
Abstract
Societies value the marine environment for its health-promoting potential. In this preregistered study, we used cross-sectional, secondary data from the Seas, Oceans, and Public Health In Europe (SOPHIE) and Australia (SOPHIA) surveys to investigate: (a) relationships of self-reported home coastal proximity and coastal visits with self-reported general health; (b) the potential of both to buffer income-related health inequalities; and (c) the generalizability of these propositions across 15 countries (n = 11,916–14,702). We find broad cross-country generalizability that living nearer to the coast and visiting it more often are associated with better self-reported general health. These results suggest that coastal access may be a viable and generalized route to promote public health across Europe and Australia. However, the relationships are not strongest among individuals with low household incomes, thereby challenging widespread assumptions of equigenesis that access to coastal environments can buffer income-related health inequalities.
Similar content being viewed by others


Introduction
Societies value the marine environment for various reasons, including its health-promoting potential. Five single-country studies from the United Kingdom1,2,3, Belgium4, and Spain5 (for details, see Supplementary Notes 1) found that individuals who lived nearer to the coast reported better health than those living further away. Supporting this cross-sectional research, a longitudinal study in England6 showed that individuals reported better general health in years when they lived within 5 km of the coast compared to years when they lived further away.
The relationship between living nearer to the coast and better health may result from reduced exposure to some environmental hazards (e.g., air pollution, but the evidence is mixed4), more physical activity (e.g., walking1,7), and/or opportunities for indirect contact (e.g., views from home) which are associated with lower psychological distress8. Moreover, living nearer to the coast is associated with more frequent coastal visits9.
Coastal visit frequency may benefit health because it promotes longer bouts of and/or higher intensity forms of physical activity10, social interactions, and psychological restoration from stress11, which can help reduce allostatic load6. Given that coastal visit frequency drops exponentially as a function of home distance, these benefits are likely to show diminishing marginal returns with increasing home distance4.
Despite these studies, a systematic review in 20177 concluded that the evidence for the relationship between exposure (especially visits) to blue spaces (including coastal environments) and a range of different health metrics was insufficient, in part because it was based on relatively few single-country studies with inconsistent health outcomes. Furthermore, previous research into marine settings and health has mainly focused on the direct relationship between nature contact and health, while its role as a potential modifier is under-researched12.
One modifier of interest relates to the equigenesis hypothesis13, which posits that contact with nature more generally may mitigate or buffer adverse relationships between health risk factors (e.g., low area or household income) and health outcomes12,14. Buffering and mitigating in this article do not imply causality but mean that a relationship (e.g., between income and health) is weaker under certain circumstances (e.g., with more frequent nature contact). Consistent with the equigenesis hypothesis, a recent systematic review15 and several studies13 found that green spaces seemed to buffer the relationship of socioeconomic status and income with health outcomes. Other studies showed no effect15 or a reverse effect, such that green spaces were associated with poorer health in low-income suburban areas16. Regarding coastal contact, two studies from England suggest that living nearer to the coast mitigates the relationship between income deprivation and both self-reported general3 and mental17 health.
In this study, we investigated: (a) relationships of both self-reported home coastal proximity and coastal visits with self-reported general health; (b) the potential of both to buffer income-related health inequalities; and (c) the generalizability of these propositions across 15 countries, using a Bayesian approach to quantify the relative support for or against any relationships. We analyzed cross-sectional, secondary data from the Seas, Oceans, and Public Health In Europe (SOPHIE) and Australia (SOPHIA) surveys which collected samples representative in terms of age, sex, and region from 14 European countries and Australia, respectively.
We expected that both living nearer to the coast (Hypothesis 1) and visiting it more often (Hypothesis 2) would predict better self-reported general health. We also expected that living nearer to the coast (Hypothesis 3) and visiting it more often (Hypothesis 4) would mitigate any adverse relationship between household income and health, such that this relationship would be weaker when individuals live nearer to the coast or visit it more often. We additionally examined generalization across countries in terms of both the proposed relationships (Research Question 1) and the potential modifier (Research Question 2).
The present work advances research in four key ways. First, this study goes beyond the relationship of self-reported general health with home coastal proximity to explore its relationship with direct coastal contact (coastal visits). Second, this study investigates the potential modifying role of coastal proximity and visits on the relationship between household income and health. Investigating coastal contact as a potential modifier is important because it may provide “leverage points for intervention”12 to reduce income-related health inequalities, in addition to policies that focus on reducing income inequality directly. Third, in contrast to previous single-country studies, this study includes samples from 14 European countries and Australia, representative in terms of age, sex, and region. This allows us to test the generalizability of any relationships found across countries. Lastly, we use a Bayesian analytical approach which allows for quantifying the relative support for or against any relationships, provides rich information about the strength of evidence, and is valid for every sample size, including large samples18. This approach paves the way for future studies to use the current findings (posterior distributions) as prior knowledge (prior distributions) for an informed and accumulated estimation of the effects19. This way, the present study provides a robust, high-quality test of the relationships between two types of coastal contact, proximity and visits, and health.
Results
Descriptive statistics for self-reported general health depending on (a) self-reported home coastal proximity and (b) self-reported coastal visits are listed in Supplementary Notes 2.
Relationship of home coastal proximity (Hypothesis 1) and coastal visits (Hypothesis 2) with health
We investigated whether living nearer to the coast (Hypothesis 1; n = 13,620; 14 countries excluding Czechia) and visiting it more often (Hypothesis 2; n = 14,702; 15 countries) predict better self-reported general health and whether these relationships generalize across countries (Research Question 1). The model with monotonic proximity/visits and a random slope (Model 4) provides the best predictive ability, although differences in LOOIC are small (Supplementary Notes 3).
Controlling for age, sex, and household income, we find very strong evidence for Hypothesis 1 that living nearer to the coast predicts better self-reported health within countries (BF+- = 82.33, b = 0.02, SE = 0.01, 90% CrI [0.01, 0.03]). A Bayes factor of 82.33 implies that the data are 82.33 times more likely under the hypothesis that the proximity-health relationship is positive (H+) rather than negative (H−).
Due to the coding of home coastal proximity (lower values =living nearer to the coast) and health (lower values = better health), a positive association means that living nearer to the coast is associated with better health. A slope of 0.02 means that, on average, self-reported general health increases by 0.02 SD with every unit of living nearer to the coast within a country. Importantly, the largest improvement in health when living nearer to the coast, namely 37.9% (90% CrI [7.7%, 64.7%]) of the total improvement, happens between <1 km and 1–2 km. For the other adjacent coastal distance categories, the improvement in health ranges from 6.7% (90% CrI [0.3%, 20.4%]) for 2–5 km and 5–10 km to 18.2% (90% CrI [1.6%, 42.2%]) for 50–100 km to >100 km.
Given this model and the prior distributions as well as keeping all covariates constant, individuals who live within 1 km of the coast are 1.22 and 1.06 times more likely to report very good (10.4%) or good (45.7%) health compared to those who live more than 100 km from the coast (very good: 8.5%, good: 43.2%). Reporting fair, bad, or very bad health are 1.07, 1.19, and 1.31 times more common among individuals who live more than 100 km from the coast (fair: 36.7%, bad: 9.2%, very bad: 2.4%) compared to those who live within 1 km of the coast (fair: 34.3%, bad: 7.7%, very bad: 1.8%; Fig. 1a).

Note. a Marginal effects of home coastal proximity on health. b Marginal effects of coastal visits on health. Probability (y-axis) refers to the probability of choosing each health category. These probabilities sum up to 1 per category of a home coastal proximity and b visits. Points in a, b represent the posterior mean of the probability of self-reported general health in five categories from 1 ‘Very good’ to 5 ‘Very bad’ (indicated by the five colors), depending on a home coastal proximity and b coastal visits. The error bars indicate the 90% credible interval, including the random effects variance across countries.
The evidence for this hypothesis varies across countries, from BF+- = 2.24 in Italy to BF+- = 341.86 in Norway, but always supports a positive relationship. Overall, half of the countries (Australia, Belgium, Bulgaria, Greece, Ireland, Norway, and Poland) show at least strong evidence of an association, while the other half (France, Germany, Italy, the Netherlands, Portugal, Spain, and the United Kingdom) show insufficient to moderate evidence. Nevertheless, the magnitude of this relationship is similar across countries, as indicated by the overlapping credible intervals (Fig. 2a). Overall, the proximity-health relationship generalizes across countries.

Note. a Posterior distributions by country for the average monotonic effect of home coastal proximity on health. b Posterior distributions by country for the average monotonic effect of coastal visits on health. The blue area represents the posterior distribution, and the black dot the average monotonic effect of a home coastal proximity and b coastal visits on self-reported health per county. The error bars indicate the 90% credible interval. For example, in a, a value of 0.04 for Greece means that, on average, self-reported general health improves by 0.04 SD with every one-unit decrease in home coastal distance in Greece.
In line with Hypothesis 2, more coastal visits predict better self-reported health within countries (BF+- → ∞, b = 0.11, SE = 0.02, 90% CrI [0.08, 0.13]) when controlling for age, sex, and income. The slope of 0.11 indicates that, on average, self-reported general health increases by 0.11 SD with every one-unit increase in coastal visits. Of note, 13.3% (90% CrI [4.4%, 22.5%]) of the total increase in health when visiting the coast more often happens between the first two categories (‘once a week or more often’ and ‘once every 2 or 3 weeks’), whereas 53.4% (90% CrI [44.5%, 61.8%]) happens between the last two categories (‘once or twice a year’ and ‘never’).
Based on this model and the prior distributions as well as keeping all covariates constant, individuals who visit the coast at least once a week are 2.60 and 1.36 times more likely to report very good (12.4%) or good (47.8%) health than those who never visit it (very good: 4.8%, good: 35.3%). Reporting fair, bad, or very bad health is 1.30, 2.13, and 3.29 times more common among individuals who never visit the coast (fair: 41.7%, bad: 13.7%, very bad: 4.5%) compared to those who visit it at least once a week (fair: 32.0%, bad: 6.4%, very bad: 1.4%; Fig. 1b).
In all countries except Italy, there is at least strong evidence for a positive relationship between coastal visits and self-reported health. However, the magnitude of this relationship differs between countries, as indicated by non-overlapping credible intervals (Fig. 2b). The positive relationship between visits and health is strongest in Ireland (BF+- → ∞, b = 0.18, SE = 0.03, 90% CrI [0.13, 0.24]) and more positive than in Belgium, France, Italy, the Netherlands, and Spain. The relationship is second strongest in Greece (BF+- = 11,999.00, b = 0.16, SE = 0.04, 90% CrI [0.09, 0.23]), which is different from the one in Italy. Overall, the visits-health relationship seems to generalize across countries in terms of presence but not magnitude.
Home coastal proximity (Hypothesis 3) and coastal visits (Hypothesis 4) as a potential ‘buffer’ on the relationship between household income and health
We investigated whether home coastal proximity (Hypothesis 3; n = 11,916; 14 countries excluding Czechia) and coastal visits (Hypothesis 4; n = 12,790; 15 countries) moderate the relationship between household income and self-reported health, such that this relationship is weaker when individuals live nearer to the coast or visit it more often. We also tested whether these propositions generalize across countries (Research Question 2). The models with a random slope for both proximity/visits and income (Model 5) has the best predictive abilities (Supplementary Notes 3).
Controlling for age and sex, we find extremely strong support that individuals with a higher rather than lower household income report better general health (BF+- → ∞, b = −0.17, SE = 0.03, 90% CrI [−0.21, −0.13]). Contrary to Hypothesis 3, there is very strong evidence that the income-health relationship is stronger when living nearer to the coast (BF+- = 39.68, b = 0.01, SE = 0.00, 90% CrI [0.00, 0.01]), though this effect is very small and most likely negligible (Fig. 3a). Notably, the effect is also compatible with a null effect (i.e., the income-health relationship is similar regardless of how far individuals live from the coast), as indicated by the credible interval that includes zero. This finding generalizes across countries, as the model with a fixed interaction (i.e., identical effects across all countries) has the best predictive abilities.

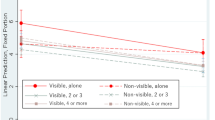
Note. a Marginal effects of household income and home coastal proximity on health. b Marginal effects of household income and coastal visits on health. Points represent the posterior mean of self-reported health from 1 ‘Very good’ to 5 ‘Very bad’ (treated as continuous for better understanding) depending on a both household income in quintiles (indicated by the five colors) and home coastal proximity as well as b both household income in quintiles (indicated by the five colors) and coastal visits. The error bars indicate the 90% credible interval, including the random effects variance across countries. The non-simplified graphs with health treated as an ordinal outcome are in Supplementary Notes 9.
Controlling for age and sex, we find insufficient evidence for Hypothesis 4 that the income-health relationship is weaker when visiting the coast more often (BF+- = 1.08, b = 0.00, SE = 0.00, 90% CrI [−0.01, 0.01]). Testing whether the effect is zero (vs. non-zero; not preregistered) reveals extremely strong evidence that lower household income is associated with poorer health regardless of how often individuals visit the coast (BF01 = 2,348.96; Fig. 3b). This finding once again generalizes across countries, as the model with a fixed interaction has the best predictive abilities.
Sensitivity analyses
We conducted several sensitivity analyses to check the robustness of all findings. The sensitivity analyses (a) with a narrower prior, α, b ~ Normal(0, 5), (b) with data from Czechia, (c) without speeders (i.e., respondents who completed the survey faster than 5 min; all Australian respondents were kept as completion time was not recorded in the Australian survey), and (d) with additional covariates (i.e., education, work status, and political orientation) yielded similar results to the main analyses, suggesting that the results are mostly robust to the choice of prior, inclusion of data from Czechia, exclusion of speeders, and inclusion of covariates (Supplementary Notes 4).
Discussion
We investigated: (a) relationships of self-reported home coastal proximity and coastal visits with self-reported general health; (b) their potential to buffer income-related health inequalities; and (c) the generalizability of these propositions across 15 countries, using a Bayesian approach.
Living nearer to the coast predicts better self-reported health within countries across Europe and Australia, with a similar yet rather small magnitude (Table 1). Importantly, 37.9% of the total improvement in health when living nearer to the coast happens between <1 km and 1–2 km, suggesting that most health benefits arise from living very close to the coast. Smaller changes (6.7–18.2%) occur between the other adjacent distance categories. These findings are consistent with Wheeler et al.3 that, for example, self-reported health is better for those living 20–50 km compared to more than 50 km from the coast. Overall, the coast provides people with a wide range of health-promoting opportunities (e.g., physical activity1,7). Living very close to the coast may make people more likely to take advantage of these opportunities6.
Visiting the coast more often also predicts better self-reported health within countries (Table 1). Notably, 53.4% of this total effect happens between visiting ‘once or twice a year’ and visiting ‘never’. This does not necessarily mean that the largest health benefits arise when visiting the coast once a year compared to never visiting it. Rather, we recognize the possibility of reverse causality here, such that individuals who never visit the coast may differ from other groups (e.g., by having a chronic illness), which limits their visit opportunities/mobility. The visits-health relationship varies across countries in terms of magnitude, with the strongest relationship in Ireland and the weakest in Italy, potentially because of high coastal tourism20 and longer travel distances in Italy (percentage of respondents who live >20 km from the coast in Ireland: 34.4% vs. Italy: 57.3%) may limit the value of the coast for locals. Moreover, the coast may be less accessible in Italy compared to other countries due to high coastal privatization21.
Supporting previous single-country studies1,2,3,4,5,6,10,11,22,23,24, the findings strengthen the evidence that living nearer to the coast and visiting it more often are associated with better self-reported health. Access to coastal environments may thus represent a viable and unified route to public health promotion across Europe and Australia.
Besides these direct effects, this study provides very and extremely strong evidence against the ‘buffering’ role of coastal contact on the income-health relationship. Lower household income is more strongly associated with poorer health when living nearer to the coast, thereby potentially reinforcing existing income-related health inequalities. However, we recognize that this effect is very small, and the results are also compatible with a null effect that the income-health relationship is similar regardless of how far individuals live from the coast.
This finding is in direct contrast to previous research that found a ‘buffering’ effect of coastal proximity for both general health, using the same outcome variable as here3, and mental health17. However, it aligns with a previous finding that more green spaces are associated with poorer health in low-income areas, potentially because green spaces in these areas are of poorer quality16. Coastal quality may also explain the current findings. When individuals with lower household incomes live near the coast, they may be more likely to live in areas of poor aesthetic and environmental quality because housing prices in such areas tend to be lower (e.g., water quality and housing prices25).
The current study also finds that lower household income is associated with poorer health regardless of coastal visits. In other words, visit frequency is positively associated with better health, irrespective of income. Although the same number of visits does not reduce health inequalities, increasing the frequency of coastal visits may still provide “leverage points for intervention”12 to improve health for people of all of incomes; and when targeting groups with lower incomes, such interventions can ultimately reduce income-related health inequalities.
Although this study contributes to understanding the value of coastal contact for health, we recognize several limitations. First, as the data are cross-sectional, we cannot rule out that healthier individuals are more likely to live near the coast and visit it more often. Nevertheless, the data are consistent with longitudinal and intervention studies that suggest that exposure to the coast is causally associated with improvements ranging from momentary moods to longer-term health effects26. Hence, the current results cannot be dismissed on selective migration grounds alone.
Second, the data are limited to middle- and high-income countries. Future research should aim to investigate whether the coastal contact-health relationships also hold for low-income countries. As individuals in low-income countries disproportionally experience threats to their health from marine environments (e.g., due to marine pollution, poor water quality, parasites, and risk of drowning27), the coast may be seen as a health risk rather than a health-protective factor.
Third, the surveys were internet-based, which appear to have, for example, under-sampled individuals with low incomes28. The findings regarding the equigenesis hypothesis should, therefore, be treated with caution, and future research should attempt to collect samples that are representative of the population in terms of household income. Relatedly, the samples were representative in terms of age, sex, and region at the national but not sub-national level. Future studies may, therefore, aim to collect larger samples that are representative at the sub-national level and assess respondents’ ethnic background, to better understand whether the current findings hold for individuals living in different regions and environments (e.g., urban vs. rural areas) as well as for individuals with different ethnic backgrounds.
Forth, the surveys were limited to rather general self-reported measures. For policy recommendations, it would be important to test the current findings’ robustness using objective health measures (e.g., hospitalizations, health service utilization). Future studies may also include (self-reported) travel time to the coast as an additional indicator of perceived coastal accessibility that may be an ecologically more valid indicator than distance per se. In addition, the self-reported visits measure may be subject to memory biases; for example, reported visit frequency in the past 12 months may be higher at the beginning of fall when thinking back to summer compared to spring when thinking back to winter. Although the number of reported visits (in the past four weeks) remains relatively frequent even in fall and winter29, future studies may aim to collect data several times a year to smooth out potential seasonality biases.
Lastly, the surveys did not monitor coastal quality. Previous research shows that higher objective and perceived quality of green spaces are associated with better self-reported general health30. As this may also apply to coastal environments, we recommend that future research considers measures of coastal quality at national and regional levels.
Conclusion
Living nearer to the coast and visiting it more often are associated with better self-reported health within countries across Europe and Australia. Although direct coastal access may represent a viable route to public health promotion, the current data suggest that the relationships of coastal living and visits with health are not strongest among individuals with low household incomes. These findings challenge widespread assumptions that access to coastal environments can reduce income-related health inequalities.
For policymakers, these results suggest that public access to coastal environments may provide clear benefits of coastal contact for public health. However, policymakers should not necessarily expect coastal access to reduce existing inequalities unless they target low-income groups in specific. Promoting and facilitating coastal contact with healthy marine environments in a fair and equitable way should be a guiding principle for policymaking as countries develop their maritime spatial plans, consider future housing needs, and develop public transportation links.
Methods
We used cross-sectional, secondary data from the Seas, Oceans, and Public Health In Europe (SOPHIE)30 and Australia (SOPHIA)31 surveys. The hypotheses and analyses of this work had been preregistered on the Open Science Framework (OSF; https://osf.io/7pju3). Deviations from the preregistration are reported in Supplementary Notes 7.
This research was performed in accordance with the declaration of Helsinki. Specifically, ethical approval for the original data collection was obtained from the Ethics Committee at the University of Exeter, Medical School (reference number: Nov18/B/171), and all participants provided informed consent at the beginning of the survey. For the current analysis, we only accessed deidentified participant data. The surveys were primarily focused on public beliefs about how marine-related issues and activities affect human health and well-being. They were translated and administered via online panels coordinated by an international polling company in 14 European countries (Belgium, Bulgaria, Czechia, France, Germany, Greece, Ireland, Italy, the Netherlands, Norway, Poland, Portugal, Spain, and the United Kingdom) from March to April 2019 and in Australia in September 2019 (spring in both settings). Samples from each country were stratified by age, sex, and region. The median survey completion time was 18.2 min.
Participants
The overall sample includes 15,179 respondents (n ≈ 1000 per country; Supplementary Notes 2) between 18 and 99 years (M = 46.20, SD = 15.81). In all, 51.3% are female, and 48.3% hold a university degree. When using 2019 country-based (rather than sample-based) income quintiles, individuals in lower income quintiles are underrepresented (lowest quintile: 14.2%; highest quintile: 21.9%; for details, see Supplementary Notes 2).
Measures
The analyses focus on selected self-reported measures, including general health as the outcome, home coastal proximity, coastal visits, and household income as the main predictors and effect modifier, as well as basic demographic information (age and sex) as potential confounders, alongside country of residence (for all measures, see Supplementary Notes 5).
Self-reported general health (outcome)
Self-reported general health was measured with the first item from the short-form health survey (SF1): “How is your health in general?” (1 ‘very good’ to 5 ‘very bad’). The SF1 has been widely used in research on nature contact1,32 as well as in the British and Irish censuses and is associated with objective health outcomes (e.g., future health service utilization33).
Self-reported coastal contact (predictor and effect modifier)
Self-reported home coastal proximity was assessed with one item: “Approximately how far do you live from the coast in miles/ km?” (1 ‘up to 1 km/0.5 miles’ to 8 ‘more than 100 km/62 miles’). Although subjective, this measure has the advantage over previous studies which used Euclidean straight-line distances from home (or neighborhood centroids) in that it allows respondents to factor in personally relevant network traveling distances. Self-reported coastal visits were assessed as follows: “Thinking now about the last 12 months in particular, which of these statements best describes how often, if ever, you visit the coast or the sea?” (1 ‘once a week or more often’ to 6 ‘never’).
Household income (predictor)
Household income was assessed in deciles adapted to each country for 2019 by the polling company (Supplementary Notes 5). For the analysis, household income was collapsed into country-level relative income (rather than sample-level) quintiles and a missing category. This approach reduced model complexity, maintained larger samples, and ensured comparability with previous research4,17.
All four main variables included additional ‘don’t know’ and ‘prefer not to answer’ options.
Potential confounders
Age (continuous), sex (male vs. female), and household income (in models where it was not an effect modifier) may be confounders. We controlled for these potential confounders if they were associated (Bayes factor of alternative against null hypothesis; BF10 ≥ 3) with any of the predictors or the outcome in the respective model.
Data analysis
Data exclusions
Respondents were excluded listwise if they had missing values on any of the key variables (but not on the confounders) in each model. The variables age and sex had no missing values, as these data were collected directly by the polling company. In addition, respondents from Czechia were excluded from the models with coastal proximity (Hypotheses 1 and 3). This resulted in analytical samples of 11,916 to 14,702 (for flow diagrams, see Supplementary Notes 6). The sampling weights, which ensure that the data are representative of the population (in terms of age, sex, and region), were rescaled to sum up to the new sample size.
Bayesian multilevel cumulative probit regressions
We used R (Version 4.1.0)34, brms (Version 2.16.3)35, and RStan (Version 2.21.3)36 to fit Bayesian multilevel cumulative probit regressions, with respondents at level 1 and countries at level 2. Unlike frequentist approaches, Bayesian analyses allow for conclusions about the relative support for or against any relationships, provide rich information about the strength of evidence, and are valid for large samples18.
Home coastal proximity and coastal visits were modeled as categorical (reference category: <1 km and ‘once a week or more often’) and monotonic (i.e., change in health between consecutive categories of proximity/visits is consistently non-increasing or non-decreasing37) to account for the unequal distance between categories.
To test Hypotheses 1 and 2, we deviated from the preregistration (for rationale, see Supplementary Notes 7) due to multi-collinearity between proximity and visits (Kendall’s τb = 0.60) and fitted four models per hypothesis, each with a random intercept: Model 1 with proximity/visits as a categorical predictor, Model 2 with additional random slopes for categorical proximity/visits (i.e., proximity/visits-health relationship is allowed to vary across countries), Model 3 with proximity/visits as a monotonic predictor, and Model 4 with additional random slopes for monotonic proximity/visits.
To test Hypotheses 3 and 4, we used the best-performing model and included the fixed interaction between household income and proximity/visits (Model 1 and 4), then the random slope for income (Model 2 and 5), and last the random interaction (Model 3 and 6).
Conclusions regarding the hypotheses were based on the model with the best predictive abilities (i.e., lower leave-one-out cross-validation information criterion; LOOIC), the Bayes Factor (BF; Supplementary Notes 8), and the posterior distribution.
The BF of alternative against null hypothesis (BF10) and the BF of null against alternative hypothesis (BF01) indicate that two hypotheses were tested (two-sided) against each other: the alternative hypothesis that the relationship differs from zero and the null hypothesis that the relationship is effectively zero. For example, BF10 = 10 would indicate that the data are 10 times more likely under the alternative compared to the null hypothesis; BF01 = 10 would indicate the opposite. In contrast, BF+- and BF-+ indicate that the hypotheses were tested one-sided: the relationship is positive (H+) versus the relationship is negative (H−). BF+- = 10 would, therefore, mean that the data are 10 times more likely under the hypothesis that the relationship is positive rather than negative, whereas BF-+ = 10 would, once again, indicate the opposite.
Conclusions regarding generalizability across countries were based on the overlap of the credible intervals (CrIs).
Priors were weakly informative, including α, b ~ Normal(0, 10) for the intercepts α and slope coefficients b, σcountry ~ HalfCauchy(0, 10) for the variation around the intercept per country, and a uniform Dirichlet distribution on the simplex parameters ξ (difference between consecutive categories; only for monotonic models). Models were fitted with four independent Markov chain Monte Carlo chains and 4000 iterations, of which 1000 per chain served as a warm-up. The chains converged and were well-mixed, effective sample sizes indicated stable estimates, no divergent transitions occurred, and posterior predictive checks indicated that the models fit the data.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
The deidentified participant data from Europe (SOPHIE) and the corresponding codebook are available after registration via the UK Data Service (https://doi.org/10.5255/UKDA-SN-8972-1; https://beta.ukdataservice.ac.uk/datacatalogue/studies/study?id=8972). The cleaned datasets (SOPHIE and SOPHIA) for the analyses in this article are available as csv files on the OSF (https://osf.io/u6scg).
Code availability
The R code to conduct the analyses is publicly available on the OSF (https://osf.io/u6scg). Other additional documents are available on the OSF as well, including the preregistration, the statistical analysis plan, and an overview of all measures in the surveys. We followed the STROBE checklist for reporting cross-sectional studies (https://www.strobe-statement.org/checklists/). We have preregistered Hypotheses 1 and 2, Research Question 1, and the data analyses on the OSF (https://osf.io/7pju3, December 13, 2021). After accessing the data (December 16, 2021) and inspecting the income-health correlation, we added an addendum for Hypotheses 3 and 4, Research Question 2, and the respective analyses (March 07, 2022).
References
Pasanen, T. P., White, M. P., Wheeler, B. W., Garrett, J. K. & Elliott, L. R. Neighbourhood blue space, health and wellbeing: The mediating role of different types of physical activity. Environ. Int. 131, 105016 (2019).
Wheeler, B. W. et al. Beyond greenspace: an ecological study of population general health and indicators of natural environment type and quality. Int. J. Health Geogr. 14, 1–17 (2015).
Wheeler, B. W., White, M., Stahl-Timmins, W. & Depledge, M. H. Does living by the coast improve health and wellbeing? Health Place 18, 1198–1201 (2012).
Hooyberg, A. et al. General health and residential proximity to the coast in Belgium: Results from a cross-sectional health survey. Environ. Res. 184, 109225 (2020).
Ballesteros-Olza, M., Gracia-de-Rentería, P. & Pérez-Zabaleta, A. Effects on general health associated with beach proximity in Barcelona (Spain). Health Promot. Int 35, 1406–1414 (2020).
White, M. P., Alcock, I., Wheeler, B. W. & Depledge, M. H. Coastal proximity, health and well-being: results from a longitudinal panel survey. Health Place 23, 97–103 (2013).
Gascon, M., Zijlema, W., Vert, C., White, M. P. & Nieuwenhuijsen, M. J. Outdoor blue spaces, human health and well-being: A systematic review of quantitative studies. Int. J. Hyg. Environ. Health 220, 1207–1221 (2017).
Nutsford, D., Pearson, A. L., Kingham, S. & Reitsma, F. Residential exposure to visible blue space (but not green space) associated with lower psychological distress in a capital city. Health Place 39, 70–78 (2016).
Elliott, L. R. et al. Residential distance and recreational visits to coastal and inland blue spaces in eighteen countries. Landsc. Urban Plan. 198, 103800 (2020).
Elliott, L. R., White, M. P., Taylor, A. H. & Herbert, S. Energy expenditure on recreational visits to different natural environments. Soc. Sci. Med. 139, 53–60 (2015).
Korpela, K., Ylén, M., Tyrväinen, L. & Silvennoinen, H. Favorite green, waterside and urban environments, restorative experiences and perceived health in Finland. Health Promot. Int. 25, 200–209 (2010).
Wells, N. The natural environment as a resilience factor: Nature’s role as a buffer of the effects of risk and adversity. In Nature and Psychology vol. 67 195–233 (2021) (Springer, Cham).
Mitchell, R. & Popham, F. Effect of exposure to natural environment on health inequalities: An observational population study. Lancet 372, 1655–1660 (2008).
Meyer, O. L., Castro-Schilo, L. & Aguilar-Gaxiola, S. Determinants of mental health and self-rated health: a model of socioeconomic status, neighborhood safety, and physical activity. Am. J. Public Health 104, 1734–1741 (2014).
Rigolon, A., Browning, M. H. E. M., McAnirlin, O. & Yoon, H. V. Green space and health equity: A systematic review on the potential of green space to reduce health disparities. Int. J. Environ. Res. Public. Health 18, 2563 (2021).
Mitchell, R. & Popham, F. Greenspace, urbanity and health: Relationships in England. J. Epidemiol. Community Health 61, 681–683 (2007).
Garrett, J. K., Clitherow, T. J., White, M. P., Wheeler, B. W. & Fleming, L. E. Coastal proximity and mental health among urban adults in England: The moderating effect of household income. Health Place 59, 102200 (2019).
Wagenmakers, E.-J. et al. Bayesian inference for psychology. Part I: Theoretical advantages and practical ramifications. Psychon. Bull. Rev. 25, 35–57 (2018).
Lindley, D. V. Bayesian Statistics. (Society for Industrial and Applied Mathematics, 1972). https://doi.org/10.1137/1.9781611970654.
European Commission et al. The EU Blue Economy Report. https://data.europa.eu/doi/10.2771/793264 (2022).
Legambiente. Rapporto Spiagge 2022. 1–74 https://www.legambiente.it/rapporti-e-osservatori/rapporto-spiagge/ (2022).
Ashbullby, K. J., Pahl, S., Webley, P. & White, M. P. The beach as a setting for families’ health promotion: A qualitative study with parents and children living in coastal regions in Southwest England. Health Place 23, 138–147 (2013).
White, M. P., Wheeler, B. W., Herbert, S., Alcock, I. & Depledge, M. H. Coastal proximity and physical activity: Is the coast an under-appreciated public health resource? Prev. Med. 69, 135–140 (2014).
White, M. P., Pahl, S., Ashbullby, K., Herbert, S. & Depledge, M. H. Feelings of restoration from recent nature visits. J. Environ. Psychol. 35, 40–51 (2013).
Liu, T., Opaluch, J. J. & Uchida, E. The impact of water quality in Narragansett Bay on housing prices. Water Resour. Res. 53, 6454–6471 (2017).
White, M. P., Elliott, L. R., Gascon, M., Roberts, B. & Fleming, L. E. Blue space, health and well-being: A narrative overview and synthesis of potential benefits. Environ. Res. 191, 110169 (2020).
World Health Organization. Global report on drowning: Preventing a leading killer. https://apps.who.int/iris/handle/10665/327621 (2014).
Rookey, B. D., Hanway, S. & Dillman, D. A. Does a probability-based household panel benefit from assignment to postal response as an alternative to internet-only? Public Opin. Q. 72, 962–984 (2008).
White, M. P. et al. Associations between green/blue spaces and mental health across 18 countries. Sci. Rep. 11, 8903 (2021).
McMeel, O. et al. Seas, oceans and public health in Europe (SOPHIE; https://doi.org/10.5255/UKDA-SN-8972-1). (2019).
McMeel, O. et al. Seas, oceans and public health in Australia (SOPHIA; https://osf.io/u6scg/). (2019).
Martin, L. et al. Nature contact, nature connectedness and associations with health, wellbeing and pro-environmental behaviours. J. Environ. Psychol. 68, 101389 (2020).
Doiron, D., Fiebig, D. G., Johar, M. & Suziedelyte, A. Does self-assessed health measure health? Appl. Econ. 47, 180–194 (2015).
R Core Team. R: A language and environment for statistical computing. (2021).
Bürkner, P.-C. Advanced Bayesian multilevel modeling with the R package brms. R J 10, 395–411 (2018).
Stan Development Team. RStan: The R interface to Stan. (2022).
Bürkner, P.-C. & Charpentier, E. Modeling monotonic effects of ordinal predictors in Bayesian regression models. Br. J. Math. Stat. Psychol. 73, 420–451 (2018).
Acknowledgements
This research was funded by the European Union’s Horizon 2020 research and innovation program (grant agreement no. 774567) and a Queensland University/Exeter University (QUEX) Initiator Grant Scheme. Open Access funding was provided by the University of Vienna.
Author information
Authors and Affiliations
Contributions
Sandra J. Geiger: Conceptualization, Data curation, Data access and validation, Formal analysis, Project administration, Software, Visualization, Writing—original draft, Writing—review & editing. Mathew P. White: Conceptualization, Data access and validation, Funding acquisition, Methodology, Supervision, Writing—review & editing. Sophie M. C. Davison: Funding acquisition, Investigation, Methodology. Lei Zhang: Validation (analysis), Writing—review & editing. Oonagh McMeel: Funding acquisition, Investigation, Methodology, Writing—review & editing. Paula Kellett: Funding acquisition, Investigation, Writing—review & editing. Lora E. Fleming: Funding acquisition, Methodology, Writing—review & editing.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Peer review
Peer review information
Communications Earth & Environment thanks Ai Tashiro, Alexander Hooyberg and the other, anonymous, reviewer(s) for their contribution to the peer review of this work. Primary Handling Editors: Sagar Parajuli, Joe Aslin and Heike Langenberg. A peer review file is available.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Geiger, S.J., White, M.P., Davison, S.M.C. et al. Coastal proximity and visits are associated with better health but may not buffer health inequalities. Commun Earth Environ 4, 166 (2023). https://doi.org/10.1038/s43247-023-00818-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s43247-023-00818-1
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
