
Abstract
Radiographic osteoarthritis (OA) is most prevalent in the hand. The association of hand injury with pain or OA is unclear. The objective was to describe the relationship between hand injury and ipsilateral pain and OA in cricketers. Data from former and current cricketers aged ≥ 30 years was used. Data included history of cricket-related hand/finger injury leading to > 4 weeks of reduced exercise, hand/finger joint pain on most days of the last month, self-reported history of physician-diagnosed hand/finger OA. Logistic regression assessed the relationship between injury with hand pain (in former cricketers) and with OA (in all cricketers), adjusted for age, seasons played, playing standard. Of 1893 participants (844 former cricketers), 16.9% reported hand pain, 4.3% reported OA. A history of hand injury increased the odds of hand pain (OR (95% CI) 2.2, 1.4 to 3.6). A history of hand injury also had increased odds of hand OA (3.1, 2.1 to 4.7). Cricket-related hand injury was related to an increased odds of hand pain and OA. This highlights the importance of hand injury prevention strategies within cricket. The high prevalence of hand pain is concerning, and further research is needed to determine the impacts of hand pain.
Similar content being viewed by others
Introduction
Physical activity is known to have a large number of health benefits, and in 2007, the American College of Sports Medicine updated recommendations to encourage increased physical activity participation in the general public1. As participation in exercise and sports increases, the prevalence of injury is likely to increase, and sports-related injury is an important item on the research agenda of the Centers for Disease Control and Prevention2. Half of the sports-related injuries managed in Orthopaedic departments are to the hand3. However, the long-term effects of sports-related hand injury is unclear. In the lower limb, sport-related injury to the knee and hip is an established risk factor for osteoarthritis (OA) development4,5,6,7,8. OA has a large personal and economic health burden, and OA treatment costs have been estimated at £579 per person per annum9. In the hand, symptomatic OA is prevalent in 7% of American adults, increasing to 27% when diagnosed radiographically10, and individuals with hand OA report mental health concerns and poor health-related quality of life11.
In the hand, the relationship between injury and OA is not yet well established. The association between finger fracture from any cause and the development of hand OA was investigated by Jones et al.12 in 522 Tasmanian adults. They found the odds of radiographic distal interphalangeal joint (DIPJ) OA was increased by two-fold in people with a self-reported history of finger fracture. However, finger fracture was not associated with Heberden’s nodes deformities in the DIPJs. It was also not associated with radiographic first carpometacarpal joint (CMCJ) OA. However, Jones et al.13 did not investigate the relationship with symptomatic hand OA. In relation to sports-related hand injury, only one study has investigated the relationship between injury and OA. This study, in retired elite male rugby and cricket players, found no association between severe hand injury and hand OA or pain. However, this study was limited by a small sample and strict inclusion criteria, highlighting the need for further research.
Cricket is a popular world-wide sport with a high prevalence of hand injury14. Understanding the relationship between hand injury and OA may encourage the development and implementation of hand injury prevention strategies, which are not common practice amongst sports with a high risk of hand injury. Identifying individuals at high-risk of hand OA could facilitate early investigations and referrals, and targeted treatments to reduce the risk of developing hand OA (for example, weight-loss strategies and education). The aims of this study were to evaluate the relationship between (i) previous hand injury and ipsilateral hand pain on most days of the past month (commonly used as a marker for symptomatic OA15,16,17) in former cricketers, and (ii) previous hand injury and ipsilateral physician-diagnosed hand OA in current and former cricketers.
Materials and methods
Procedure
28,152 current and former cricket players, registered on a database managed by the England and Wales Cricket Board, who had agreed to be contacted for cricket-related research, were invited to complete an online epidemiological cross-sectional questionnaire (the Cricket Health and Wellbeing Study (CHWS)). All participants were recruited between March and May 2017. To be eligible to participate in the CHWS, individuals must have been aged 18 years or older and played at least 1 season of cricket. People who were potentially eligible were sent one generic email from the England and Wales Cricket Board, with details of the CHWS, eligibility criteria, and a link to the patient information sheet and consent form. 2548 (9.1%) individuals who received an invitation by email believed they met the eligibility criteria and gave informed consent to participate. Of these, 254 were ineligible and therefore excluded, leaving 2294 participants in the CHWS.
Ethical approval
The purpose of the CHWS was to evaluate and explain variation in 5 aspects of health and wellbeing in current and former cricketers (i. cricket-related injury; ii. pain and osteoarthritis; iii. general health and disease; iv. physical activity; v. resilience, quality of life and flourishing). This study investigates pain and osteoarthritis in current and former cricketers. Ethical approval was given by the NHS Health Research Authority (NRES), London Stanmore Research Ethics Committee (REC 15/LO/1274). All participants provided informed consent before proceeding to the questionnaire. This study adhered to guidelines and regulations of the Strengthening the Reporting of Observational studies in Epidemiology (STROBE) Statement18.
The CHWS questionnaire was designed in collaboration with current and former cricketers, and the England and Wales Cricket Board. The questionnaire was developed on REDCap (Research Electronic Data Capture)19,20, hosted at the University of Oxford, with assistance from an experienced database manager. A pilot questionnaire was tested on seven individuals with a range of experience (current and former cricket players, coaching, sports medicine/physiotherapy clinical and research experience). REDCap allowed for branch logic, and participants were able to save their questionnaire progress and resume at a later date. Given the high prevalence of hand injury within cricket, cricketers provide an ideal population to investigate the relationship between hand injury and OA. Data was extracted from the CHWS questionnaire for the current study.
Eligibility criteria
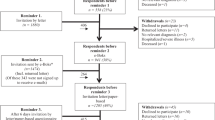
To be eligible for the current study, participants must have been aged 30 years or older at the time of questionnaire completion. Participants with missing data, or ‘don’t know’ responses for joint injury, pain, osteoarthritis, age, playing standard, and length of cricket participation questions were excluded (Fig. 1). Participants who reported using both the right and left hands for bowling and throwing were excluded from a sub-group analyses of dominant and non-dominant hands.

Participant recruitment.
Outcomes
Hand pain
To assess for hand pain, the National Health and Nutrition Examination Survey (NHANES) criteria was used21. Participants were asked, ‘Have you had pain in the [left/right] hand or finger(s) on most days of the last month?’, and ‘Yes/No’ response options were offered.
Hand OA
To assess for a history of physician-diagnosed hand OA, participants were asked ‘Have you ever been told by a doctor that you have osteoarthritis (wear and tear or joint degeneration) in your hand/finger’, ‘Yes/No’ response options were provided. Those responding ‘Yes’ were then prompted to indicate whether their left, right or both hands were affected.
Explanatory variables
Hand injury
Participants were asked ‘have you ever had any cricket-related [hand/finger] injuries leading to more than 4 weeks of reduced participation in exercise, training or sport?’ (‘Yes/No’ response options). Participants then indicated whether they had injured their left, right of both hand(s).
Hand dominance
The dominant hand was defined using the following item, ‘When you bowl or throw do you use your right or left hand?’ (‘Right/Left/Both’ response options). The hand identified was defined as the dominant hand, in the sub-group analyses.
Confounders
Length of cricket participation
Participants were asked ‘Approximately how many seasons have you played cricket for?’ (numerical response).
Playing standard
Participants were asked ‘What was the highest standard of cricket that you played for at least one season?’, (response options were: International, County or Premier league, Academy, County-age-group, University, School, Village or Social). Responses were grouped into higher standard (International/County/Premier league/Academy/County-age-group) and lower standard (University/School/Village/Social).
Statistical analysis
Step-wise logistic regression was used to assess the relationship between hand injury and outcomes (hand pain and hand OA). A hand-level analysis was performed (including both the left and right hands of each participant), whereby the injury status of the left or right hand was assessed in relation to pain/OA in the same (ipsilateral) hand. The relationship between ipsilateral hand injury and hand pain was only assessed in former cricketers, to minimise confounding by pain due to recent cricket-related injury in current players. The relationship between ipsilateral hand injury and hand OA was assessed in all (both current and former) cricketers. Unadjusted and adjusted odds ratios (OR) and 95% confidence intervals (CIs) were calculated for each outcome. All analyses were adjusted for age, number of seasons played, and the highest standard of cricket played (higher/lower standard). All underlying assumptions for logistic regression were checked and satisfied. Due to the small amount of missing data (cricket-related injury: 0.9%, pain: 0.4%, history of OA: 0.1%) and ‘don’t know’ responses (cricket-related injury: 0.9%, pain: 0.3%, history of OA: 2.5%; Fig. 1), a complete case analysis was performed.
Sub-group analysis
A sub-group analysis was performed to compare the relationship between ipsilateral hand injury and pain/OA in the dominant and non-dominant hand. Fifteen current players were excluded (10 ambidextrous, 1 ‘don’t known’ response, 4 missing data for hand dominance), and 12 former players were excluded (8 ambidextrous, 4 missing data for hand dominance).
Results
Participants
Of the 2294 participants in the CHWS, 401 were ineligible and excluded from the current study (n = 223 aged < 30 years, n = 126 ‘don’t know’ responses, and n = 52 did not complete playing standard/length of participation/injury/pain/OA items). Therefore, 1893 CHWS participants met the eligibility criteria for this study (Fig. 1). Of these, 844 (44.6%) were former cricketers and 1049 (55.4%) were currently playing cricket. The mean age of participants (both current and former cricketers) was 54.7 (standard deviation (SD) 12.1) years, participants had played a mean 30.8 (SD 14.4) seasons of cricket, and 1838 (97.1%) were male. A high standard of cricket was played by 703 (37.1%) participants. The mean age of former cricketers was 60.3 (SD 11.2) years, they had played a mean 30.7 (SD 14.2) cricket seasons, and 316 (37.4%) had played at a high standard (Table 1).
The relationship between hand injury and hand pain in former cricketers: 122 (14.5%) former cricketers reported a history of hand injury leading to more than 4 weeks of reduced participation in exercise, training or sport (dominant hand injury: 90 (10.7%), non-dominant hand injury: 83 (9.8%)). 98 (11.6%) individuals reported hand pain on most days of the last month (11.8% of males and 8.7% of females) (Table 1).
Hand injury was associated with a greater odds of ipsilateral hand pain (OR 2.3, 95% CI 1.5 to 3.6). After adjustment for age, length of participation and playing standard, this relationship remained (2.2, 1.4 to 3.6) (Table 2).
In the sub-group analysis, hand injury was associated with a greater odds of ipsilateral hand pain in both the dominant (2.1, 1.1 to 3.9) and non-dominant hand (2.2, 1.1 to 4.4). This relationship remained after adjusting for covariates, (dominant hand: 2.0, 1.0 to 3.9, non-dominant hand: 2.1, 1.0 to 4.4) (Table 2).
The relationship between hand injury and hand OA in current and former cricketers
In all cricketers, 315 (16.6%) individuals reported a history of hand injury (dominant hand injury: 247 (13.0%), non-dominant hand injury: 228 (12.0%). 81 (4.3%) participants had been diagnosed with hand OA (4.4% of males and 2.3% of females) (Table 1). Hand injury was associated with an increased odds of ipsilateral hand OA (2.6, 1.7 to 3.8), and this relationship remained after adjustment for all confounders (3.1, 2.1 to 4.7) (Table 3).
In the sub-group analysis, hand injury was associated with an increased odds of ipsilateral hand OA in the dominant hand (2.2, 1.3 to 3.9), and non-dominant hand (2.6, 1.4 to 4.9). These relationships remained after adjusting for covariates (dominant hand: 2.7, 1.5 to 4.6; non-dominant hand: 3.2, 1.7 to 6.1 (Table 3).
Discussion
This is the first study to find a relationship between hand injury and an increased odds of ipsilateral hand pain in former cricketers, and a relationship between hand injury and an increased odds of ipsilateral hand OA in both current and former cricketers. These associations remained after adjustment for age, length of cricket participation, and playing standard. Our results contrast findings from Jones et al., whom found no association between hand injury and pain (on most days of the past month) or a diagnosis of hand OA (using the same criteria as our study)13. However, their sample size was only 200 cricket players, with an OA prevalence of 2.4%, and therefore might have been underpowered to detect an effect. Our study included both male and female players, who played at both recreational and elite levels. By using a larger sample size in our study, we might be more likely to identify an association between injury and pain/OA, if one exists.
Due to the cross-sectional nature of our study, we could not imply a causal relationship between hand injury and pain or OA. Similarly, risk factors for the progression of IPJ OA are not yet well understood22. It is possible that other factors could explain the observed relationship. In a recent study involving participants from the CHWS, former elite cricketers were found to have a greater odds of hand pain, compared to former recreational cricketers23, and this relationship remained after adjustment for hand injury. We adjusted for playing standard in our analysis, and the positive relationship between hand injury and hand pain/OA remained. Research also suggests that high grip strength is a risk factor for hand OA24. Sports such as golf, hockey and tennis demand high grip strength25. In these sports, a ‘power’ style grip is used to hold a stick or bat26. A similar grip is used by cricketers when batting, a position which all players are required to partake in if an innings is completed. This type of grip exerts remarkably high compressive forces across the hand joints, particularly the proximal interphalangeal joints (PIPJs), the first metacarpophalangeal joint and the first CMCJ27,28. These forces might be on the causal pathway for hand OA. However, to our knowledge, the association between grip strength and compressive forces with hand pain and OA have not yet been studied in cricketers. To more accurately assess hand injury as a risk factor for pain and OA, prospective longitudinal studies, adjusted for potential risk factors such as grip strength, are required.
Pain is a common symptom of OA. However, for hand OA, there is not yet established criteria to measure the presence and severity of pain, separate from other symptoms of hand OA. Self-reported questionnaires to measure hand function in patients with hand OA include questions relating to pain29. In particular, the Arthritis Impact Measurement 2 Short Form (AIMS2-SF) questionnaire30, Score for Assessment and Qualification of Chronic Rheumatoid Affections of the Hands (SACRAH) questionnaire31 and the Australian/Canadian (AUSCAN) Osteoarthritis Health Index32,33 include questions regarding pain in the hand joints. However, when using these questionnaires, the questions relating only to pain cannot be interpreted separately from other questions. NHANES pain is often used as an OA outcome measure in the lower limb15,16,17. Therefore, in our study, we chose to use NHANES pain in the hand as a surrogate for the prevalence of hand OA. Our results showed similar associations between injury and NHANES pain in the hand, and between injury and hand OA. This suggests that the NHANES criteria for hand pain may be a good marker for symptomatic hand OA. Pain from hand OA has been described as having a diurnal pattern34. However, as the NHANES criteria measures pain cross-sectionally, it might be under-reported due to its fluctuating nature. The NHANES criteria also does not differentiate between pain at different joints of the hand, such as an interphalangeal joint (IPJ) and base of thumb. Pain from base of thumb OA can radiate distally to the IPJs, or proximally to the wrist35. Therefore, there is a chance the pain measured in our study might not correlate with the anatomical site of injury on the hand. Future research should aim to develop questionnaires to assess pain longitudinally and to differentiate between pain at different anatomical sites, such as by specifying individual joints or by asking about the presence of tenderness when a particular joint is moved.
Hand pain on most days of the past month was reported by 11.6% of former cricketers (11.8% of males and 8.7% of females). Cai et al.23 found that the hand was the third most common site where pain was reported on most days of the past month by former cricketers from the CHWS (the most common sites were the knee and back). In a general population study of men and women aged 25–65 years whom were residents of the United Kingdom (UK), the prevalence of hand or wrist pain (defined as pain lasting 1 day or longer in the last 7 days) was 8.7% in men and 11.5% in women36. Notably, fewer people are likely to experience hand pain on most days of the past month compared to hand or wrist pain lasting at least 1 day in the last 7 days. Despite this, a greater proportion of former male cricketers reported hand pain compared to males from a general UK population sample. Although our findings suggest hand pain may be less prevalent in female former cricketers compared with the general population, further research is needed due to the small number of females in our study and the heterogeneous criteria used to categorise hand pain.
The high prevalence of hand pain is particularly concerning as pain from hand OA has been described as being as severe as that from rheumatoid arthritis37. Hand pain due to OA has also been associated with poor health-related quality of life (HRQoL), and mental health concerns11. However, a recent CHWS study in former cricketers found that persistent upper extremity pain was not associated with worse mental component scores (measured with the Short-Form 8 Health Survey), compared to former cricketers without joint pain38. Bullock et al.38 suggest this might be due to psychological strengths common amongst cricketers, allowing them to cope better with adversity, such as pain. Despite no association with mental component scores, Bullock et al.38 found persistent upper extremity pain was associated with worse physical component scores, compared to former cricketers without persistent joint pain, and this exceeded the minimal clinically important difference for this measure. However, no study has specifically looked at the impact of persistent hand pain or hand OA on physical and mental components of HRQoL in former cricketers. It is possible that persistent hand pain in former cricketers has a negative impact on participation in physical activity, work duties or family roles. Qualitative research in former cricketers could provide valuable insights into the physical and mental burden of living with persistent hand pain.
Given the high prevalence of hand injuries reported in this study, there is a need to develop injury prevention strategies for cricket players of all playing standards. In stick-handling sports, the odds of hand/finger injuries and fractures are significantly higher in athletes not using gloves, compared to those using gloves39. In cricket, only batsmen and wicketkeepers are permitted to wear gloves. Despite batsmen wearing gloves, Jones et al.13 found the highest prevalence of severe hand injury in cricketers was in batsmen. This suggests that the use of personal protective equipment might not be adequate to prevent hand injury in cricketers. Instead, strategies focused on neuromuscular exercise, proprioception and strength training, could be more effective. These strategies have been shown to be successful in lower limb injury prevention40,41. However, to our knowledge, injury prevention strategies for the hand have not yet been developed or evaluated. Novel strategies such as these might decrease the incidence of hand injuries, with potential to reduce the burden of symptomatic hand OA.
The participant recruitment strategy was chosen to reach a large, diverse sample of cricketers in the UK. However, a limitation of this recruitment strategy was that we could not determine the response rate or assess for non-response bias. It is, however, possible that cricketers with a particular concern in health and wellbeing were more likely to respond to this questionnaire, introducing a selection bias. Notably, this is a cross-sectional study and all data was collected through self-reported questionnaires, increasing the risk of recall bias. Due to the nature of the questionnaire, we could not reliably assess which hand structures were injured, and it is possible that some injuries did not involve the joints. Similarly, we were unable to account for injuries occurring during other activities. Longitudinal studies are required to more accurately characterise the relationship between hand injuries, confounders and injury/OA. Pain on most days of the past month may be a surrogate for OA in former cricketers21. However, in current cricketers where hand injury is prevalent, pain on most days of the past month may reflect an acute hand injury. Since exploring acute pain following hand injury does not align with the objectives of this study, we only investigated the relationship between injury and pain in former cricketers. We assessed hand OA in both current and former cricketers, and despite current cricketers having similar characteristics to former cricketers in our study, it is possible that there were other unmeasured differences between the two groups, which we were unable to account for. Additionally, OA was assessed through a self-reported history of a physician diagnosis. The health-seeking behaviour of cricketers is not well described in the literature, and considering the high rate of persistent hand pain, it is likely that some cricketers had not visited a physician or been assessed for hand OA. It is therefore likely that hand OA is under-reported in this sample.
Additionally, this study did not differentiate between CMCJ OA and (IPJ OA. CMCJ and IPJ OA are thought to be different subsets of hand OA, and therefore might have differing underlying pathologies and aetiologies42. Future studies should assess these anatomical sites separately. The number of females in our study was low. However, female gender is known to be associated with incident hand OA43, and though previous studies have described injuries sustained by female cricketers44,45, further work is needed to better understand the association between hand pain and OA with injury in female cricketers.
Data availability
The datasets generated during this study are available from the senior author on reasonable request.
References
Haskell, W. L. et al. Physical activity and public health: updated recommendation for adults from the American college of sports medicine and the American heart association. Med. Sci. Sports Exerc. 39, 1423–1434. https://doi.org/10.1249/mss.0b013e3180616b27 (2007).
Weiss, A. J. & Elixhauser, A. in Healthcare cost and utilization project (hcup) statistical briefs (Agency for Healthcare Research and Quality (US), 2006).
Simpson, D. & McQueen, M. M. Acute sporting injuries to the hand and wrist in the general population. Scott. Med. J. 51, 25–26. https://doi.org/10.1258/rsmsmj.51.2.25 (2006).
Lohmander, L. S., Ostenberg, A., Englund, M. & Roos, H. High prevalence of knee osteoarthritis, pain, and functional limitations in female soccer players twelve years after anterior cruciate ligament injury. Arthritis Rheum. 50, 3145–3152. https://doi.org/10.1002/art.20589 (2004).
Golightly, Y. M., Marshall, S. W., Callahan, L. F. & Guskiewicz, K. Early-onset arthritis in retired national football league players. J. Phys. Act Health 6, 638–643 (2009).
Deacon, A., Bennell, K., Kiss, Z. S., Crossley, K. & Brukner, P. Osteoarthritis of the knee in retired, elite australian rules footballers. Med. J. Aust. 166, 187–190 (1997).
Fernandes, G. S. et al. Prevalence of knee pain, radiographic osteoarthritis and arthroplasty in retired professional footballers compared with men in the general population: a cross-sectional study. Br. J. Sports. Med. 52, 678–683. https://doi.org/10.1136/bjsports-2017-097503 (2018).
Cooper, D. J., Scammell, B. E., Batt, M. E. & Palmer, D. Factors associated with pain and osteoarthritis at the hip and knee in great Britain’s olympians: a cross-sectional study. Br. J. Sports Med. 52, 1101–1108. https://doi.org/10.1136/bjsports-2017-098315 (2018).
Sandell, L. J. Etiology of osteoarthritis: genetics and synovial joint development. Nat. Rev. Rheumatol. 8, 77–89. https://doi.org/10.1038/nrrheum.2011.199 (2012).
Lawrence, R. C. et al. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States. Part II. Arthritis Rheum. 58, 26–35. https://doi.org/10.1002/art.23176 (2008).
Michon, M., Maheu, E. & Berenbaum, F. Assessing health-related quality of life in hand osteoarthritis: a literature review. Ann. Rheum. Dis. 70, 921–928. https://doi.org/10.1136/ard.2010.131151 (2011).
Jones, G., Cooley, H. M. & Stankovich, J. M. A cross sectional study of the association between sex, smoking, and other lifestyle factors and osteoarthritis of the hand. J. Rheumatol. 29, 1719–1724 (2002).
Jones, M. E. et al. The prevalance of hand and wrist osteoarthritis in elite cricket and rugby union players. J. Sci. Med. Sport 22, 871–875 (2019).
Ranson, C., Hurley, R., Rugless, L., Mansingh, A. & Cole, J. International cricket injury surveillance: a report of five teams competing in the ICC cricket world cup 2011. Br. J. Sports Med. 47, 637–643. https://doi.org/10.1136/bjsports-2012-091783 (2013).
Leyland, K. M. et al. Harmonising measures of knee and hip osteoarthritis in population-based cohort studies: an international study. Osteoarthr. Cartil. 26, 872–879. https://doi.org/10.1016/j.joca.2018.01.024 (2018).
Felson, D. T. et al. Defining radiographic osteoarthritis for the whole knee. Osteoarthr. Cartil. 5, 241–250 (1997).
National Center for Health Statistics. Basic data on arthritis knee, hip, and sacroiliac joints, in adults ages 25–74 years, united states, 1971–1975. Vital Health Stat. 11, 1–8 (1979).
von Elm, E. et al. The strengthening the reporting of observational studies in epidemiology (strobe) statement: guidelines for reporting observational studies. Int. J. Surg. 12, 1495–1499. https://doi.org/10.1016/j.ijsu.2014.07.013 (2014).
Harris, P. A. et al. Research electronic data capture (redcap)–a metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 42, 377–381. https://doi.org/10.1016/j.jbi.2008.08.010 (2009).
Harris, P. A. et al. The redcap consortium: Building an international community of software platform partners. J. Biomed. Inform. 95, 103208. https://doi.org/10.1016/j.jbi.2019.103208 (2019).
CDC. In 2003–2004 Data Documentation, Codebook, and Frequencies (ed Centers for Disease Control and Prevention) (2003).
Shah, K., Yang, X., Lane, J. C. E., Collins, G. S., Arden, N. K., Furniss, D. & Filaby, S. R. Risk factors for the progression of finger interphalangeal joint osteoarthritis: a systematic review. Rheumatol Int.. 40, 1781–1792. https://doi.org/10.1007/s00296-020-04687-1 (2020).
Cai, H. et al. Joint pain and osteoarthritis in former recreational and elite cricketers. BMC Musculoskelet. Disord. 20, 596. https://doi.org/10.1186/s12891-019-2956-7 (2019).
Chaisson, C. E., Zhang, Y., Sharma, L., Kannel, W. & Felson, D. T. Grip strength and the risk of developing radiographic hand osteoarthritis: results from the framingham study. Arthritis Rheum. 42, 33–38. https://doi.org/10.1002/1529-0131(199901)42:1%3c33::Aid-anr4%3e3.0.Co;2-i (1999).
Cronin, J., Lawton, T., Harris, N., Kilding, A. & McMaster, D. T. A brief review of handgrip strength and sport performance. J. Strength Cond. Res. 31, 3187–3217. https://doi.org/10.1519/jsc.0000000000002149 (2017).
Young, R. W. Evolution of the human hand: the role of throwing and clubbing. J. Anat. 202, 165–174. https://doi.org/10.1046/j.1469-7580.2003.00144.x (2003).
An, K. N., Chao, E. Y., Cooney, W. P. & Linscheid, R. L. Forces in the normal and abnormal hand. J. Orthop. Res. 3, 202–211. https://doi.org/10.1002/jor.1100030210 (1985).
Cooney, W. P. 3rd. & Chao, E. Y. Biomechanical analysis of static forces in the thumb during hand function. J. Bone Joint Surg. Am. 59, 27–36 (1977).
Stamm, T. et al. Measuring functioning in patients with hand osteoarthritis–content comparison of questionnaires based on the international classification of functioning, disability and health (ICF). Rheumatology (Oxford) 45, 1534–1541. https://doi.org/10.1093/rheumatology/kel133 (2006).
Meenan, R. F., Mason, J. H., Anderson, J. J., Guccione, A. A. & Kazis, L. E. Aims2. The content and properties of a revised and expanded arthritis impact measurement scales health status questionnaire. Arthritis Rheumatol. 35, 1–10. https://doi.org/10.1002/art.1780350102 (1992).
Leeb, B. F., Sautner, J., Andel, I. & Rintelen, B. Sacrah: a score for assessment and quantification of chronic rheumatic affections of the hands. Rheumatology (Oxford) 42, 1173–1178. https://doi.org/10.1093/rheumatology/keg319 (2003).
Bellamy, N. et al. Clinimetric properties of the auscan osteoarthritis hand index: an evaluation of reliability, validity and responsiveness. Osteoarthr. Cartil. 10, 863–869 (2002).
Bellamy, N. et al. Dimensionality and clinical importance of pain and disability in hand osteoarthritis: development of the Australian/Canadian (auscan) osteoarthritis hand index. Osteoarthr. Cartil. 10, 855–862 (2002).
Bellamy, N., Sothern, R. B., Campbell, J. & Buchanan, W. W. Rhythmic variations in pain, stiffness, and manual dexterity in hand osteoarthritis. Ann. Rheum. Dis. 61, 1075–1080. https://doi.org/10.1136/ard.61.12.1075 (2002).
Anakwe, R. E. & Middleton, S. D. Osteoarthritis at the base of the thumb. BMJ 343, d7122. https://doi.org/10.1136/bmj.d7122 (2011).
Walker-Bone, K., Palmer, K. T., Reading, I., Coggon, D. & Cooper, C. Prevalence and impact of musculoskeletal disorders of the upper limb in the general population. Arthritis Rheum. 51, 642–651. https://doi.org/10.1002/art.20535 (2004).
Kjeken, I. et al. Activity limitations and participation restrictions in women with hand osteoarthritis: patients’ descriptions and associations between dimensions of functioning. Ann. Rheum. Dis. 64, 1633–1638. https://doi.org/10.1136/ard.2004.034900 (2005).
Bullock, G. S., Collins, G., Peirce, N., Arden, N. K. & Filbay, S. R. Physical activity and health-related quality of life in former elite and recreational cricketers from the uk with upper extremity or lower extremity persistent joint pain: a cross-sectional study. BMJ Open 9, e032606. https://doi.org/10.1136/bmjopen-2019-032606 (2019).
Bowers, A. L., Baldwin, K. D. & Sennett, B. J. Athletic hand injuries in intercollegiate field hockey players. Med. Sci. Sports Exerc. 40, 2022–2026. https://doi.org/10.1249/MSS.0b013e318182afe3 (2008).
Dargo, L., Robinson, K. J. & Games, K. E. Prevention of knee and anterior cruciate ligament injuries through the use of neuromuscular and proprioceptive training: an evidence-based review. J. Athl. Train. 52, 1171–1172. https://doi.org/10.4085/1062-6050-52.12.21 (2017).
Mehl, J. et al. Evidence-based concepts for prevention of knee and acl injuries. 2017 guidelines of the ligament committee of the german knee society (dkg). Arch. Orthop. Trauma Surg. 138, 51–61. https://doi.org/10.1007/s00402-017-2809-5 (2018).
Reginster, J. L. et al. Guidelines for the conduct of pharmacological clinical trials in hand osteoarthritis: consensus of a working group of the European society on clinical and economic aspects of osteoporosis, osteoarthritis and musculoskeletal diseases (ESCEO). Semin. Arthritis Rheum. 48, 1–8. https://doi.org/10.1016/j.semarthrit.2017.12.003 (2018).
Zhang, Y. & Jordan, J. M. Epidemiology of osteoarthritis. Clin. Geriatr. Med. 26, 355–369. https://doi.org/10.1016/j.cger.2010.03.001 (2010).
Panagodage Perera, N. K., Kemp, J. L., Joseph, C. & Finch, C. F. Epidemiology of hospital-treated cricket injuries sustained by women from 2002–2003 to 2013–2014 in Victoria, Australia. J. Sci. Med. Sport 22, 1213–1218. https://doi.org/10.1016/j.jsams.2019.07.010 (2019).
Panagodage Perera, N. K., Kountouris, A., Kemp, J. L., Joseph, C. & Finch, C. F. The incidence, prevalence, nature, severity and mechanisms of injury in elite female cricketers: A prospective cohort study. J Sci Med Sport22, 1014-1020. https://doi.org/10.1016/j.jsams.2019.05.013 .
Acknowledgements
The authors would like to thank the England and Wales Cricket Board for their assistance with recruitment for this study, and the participants for taking part in this study.
Author information
Authors and Affiliations
Contributions
K.S., D.F., G.S.C., N.P., N.K.A, S.R.F. conceived the study idea. K.S., D.F., G.S.C., N.P., N.K.A., S.R.F. were involved in the methodological design and planning. S.R.F., N.P. and N.A. designed the questionnaire. S.R.F. and N.P. recruited participants. K.S. performed statistical analysis. K.S. and S.R.F. wrote the first draft of the manuscript. K.S., D.F., G.S.C., N.P., N.K.A., S.R.F. critically revised the manuscript. K.S., D.F., G.S.C., N.P., N.K.A., S.R.F. approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
KS is funded by the British Society for Surgery of the Hand. DF and GC are funded by the NIHR Oxford Biomedical Research Centre. NKA and SRF are funded by the Centre for Sports, Exercise and Osteoarthritis Research Versus Arthritis. NP is Chief Medical Officer for the England and Wales Cricket Board but receives no external funding. This study was funded by the Centre for Sports, Exercise and Osteoarthritis Research Versus Arthritis (Grant Reference 21595). Study sponsors had no involvement in the study design, collection, analysis and interpretation of data, writing of the manuscript, and in the decision to submit for publication.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Shah, K., Furniss, D., Collins, G.S. et al. Cricket related hand injury is associated with increased odds of hand pain and osteoarthritis. Sci Rep 10, 16775 (2020). https://doi.org/10.1038/s41598-020-73586-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-020-73586-z
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
