





Abstract
Aims Anaemia is often observed in patients with chronic heart failure (CHF), and it may be associated with a worse prognosis. Aim of this study was to identify the individual mechanisms of anaemia in CHF patients.
Methods and results One hundred and forty-eight consecutive patients with haemoglobin concentration <13 g/dL (if males) or <12 g/dL (if females) were enrolled. Factors responsible for anaemia were investigated by evaluating endogenous erythropoietin (Epo) production, serum cytokines levels, body iron status, and iron supply for erythropoiesis. Most patients (57%) presented anaemia of chronic disease and among them, 92% showed evidence of a defective endogenous Epo production. This was indicated by an observed/predicted log(serum Epo) ratio less than 0.8 and/or a defective iron supply for erythropoiesis diagnosed by low transferrin saturation and/or increased value of soluble transferrin receptor. According to regression analysis sex, renal failure, and serum Epo were correlated with anaemia.
Conclusion According to our study, about half of anaemic CHF patients showed anaemia of chronic disease with blunted endogenous Epo production and/or a defective iron supply for erythropoiesis. Determination of the individual mechanisms of anaemia in CHF could justify a rational therapeutic approach to anaemia.
See for the editorial comment on this article (doi:10.1093/eurheartj/ehi509)
Introduction
Chronic heart failure (CHF) is a complex syndrome related to both dysfunctional regulatory systems and a heart performance that is inadequate to meet the tissues' demands.1 Adequate tissue oxygen supply depends not only on cardiac output but also on arterial blood haemoglobin (Hb) concentration and oxygen saturation.2 Each of these components has its own mechanisms to compensate for hypoxia. Sustained reductions in the tissue oxygen pressure (PO2) stimulate both red cell production, by means of erythropoietin, (Epo) and 2,3-diphosphoglycerate production to shift the Hb oxygen-dissociation curve for greater oxygen delivery.3 Anaemia may significantly affect oxygen delivery. In the last few years, several studies have shown that anaemia is frequent in patients with CHF,4 has a prognostic power,5–13 and is a target of therapy.14–17 However, the heterogeneity of both aetiology and progression processes of the heart failure syndrome suggests that the anaemia's pathophysiology might be non-univocal in the universe of heart failure patients.18–20
In this study, we focus on some of the mechanisms of impaired red cell production in consecutive anaemic CHF patients.
Methods
Study design and patients
All patients evaluated in this study suffered from CHF due to either left ventricular systolic or diastolic dysfunction and were regularly attending heart failure clinics. The diagnostic criteria for CHF were those recommended by the European Society of Cardiology guidelines.21 Patients were included in the study only if they were in stable clinical conditions (absence of physical findings of congestion, significant changes in diuretics, and weight or blood pressure in the previous four weeks) and only if they presented at least once in the last 3 months an Hb concentration value <13 g/dL if males and <12 g/dL if females. Patients were not considered eligible for the study if they had any comorbid condition causing anaemia (i.e. malignancies, chronic inflammatory states, collagen vascular diseases, myelodysplastic or myelophthisic syndromes, immunosuppressant therapy, and chemo/radiation therapy). New cases of heart failure defined by a duration of symptoms <6 months were also excluded.
The patients were enrolled from January to October 2002 in three heart failure clinics.
In all patients, blood samples were collected to determine complete blood cell count, body iron status, iron supply for erythropoiesis, endogenous Epo production, and cytokines levels.
The procedures we followed were in accordance with the ethical standards of the institutional committee on human experimentation and with the Helsinki Declaration of 1975, as revised in 1983.
After overnight fasting, an intravenous cannula was inserted. After at least a 20 min supine rest, blood samples were withdrawn. An assay to determine blood cell count, body iron status, and iron supply for erythropoiesis was performed using the hospital's routine analysis procedures. Serum samples for cytokines, cytokines receptor, and Epo levels were stored at −80° until analysis.
Haematological profile and iron status
Blood counts were determined with automatic counters. Body iron status was evaluated by measuring serum iron, serum ferritin, and soluble transferrin receptor (Dade Behring, Marburg, Germany). Creatinine clearance was estimated by the Cockcroft–Gault formula.22
Serum Epo assay
Circulating Epo levels were measured by partly automated two-step enzyme immunoassay on the basis of two monoclonal antibodies used to recognize natural or recombinant Epo (EPO ELISA—Medac, Hamburg, Germany). The standard curve of the assay is linear up to 80 mIU/mL and it is substandardized against the Third International Standard for Epo. To define Epo levels as appropriate or inappropriate for a given degree of anaemia, an exponential regression of serum Epo vs. Hb was determined in 31 reference subjects (Epo 14.1±2.8 mU/mL) and 95% confidence limits were defined.23 For Hb values <13 g/dL, the regression equation was log(Epo)=4.746−(0.275×Hb). This equation was employed to predict Epo on the basis of Hb concentration and to derive the observed/predicted log(Epo) ratio (O/P ratio) as following: O/P ratio=[log(observed Epo)]/[log(predicted Epo)]. Mean O/P ratio in reference subjects was 1.01±0.11 (95% CI 0.80–1.22).24–26 A defective endogenous Epo production was defined as an O/P ratio less than 0.8.
C-reactive protein assay
C-reactive protein was measured by high-sensitive C-reactive protein assay (Dade Behring) by means of particle-enhanced immunonephelometry using BNTM System, designed to measure C-reactive protein concentrations in the overall range of 0.0175–110 mg/dL. Our reference interval was up to 0.5 mg/dL.27
Serum cytokines assay
Tumour necrosis factor-alpha (TNF-α) and its two soluble receptors, sTNFR-I and sTNRF-II, and interleukin-6 (IL-6) and interleukin-1 receptor (IL-1Ra) levels were measured using ELISA commercial kits (TNF-α: Biosource, Europe SA Nivelles, Belgium; sTNFR-I and sTNFR-II, IL-6 and IL-1Ra: R&D System Inc., Minneapolis, MN, USA) as previously described.28
The sensitivity of the kits used for measurements of TNF-α, sTNFR-I and sTNFR-II, and IL-6 and IL-1Ra was <0.5 pg/mL, 3 pg/mL, 1 pg/mL, 0.7 pg/mL, and 1 pg/mL, respectively. All kits had a good linearity in the detected intervals. Coefficients of variation were 3.9, 5.5, 3.8, 3.5, and 4.4%, respectively.
For cytokines levels, the reference subjects were 24 healthy males and 16 females, mean age 65±6 years.28
Statistical analysis
The association between clinical and haematological variables was assessed by Pearson's coefficient of correlation or by analysis of variance depending on whether the variables were continuous or categorical, respectively. All tests were two-sided. No formal sample size calculations were done. Data are reported as mean value ±1 SD. All tests of hypothesis were carried out using 0.05 as the level of statistical significance.
Results
One hundred and forty-eight patients were included in the study. Their clinical characteristics are reported in Table 1. The majority of patients were males, affected by a dilated ischaemic cardiomyopathy with prevalent systolic dysfunction, in New York Heart Association (NYHA) class II and III. Heart failure symptoms were longlasting and renal dysfunction (defined as plasma creatinine >1.5 mg/dL, range 1.53–3.9 mg/dL) was found in 30% of the patients. Nearly all patients were receiving diuretics, ACE-inhibitors or ATII-inhibitors, antiplatelet drugs or warfarin; 55% of them were on beta-blockers.
Haematological data and parameters of body iron status are reported in Table 2. Distribution of the anaemia causing factors in our population is reported in Figure 1.
Although the major criterion of inclusion was an Hb concentration <13 g/dL(if males) or <12 g/dL (if females) on at least one occasion, at the time of enrolment three males and two females showed borderline Hb values (Hb 13.1, 13.2, and 13.5 g/dL and Hb 12.0 and 12.4 g/dL, respectively).
Thirty-one patients had microcytic anaemia, defined as mean corpuscular volume (MCV) value <80 fL. Eight of them had heterozygous beta-thalassaemia: a 5% frequency is comparable to that of thalassaemia carriers in the Italian population. Only two patients had microcytic iron deficiency anaemia (ferritin <15 ng/mL in males and <10 ng/mL in females).
Seven patients had macrocytic anaemia (MCV>100 fL) associated with folate deficiency. One hundred and five patients were found to have normocytic anaemia. Six of them had iron deficiency according to their low ferritin values. In thirty-five cases, there was evidence of renal impairment (serum creatinine >1.5 mg/dL) indicating renal anaemia, with mean serum Epo 18.2±24.8 mU/mL; 80% of them showed a defective endogenous Epo production (indicated by O/P ratio less than 0.8). No patient displayed signs of haemolytic anaemia.
Anaemia of chronic disease
Out of the entire study population, eighty-five patients had anaemia of chronic disease, as defined by the following parameters: reduced concentrations of serum iron, transferrin, and total iron binding capacity; normal or raised ferritin; normal or slightly increased soluble transferrin receptor. All patients had normal ferritin values; 50 of them had low serum iron (<60 µg/dL), 36 had low transferrin saturation (<15%), and 47 had increased levels of soluble transferrin receptor (>1.76 g/L). Overall, the combination of high soluble transferrin receptor and/or low transferrin saturation, indicating iron deficiency for erythropoiesis, was found in 54 patients. Two persons had fasting iron saturation >60%, suggesting iron overload. A C-reactive protein level >0.50 mg/dL was found in 53 patients (62%), urea was >50 mg/dL in 60 patients (71%), and all but 14 individuals showed elevated (higher than mean+2SD of the reference values) TNF-α levels (Table 3). In these patients with chronic disease anaemia, serum Epo levels correlated with cardiac disease severity (NYHA class II 8.4±7.6 mU/mL; NYHA class III 29±37 mU/mL; NYHA class IV 53.4±74 mU/mL; F=6.7; P=0.001), with C-reactive protein (r=−0.25; P=0.021) and, strongly, with IL-6 (r=0.57; P=0.0001). According to the calculated O/P ratio, the vast majority of anaemic patients showed evidence of defective endogenous Epo production. In fact, using a cut-off value of 0.8 for the O/P ratio, 76% (65/85) of the investigated patients had a ratio below this value.
Out of the group classified as having anaemia of chronic disease, 78 patients (92%) showed iron deficiency for erythropoiesis (that is high soluble transferrin receptor and/or low transferrin saturation) and/or defective endogenous Epo production.
In these patients, Hb significantly correlated with gender (females 10.4±0.9 g/dL vs. males 11.1±1.0 g/dL; P=0.0002) and inversely related with serum creatinine (r=−0.42; P<0.001), urea (r=−0.29; P=0.008), sTNFR-I (r=−0.44; P<0.001), IL-6 (r=−0.41; P=0.001), and Epo levels (r=−0.21; P=0.04).
Discussion
Multiple factors contribute to anaemia in our CHF population (Figure 1). A reduced Hb concentration may be a consequence of the haemodilution, which is often due to the activation of rennin–angiotensin–aldosterone and vasopressin systems, leading to sodium and water retention. Pseudo-anaemia due to plasma volume seems to have a worse prognosis than ‘true’ anaemia.29 In our study, the volume status was assessed only by physical examination, whereas haemodilution may occur even in some patients appearing as being euvolemic on clinical examination. All the patients we selected were in stable conditions and had at least two Hb determinations spaced of minimum 10 days (mean 49 days) from each others to limit the likelihood of a significant haemodilution.
Only few patients showed haematinic deficiencies (iron, folate, and/or vitamin B12), which are also reported as being a rare event in other series of CHF patients,18,30 likely due to poor nutrition, gastrointestinal malabsorption, chronic use of aspirin, uremic gastritis, and other comorbidity.
Among the potential causes of normocytic anaemia, which affected 71% of our patients, renal dysfunction with consequent decreased renal Epo secretion was found in a third of our cases.18,31
Poor utilization of seemingly adequate iron stones, excessive cytokines activation, and inhibited synthesis of Epo were common, suggesting that these are probably the most important factors closely connected with anaemia of chronic disease. They were found in 57% of our population, a proportion similar to the one that is reported in the literature.9 In the vast majority of these patients, we found evidence of inadequate endogenous Epo production and/or defective iron supply for erythropoiesis. These observations may have clinical implications, as in most instances, intravenous iron, combined, in selected cases, with subcutaneous administration of recombinant human Epo would represent a rational therapeutic approach to these anaemic CHF patients.14–17,32
A variety of causes were identified for defective endogenous Epo production. Epo is mostly produced by the kidney and hypoxia is the fundamental physiologic stimulus to the Epo renal production through an exponential increase in the number of Epo producing cells.32 Defective Epo production is the major cause of anaemia associated with renal failure and likely of anaemia in CHF patients with concomitant renal damage.
Inflammatory cytokines may interfere with Epo gene expression.25,33 Interleukins, TNF-α, and transforming growth factor-beta have been found to inhibit hypoxia-induced Epo production in vitro. At variance, IL-6 was shown to mimic hypoxia in vitro, and elevated levels in humans are associated with increase endogenous Epo production.25 By inhibiting erythroid progenitor cell proliferation, these cytokines also play a major role in the pathogenesis of anaemia of chronic disease, which was established as a distinct entity in 1962 and which is frequently associated with diabetes mellitus, connective tissue disease, chronic infections, and malignancy.34 Anaemia of chronic disease is often normochromic normocytic, even if it may also show hypochromic microcytic indices similar to the effects of iron deficiency. It is characterized by reduced concentrations of serum iron, transferrin, and total iron binding capacity; normal or raised ferritin (instead of reduced as when iron sores are diminished); normal or slightly increased soluble transferrin receptor (which are raised in iron deficiency anaemia); and high erythrocyte sedimentation rate.34 Moreover, elevated plasma levels of inflammatory cytokines, particularly TNF-α, are implicated in the Epo resistance process and have been shown to interfere with the peripheral actions of Epo.19 Epo resistance could also be relevant to anaemia in CHF and could explain why elevated plasma Epo levels were associated with an impaired prognosis in van der Meer's study on 74 CHF patients.35 In our study, IL-6 resulted strictly related with Epo endogenous production. In fact, nearly all the anaemic patients we studied showed evidence of cytokines activation, and it is very likely that this factor also contributed to the development of blunted endogenous Epo production.
Inflammatory cytokines not only interfere with Epo gene expression, but also have a major impact on iron metabolism, determining the so-called reticuloendothelial iron block with defective iron supply to the erythropoiesis. The molecular mechanisms responsible for this effect have been recently elucidated.36 Hepcidin is the key regulator for iron metabolism and mediator of anaemia during inflammation. This small peptide is induced by inflammatory cytokines and its overproduction results in macrophage iron retention and, consequently, less iron is available for erythropoiesis. This reticuloendothelial iron block cannot be overcome by oral iron administration, whereas intravenous iron may be effective for this purpose.37 The best parameters to recognize impaired iron supply to the erythroid marrow are transferrin saturation and soluble transferrin receptor.38 In an anaemic patient with CHF, a transferrin saturation <15% and an increased level of soluble transferrin receptor are together suggestive of iron deficient erythropoiesis.
Finally, several drugs may interfere with Epo gene expression. Angiotensin-converting enzyme-inhibitors may cause a reduction in the Hb levels by attenuating the production of Epo and may therefore contribute to anaemia in CHF patients.39 The signal seems to be mediated via AT1 receptors and a possible advantage of AT1 antagonists over ACE-inhibitors with regard to EPO effect has not been elucidated yet.40
Limits of the study
Patients here investigated had moderate heart failure; however, it cannot be ruled out, though it is unlikely, that in more symptomatic patients with a more severe systolic dysfunction, mechanism of anaemia might be somehow different.
Moreover, undernourishment was not routinely searched in our patients; however, only few of them showed haematinic deficiencies.
In the present study, chronic bleedings were not specifically investigated in our out-patients, which did not present clinical indicators of historical or present haemorrhages, although many of them were on antiplatelet drugs or warfarin. However, in our series, severe liver dysfunction, bleeding diathesis, and coagulopathy were considered as exclusion criteria.
Our study was multicentred and focused on anaemic patients. Unfortunately, a log book of all patients among whom the anaemics were found has not been held and the real prevalence of anaemic patients is not available. Anyway, we reviewed the number of patients visited at the heart failure clinics during the period of pertinent enrolment in the study and obtained a prevalence of 15.6%, similar to that reported in the literature.4,5–13
Finally, no healthy control subjects were included in the study. It was considered that being data on normal people largely available, the fact of asking subjects to provide their blood samples just to serve as controls might appear as non-ethical.
Practical implications
According to the present study, it appears that many anaemic patients with CHF have chronic disease anaemia with both blunted endogenous Epo production and iron deficient erythropoiesis.
An observed/predicted log Epo ratio less than 0.80 in an anaemic patient could be taken as a reliable indicator of blunted Epo production.41 These patients are very likely to respond to renal doses of recombinant human Epo with an amelioration of anaemia, even when renal function is still normal.
Acknowledgements
We are grateful to Dr Gloria Francolini (Laboratory of Chemical Analysis, Fondazione S. Maugeri, Gussago) and Dr Giulia Albonico (Laboratory of Chemical Analysis of the IRCCS Policlinico S. Matteo) for the technical support.
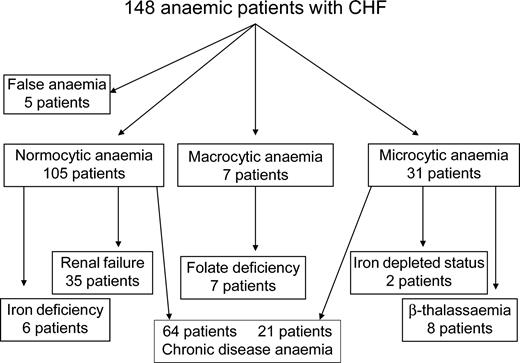
Figure 1 Causes of anaemia in our population of CHF patients.
Baseline characteristics of the study population
| Characteristics | Patients |
|---|---|
| Age, years | 64.5±12.2 |
| Males, n (%) | 109 (74) |
| NYHA class II/III/IV, n (%) | 58/69/21 (39, 47, 14) |
| CHF symptoms duration (months) | 33.9±36 |
| Diabetes, n (%) | 43 (29) |
| Smokers (past or present), n (%) | 49 (33) |
| Patients with ≥1 comorbidity, n (%) | 104 (70) |
| Serum creatinine (mg/dL) | 1.47±0.6 |
| Aetiology, n (%) | |
| Ischaemic cardiopathy | 71 (48) |
| Hypertensive cardiopathy | 7 (5) |
| Dilated cardiomyopathy | 45 (30) |
| Valvular cardiopathy | 14 (10) |
| Others | 7 (5) |
| Not known | 4 (2) |
| Echocardiographic data | |
| Left ventricular end-diastolic diameter (mm) | 62.4±10.7 |
| Left ventricular end-diastolic volume (mL) | 185.7±85 |
| Left ventricular ejection fraction (%) | 31±12.1 |
| Therapy | |
| Digoxin, n (%) | 60 (40) |
| ACE-inhibitors/ATII-inhibitors, n (%) | 133 (90) |
| Captopril equivalent dose (mg) | 67.3±26.5 |
| Beta-blockers, n (%) | 82 (55) |
| Furosemide, n (%) | 141 (95) |
| Other diuretics, n (%) | 15 (10) |
| Nitrates, n (%) | 67 (45) |
| Antiplatelet agents, n (%) | 55 (37) |
| Warfarin, n (%) | 83 (56) |
| Characteristics | Patients |
|---|---|
| Age, years | 64.5±12.2 |
| Males, n (%) | 109 (74) |
| NYHA class II/III/IV, n (%) | 58/69/21 (39, 47, 14) |
| CHF symptoms duration (months) | 33.9±36 |
| Diabetes, n (%) | 43 (29) |
| Smokers (past or present), n (%) | 49 (33) |
| Patients with ≥1 comorbidity, n (%) | 104 (70) |
| Serum creatinine (mg/dL) | 1.47±0.6 |
| Aetiology, n (%) | |
| Ischaemic cardiopathy | 71 (48) |
| Hypertensive cardiopathy | 7 (5) |
| Dilated cardiomyopathy | 45 (30) |
| Valvular cardiopathy | 14 (10) |
| Others | 7 (5) |
| Not known | 4 (2) |
| Echocardiographic data | |
| Left ventricular end-diastolic diameter (mm) | 62.4±10.7 |
| Left ventricular end-diastolic volume (mL) | 185.7±85 |
| Left ventricular ejection fraction (%) | 31±12.1 |
| Therapy | |
| Digoxin, n (%) | 60 (40) |
| ACE-inhibitors/ATII-inhibitors, n (%) | 133 (90) |
| Captopril equivalent dose (mg) | 67.3±26.5 |
| Beta-blockers, n (%) | 82 (55) |
| Furosemide, n (%) | 141 (95) |
| Other diuretics, n (%) | 15 (10) |
| Nitrates, n (%) | 67 (45) |
| Antiplatelet agents, n (%) | 55 (37) |
| Warfarin, n (%) | 83 (56) |
Baseline characteristics of the study population
| Characteristics | Patients |
|---|---|
| Age, years | 64.5±12.2 |
| Males, n (%) | 109 (74) |
| NYHA class II/III/IV, n (%) | 58/69/21 (39, 47, 14) |
| CHF symptoms duration (months) | 33.9±36 |
| Diabetes, n (%) | 43 (29) |
| Smokers (past or present), n (%) | 49 (33) |
| Patients with ≥1 comorbidity, n (%) | 104 (70) |
| Serum creatinine (mg/dL) | 1.47±0.6 |
| Aetiology, n (%) | |
| Ischaemic cardiopathy | 71 (48) |
| Hypertensive cardiopathy | 7 (5) |
| Dilated cardiomyopathy | 45 (30) |
| Valvular cardiopathy | 14 (10) |
| Others | 7 (5) |
| Not known | 4 (2) |
| Echocardiographic data | |
| Left ventricular end-diastolic diameter (mm) | 62.4±10.7 |
| Left ventricular end-diastolic volume (mL) | 185.7±85 |
| Left ventricular ejection fraction (%) | 31±12.1 |
| Therapy | |
| Digoxin, n (%) | 60 (40) |
| ACE-inhibitors/ATII-inhibitors, n (%) | 133 (90) |
| Captopril equivalent dose (mg) | 67.3±26.5 |
| Beta-blockers, n (%) | 82 (55) |
| Furosemide, n (%) | 141 (95) |
| Other diuretics, n (%) | 15 (10) |
| Nitrates, n (%) | 67 (45) |
| Antiplatelet agents, n (%) | 55 (37) |
| Warfarin, n (%) | 83 (56) |
| Characteristics | Patients |
|---|---|
| Age, years | 64.5±12.2 |
| Males, n (%) | 109 (74) |
| NYHA class II/III/IV, n (%) | 58/69/21 (39, 47, 14) |
| CHF symptoms duration (months) | 33.9±36 |
| Diabetes, n (%) | 43 (29) |
| Smokers (past or present), n (%) | 49 (33) |
| Patients with ≥1 comorbidity, n (%) | 104 (70) |
| Serum creatinine (mg/dL) | 1.47±0.6 |
| Aetiology, n (%) | |
| Ischaemic cardiopathy | 71 (48) |
| Hypertensive cardiopathy | 7 (5) |
| Dilated cardiomyopathy | 45 (30) |
| Valvular cardiopathy | 14 (10) |
| Others | 7 (5) |
| Not known | 4 (2) |
| Echocardiographic data | |
| Left ventricular end-diastolic diameter (mm) | 62.4±10.7 |
| Left ventricular end-diastolic volume (mL) | 185.7±85 |
| Left ventricular ejection fraction (%) | 31±12.1 |
| Therapy | |
| Digoxin, n (%) | 60 (40) |
| ACE-inhibitors/ATII-inhibitors, n (%) | 133 (90) |
| Captopril equivalent dose (mg) | 67.3±26.5 |
| Beta-blockers, n (%) | 82 (55) |
| Furosemide, n (%) | 141 (95) |
| Other diuretics, n (%) | 15 (10) |
| Nitrates, n (%) | 67 (45) |
| Antiplatelet agents, n (%) | 55 (37) |
| Warfarin, n (%) | 83 (56) |
Haematological parameters of the study population
| Parameter | Males (n=109) | Females (n=39) | Reference values |
|---|---|---|---|
| Hb (g/dL) | 11.1±1.04 | 10.5±0.98 | Males: 13–17 |
| Females: 12–16 | |||
| MCV (fL) | 86.2±9.8 | 84.5±10.4 | 83–97 |
| Reticulocytes (109/L) | 12.8±17.2 | 22±24.4 | 20–100 |
| Platelets (109/L) | 232±86.7 | 256±70 | 150–450 |
| Serum iron (µg/dL) | 64.3±31 | 57.6±28 | 60–150 |
| Transferrin saturation (%) | 22.4±13 | 16.8±9.4 | 15–45 |
| Serum ferritin (ng/mL) | 182±193 | 102±132 | Males: 15–250 |
| Females 10–150 | |||
| Soluble transferrin receptor (mg/L) | 2.2±0.3 | 2.5±1.58 | 0.83–1.76 |
| Serum erythropoietin (mU/mL) | 19.9±33 | 25.5±36.4 | 5–25 in non-anaemic subjects26 |
| EPO O/P ratio | 0.64±0.4 | 0.49±0.3 | 0.80–1.2026 |
| Serum urea (mg/dL) | 76.1±36 | 82.7±48 | 10–50 |
| Creatinine clearance (mL/min) | 74±16 | 73.8±14 | 90–150 |
| Serum creatinine (mg/dL) | 1.5±0.57 | 1.4±0.6 | 0.7–1.20 |
| C-reactive protein (mg/dL) | 1.6±2.5 | 1.5±2.1 | <0.50 |
| Parameter | Males (n=109) | Females (n=39) | Reference values |
|---|---|---|---|
| Hb (g/dL) | 11.1±1.04 | 10.5±0.98 | Males: 13–17 |
| Females: 12–16 | |||
| MCV (fL) | 86.2±9.8 | 84.5±10.4 | 83–97 |
| Reticulocytes (109/L) | 12.8±17.2 | 22±24.4 | 20–100 |
| Platelets (109/L) | 232±86.7 | 256±70 | 150–450 |
| Serum iron (µg/dL) | 64.3±31 | 57.6±28 | 60–150 |
| Transferrin saturation (%) | 22.4±13 | 16.8±9.4 | 15–45 |
| Serum ferritin (ng/mL) | 182±193 | 102±132 | Males: 15–250 |
| Females 10–150 | |||
| Soluble transferrin receptor (mg/L) | 2.2±0.3 | 2.5±1.58 | 0.83–1.76 |
| Serum erythropoietin (mU/mL) | 19.9±33 | 25.5±36.4 | 5–25 in non-anaemic subjects26 |
| EPO O/P ratio | 0.64±0.4 | 0.49±0.3 | 0.80–1.2026 |
| Serum urea (mg/dL) | 76.1±36 | 82.7±48 | 10–50 |
| Creatinine clearance (mL/min) | 74±16 | 73.8±14 | 90–150 |
| Serum creatinine (mg/dL) | 1.5±0.57 | 1.4±0.6 | 0.7–1.20 |
| C-reactive protein (mg/dL) | 1.6±2.5 | 1.5±2.1 | <0.50 |
Haematological parameters of the study population
| Parameter | Males (n=109) | Females (n=39) | Reference values |
|---|---|---|---|
| Hb (g/dL) | 11.1±1.04 | 10.5±0.98 | Males: 13–17 |
| Females: 12–16 | |||
| MCV (fL) | 86.2±9.8 | 84.5±10.4 | 83–97 |
| Reticulocytes (109/L) | 12.8±17.2 | 22±24.4 | 20–100 |
| Platelets (109/L) | 232±86.7 | 256±70 | 150–450 |
| Serum iron (µg/dL) | 64.3±31 | 57.6±28 | 60–150 |
| Transferrin saturation (%) | 22.4±13 | 16.8±9.4 | 15–45 |
| Serum ferritin (ng/mL) | 182±193 | 102±132 | Males: 15–250 |
| Females 10–150 | |||
| Soluble transferrin receptor (mg/L) | 2.2±0.3 | 2.5±1.58 | 0.83–1.76 |
| Serum erythropoietin (mU/mL) | 19.9±33 | 25.5±36.4 | 5–25 in non-anaemic subjects26 |
| EPO O/P ratio | 0.64±0.4 | 0.49±0.3 | 0.80–1.2026 |
| Serum urea (mg/dL) | 76.1±36 | 82.7±48 | 10–50 |
| Creatinine clearance (mL/min) | 74±16 | 73.8±14 | 90–150 |
| Serum creatinine (mg/dL) | 1.5±0.57 | 1.4±0.6 | 0.7–1.20 |
| C-reactive protein (mg/dL) | 1.6±2.5 | 1.5±2.1 | <0.50 |
| Parameter | Males (n=109) | Females (n=39) | Reference values |
|---|---|---|---|
| Hb (g/dL) | 11.1±1.04 | 10.5±0.98 | Males: 13–17 |
| Females: 12–16 | |||
| MCV (fL) | 86.2±9.8 | 84.5±10.4 | 83–97 |
| Reticulocytes (109/L) | 12.8±17.2 | 22±24.4 | 20–100 |
| Platelets (109/L) | 232±86.7 | 256±70 | 150–450 |
| Serum iron (µg/dL) | 64.3±31 | 57.6±28 | 60–150 |
| Transferrin saturation (%) | 22.4±13 | 16.8±9.4 | 15–45 |
| Serum ferritin (ng/mL) | 182±193 | 102±132 | Males: 15–250 |
| Females 10–150 | |||
| Soluble transferrin receptor (mg/L) | 2.2±0.3 | 2.5±1.58 | 0.83–1.76 |
| Serum erythropoietin (mU/mL) | 19.9±33 | 25.5±36.4 | 5–25 in non-anaemic subjects26 |
| EPO O/P ratio | 0.64±0.4 | 0.49±0.3 | 0.80–1.2026 |
| Serum urea (mg/dL) | 76.1±36 | 82.7±48 | 10–50 |
| Creatinine clearance (mL/min) | 74±16 | 73.8±14 | 90–150 |
| Serum creatinine (mg/dL) | 1.5±0.57 | 1.4±0.6 | 0.7–1.20 |
| C-reactive protein (mg/dL) | 1.6±2.5 | 1.5±2.1 | <0.50 |
Cytokine profile in anaemia of chronic disease patients
| Variables (pg/mL) | Patients (n=85) | Healthy subjects (reference values, n=40)28 |
|---|---|---|
| TNF-α | 40.6±11.6 | 18.2±4 |
| sTNFR-I | 3052±1438 | 978±775 |
| sTNFR-II | 4647±2339 | 1947±1403 |
| IL-6 | 19.6±24.9 | 4.3±8 |
| IL-1Ra | 613±623 | 224±112 |
| Variables (pg/mL) | Patients (n=85) | Healthy subjects (reference values, n=40)28 |
|---|---|---|
| TNF-α | 40.6±11.6 | 18.2±4 |
| sTNFR-I | 3052±1438 | 978±775 |
| sTNFR-II | 4647±2339 | 1947±1403 |
| IL-6 | 19.6±24.9 | 4.3±8 |
| IL-1Ra | 613±623 | 224±112 |
Cytokine profile in anaemia of chronic disease patients
| Variables (pg/mL) | Patients (n=85) | Healthy subjects (reference values, n=40)28 |
|---|---|---|
| TNF-α | 40.6±11.6 | 18.2±4 |
| sTNFR-I | 3052±1438 | 978±775 |
| sTNFR-II | 4647±2339 | 1947±1403 |
| IL-6 | 19.6±24.9 | 4.3±8 |
| IL-1Ra | 613±623 | 224±112 |
| Variables (pg/mL) | Patients (n=85) | Healthy subjects (reference values, n=40)28 |
|---|---|---|
| TNF-α | 40.6±11.6 | 18.2±4 |
| sTNFR-I | 3052±1438 | 978±775 |
| sTNFR-II | 4647±2339 | 1947±1403 |
| IL-6 | 19.6±24.9 | 4.3±8 |
| IL-1Ra | 613±623 | 224±112 |
References
Pina IL, Apstein CS, Balady GJ, Belardinelli R, Chaitman BR, Duscha BD, Fletcher BJ, Fleg JL, Myers JN, Sullivan MJ; American Heart Association Committee on exercise, rehabilitation, and prevention. Exercise and heart failure: a statement from the American Heart Association Committee on exercise, rehabilitation, and prevention.
Komajda M. Prevalence of anaemia in patients with chronic heart failure and their clinical characteristics.
Anand I, McMurray JJ, Whitmore J, Warren M, Pham A, McCamish MA, Burton PB. Anaemia and its relationship to clinical outcome in heart failure.
Horwich TB, Fonarow GC, Hamilton MA, MacLellan WR, Borenstein J. Anemia is associated with worse symptoms, greater impairment in functional capacity and a significant increase in mortality in patients with advanced heart failure.
McClellan WM, Flanders WD, Langston RD, Jurkovitz C, Presley R. Anemia and renal insufficiency are independent risk factors for death among patients with congestive heart failure admitted to community hospitals: a population-based study.
Kosiborod M, Smith GL, Radford MJ, Foody JM, Krumholz HM. The prognostic importance of anemia in patients with heart failure.
Ezekowitz JA, McAlister FA, Armstrong PW. Anemia is common in heart failure and is associated with poor outcomes: insights from a cohort of 12065 patients with new-onset heart failure.
Sharma R, Francis DP, Pitt B, Poole-Wilson PA, Coats AJ, Anker SD. Haemoglobin predicts survival in patients with chronic heart failure: a substudy of the ELITE II trial.
Felker GM, Gattis WA, Leimberger JD, Adams KF, Cuffe MS, Gheorghiade M, O'Connor CM. Usefulness of anemia as a predictor of death and rehospitalization in patients with decompensated heart failure.
Al-Ahmad A, Rand WM, Manjunath G, Konstam MA, Salem DN, Levey AS, Sarnak MJ. Reduced kidney function and anemia as risk factors for mortality in patients with left ventricular dysfunction.
Mozaffarian D, Nye R, Levy WC. Anemia predicts mortality in severe heart failure: the prospective randomized amlodipine survival evaluation (PRAISE).
Silverberg DS, Wexler D, Laina A. The importance of anemia and its correction in the management of severe congestive heart failure.
Silverberg DS, Wexler D, Blum M, Keren G, Sheps D, Leibovitch E, Brosh D, Laniado S, Schwartz D, Yachnin T, Shapira I, Gavish D, Baruch R, Koifman B, Kaplan C, Steinbruch S, Iaina A. The use of subcutaneous erythropoietin and intravenous iron for the treatment of the anemia of severe, resistant congestive heart failure improves cardiac and renal function and functional cardiac class, and markedly reduces hospitalizations.
Silverberg DS, Wexler D, Sheps D, Blum M, Keren G, Baruch R, Schwartz D, Yachnin T, Steinbruch S, Shapira I, Laniado S, Iaina A. The effect of correction of mild anemia in severe, resistant congestive heart failure using subcutaneous erythropoietin and intravenous iron: a randomized controlled study.
Mancini DM, Katz SD, Lang CC, LaManca J, Hudaihed A, Androne AS. Effect of erythropoietin on exercise capacity in patients with moderate to severe chronic heart failure.
Cromie N, Lee C, Struthers AD. Anemia in chronic heart failure: what is the frequency in the UK and its underlying causes?
Okonko D, Ankers S. Anemia in chronic heart failure: pathogenetic mechanisms.
Kalra PR, Collier T, Cowie MR, Fox KF, Wood DA, Poole-Wilson PA, Coats AJ, Sutton GC. Haemoglobin concentration and prognosis in new cases of heart failure.
Remme WJ, Swedberg K. Task force of the diagnosis and treatment of chronic heart failure, European Society of Cardiology. Guidelines for the diagnosis and treatment of chronic heart failure.
Cockcroft DW, Gault MH. Prediction of creatinine clearance from serum creatinine.
Beguin Y, Clemons GK, Pootrakul P, Fillet G. Quantitative assessment of erythropoiesis and functional classification of anemia based on measurements of serum transferrin receptor and erythropoietin.
Cazzola M, Beguin Y. New tools for clinical evaluation of erythron function in man.
Cazzola M, Ponchio L, de Benedetti F, Ravelli A, Rosti V, Beguin Y, Invernizzi R, Barosi G, Martini A. Defective iron supply for erythropoiesis and adequate endogenous erythropoietin production in the anemia associated with systemic-onset juvenile chronic arthritis.
Cazzola M, Guarnone R, Cerani P, Centenara E, Rovati A, Beguin Y. Red blood cell precursor mass as an independent determinant of serum erythropoietin level.
Cerutti A, Custodi P, Duranti M, Cazzola M, Balduini CL. Circulating thrombopoietin in reactive conditions behaves like an acute phase reactant.
Valgimigli M, Agnoletti L, Curello S, Comini L, Francolini G, Mastrorilli F, Merli E, Pirani R, Guardigli G, Grigolato PG, Ferrari R. Serum from patients with acute coronary syndromes displays a proapoptotic effect on human endothelial cells: a possible link to pan-coronary syndromes.
Androne AS, Katz SD, Lund L, LaManca J, Hudaihed A, Hryniewicz K, Mancini DM. Hemodilution is common in patients with advanced heart failure.
Witte KK, Desilva R, Chattopadhyay S, Ghosh J, Cleland JG, Clark AL. Are hematinic deficiencies the cause of anemia in chronic heart failure?
Tefferi A. Anemia in adults: a contemporary approach to diagnosis.
Cazzola M, Mercuriali F, Brugnara C. Use of recombinant human erythropoietin outside the setting of uremia.
Faquin WC, Schneider TJ, Goldberg MA. Effect of inflammatory cytokines on hypoxia-induced erythropoietin production.
van der Meer P, Voors AA, Lipsic E, Smilde TD, van Gilst WH, van Veldhuisen DJ. Prognostic value of plasma erythropoietin on mortality in patients with chronic heart failure.
Ganz T. Hepcidin, a key regulator of iron metabolism and mediator of anemia of inflammation.
Martini A, Ravelli A, Di Fuccia G, Rosti V, Cazzola M, Barosi G. Intravenous iron therapy for severe anaemia in systemic-onset juvenile chronic arthritis.
Thomas C, Thomas L. Biochemical markers and hematologic indices in the diagnosis of functional iron deficiency.
Plata R, Cornejo A, Arratia C, Anabaya A, Perna A, Dimitrov BD, Remuzzi G, Ruggenenti P. Commission on Global Advancement of Nephrology (COMGAN), Research Subcommittee of the International Society of Nephrology. Angiotensin-converting-enzyme inhibition therapy in altitude polycythaemia: a prospective randomised trial.
Chatterjee B, Nydegger UE, Mohacsi P. Serum erythropoietin in heart failure patients treated with ACE-inhibitors or AT1 antagonists.


{kind=link}