. https://covidtracking.com/nursing-homes-long-term-care-facilities
Tartof, S. Y. et al. Effectiveness of mRNA BNT162b2 COVID-19 vaccine up to 6 months in a large integrated health system in the USA: a retrospective cohort study. Lancet 398, 1407–1416 (2021).
Koebnick, C. et al. Sociodemographic characteristics of members of a large, integrated health care system: comparison with US Census Bureau data. Perm. J. 16, 37–41 (2012).
California Department of Public Health. Variants in California—COVID-19 Response. https://covid19.ca.gov/variants/
Rubin, D. B. Multiple imputation after 18+ years. J. Am. Stat. Assoc. 91, 473–489 (1996).
León, T. M. et al. COVID-19 cases and hospitalizations by COVID-19 vaccination status and previous COVID-19 diagnosis—California and New York, May–November 2021. MMWR Morb. Mortal. Wkly Rep. 71, 125–131 (2022).
Andrejko, K. L. et al. Prevention of COVID-19 by mRNA-based vaccines within the general population of California. Clin. Infect. Dis. 74, 1382–1389 (2021).
Feikin, D. R. Duration of effectiveness of vaccines against SARS-CoV-2 infection and COVID-19 disease: results of a systematic review and meta-regression. Lancet 399, 924–944 (2022).
Burnham, K. P. & Anderson, D. R. Multimodel inference: understanding AIC and BIC in model selection. Sociol. Methods Res 33, 261–304 (2004).
Therneau, T. M. Package ‘survival’: Survival Analysis. Version 3.3-1. https://cran.r-project.org/web/packages/survival/survival.pdf (2022).
Honaker, J., King, G. & Blackwell, M. Amelia II: a program for missing data. J. Stat. Softw. 45, 1–47 (2011).
Acknowledgements
This work was funded by the US Centers for Disease Control and Prevention (CDC) (grant 75D3–121C11520 to S.Y.T.); M.L., R.J.K. and M.M.P. are employees of this agency. The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the CDC. J.A.L. was supported by grant R01-AI14812701A1 from the National Institute for Allergy and Infectious Diseases (US National Institutes of Health), which had no role in design or conduct of the study or the decision to submit for publication.
Author information
Authors and Affiliations
Contributions
J.A.L., V.X.H., M.M.P., R.K., M.L. and S.Y.T. contributed to the study concept and design. J.A.L., V.X.H. and S.Y.T. led the acquisition and statistical analysis of data. J.A.L., M.M.P., R.K., M.L. and S.Y.T. led the interpretation of data. J.A.L. drafted the manuscript. V.X.H., M.M.P., R.K., M.L. and S.Y.T. critically revised the manuscript for important intellectual content. S.Y.T. obtained funding and provided supervision.
Corresponding authors
Ethics declarations
Competing interests
J.A.L. has received research grants and consulting honoraria unrelated to this study from Pfizer. S.Y.T. has received research grants unrelated to this study from Pfizer. M.L. has received research grants unrelated to this study from Pfizer and has provided unpaid scientific advisory services to Janssen, AstraZeneca, One Day Sooner and Covaxx (United Biomedical). The remaining authors declare no competing interests.
Peer review
Peer review information
Nature Medicine thanks Shabir Madhi and the other, anonymous, reviewer(s) for their contribution to the peer review of this work. Primary handling editor: Alison Farrell, in collaboration with the Nature Medicine team.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Supplementary Information
Supplementary Figs. 1–4 and Supplementary Tables 1–22
Rights and permissions
About this article

Cite this article
Lewnard, J.A., Hong, V.X., Patel, M.M. et al. Clinical outcomes associated with SARS-CoV-2 Omicron (B.1.1.529) variant and BA.1/BA.1.1 or BA.2 subvariant infection in Southern California. Nat Med 28, 1933–1943 (2022). https://doi.org/10.1038/s41591-022-01887-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41591-022-01887-z
This article is cited by
-
Characteristics and outcomes of COVID-19 patients presumed to be treated with sotrovimab in NHS hospitals in England
BMC Infectious Diseases (2024)
-
Clinical course and management of COVID-19 in the era of widespread population immunity
Nature Reviews Microbiology (2024)
-
Artificial Neural Network Prediction of COVID-19 Daily Infection Count
Bulletin of Mathematical Biology (2024)
-
Immune escape of SARS-CoV-2 variants to therapeutic monoclonal antibodies: a system review and meta-analysis
Virology Journal (2023)
-
SARS-CoV-2 before and after Omicron: two different viruses and two different diseases?
Journal of Translational Medicine (2023)
